Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_016
Taming the Stone: Successful PCI of Heavily Calcified LAD Using Rotablator and Intravascular Lithotripsy (IVL)
By Praise Jeremiah, Hua Yan
Presenter
Praise Jeremiah
Authors
Praise Jeremiah1, Hua Yan2
Affiliation
Wuhan Asia Heart Hospital, Indonesia1, Wuhan Asia Heart Hospital, China2
View Study Report
CASE20251106_016
Coronary - Complex PCI - Left Main
Taming the Stone: Successful PCI of Heavily Calcified LAD Using Rotablator and Intravascular Lithotripsy (IVL)
Praise Jeremiah1, Hua Yan2
Wuhan Asia Heart Hospital, Indonesia1, Wuhan Asia Heart Hospital, China2
Clinical Information
Relevant Clinical History and Physical Exam
A 85-year-oldmale presented with intermittent chest tightness and dyspnea for one month,worsening over the past two weeks, particularly at night and relieved bysitting up. He is on hemodialysis for 4 years, had paroxysmal AF, had historyof DVT and PE. Vital signs were normal,but upon he had coarse breath sounds bilaterally with crackles at the lung bases,cardiomegaly, and 2/6 systolic murmur at the apex.
Relevant Test Results Prior to Catheterization
Echocardiographyshowed aortic valve calcification with mild AR and AS, severe MR, moderate TR,and pulmonary hypertension.
Relevant Catheterization Findings
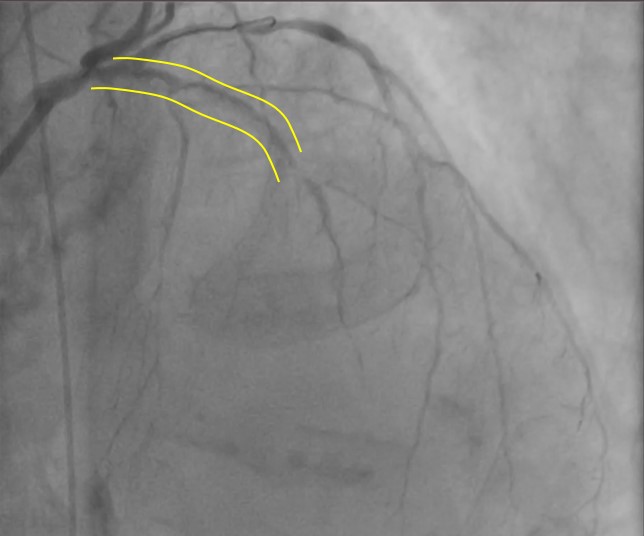
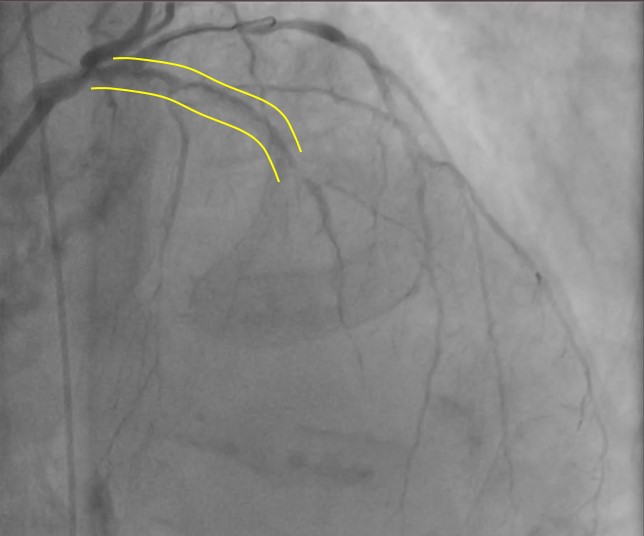
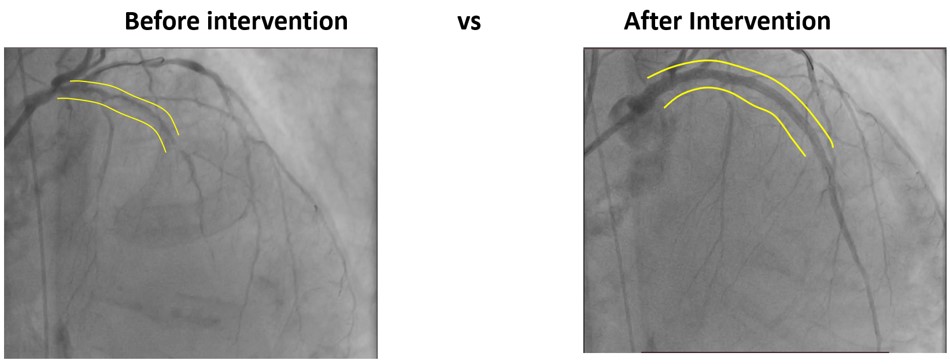
Coronaryangiography revealed diffuse calcified lesion in the LM at bifurcation with 70%stenosis, 99% stenosis at proximal LAD, and 99% stenosis at mid-LAD. Thepatient was diagnosed as CAD, UAP, Heart failure class II NYHA.
Interventional Management
Procedural Step
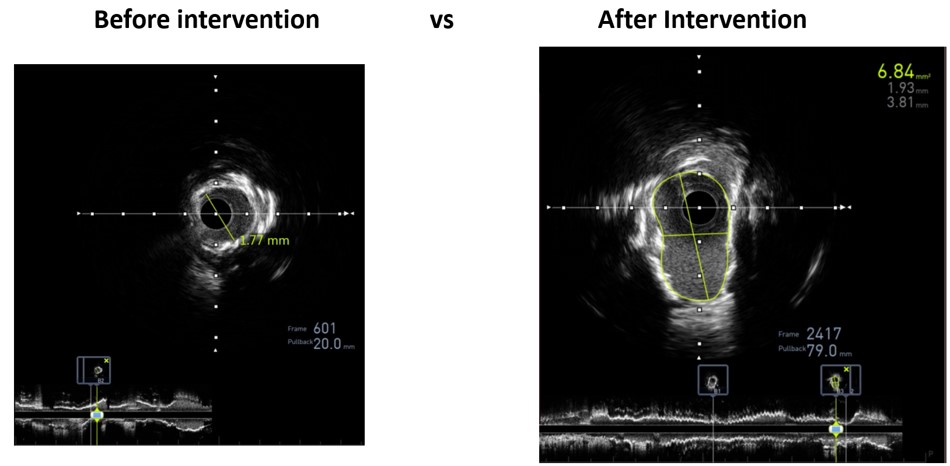
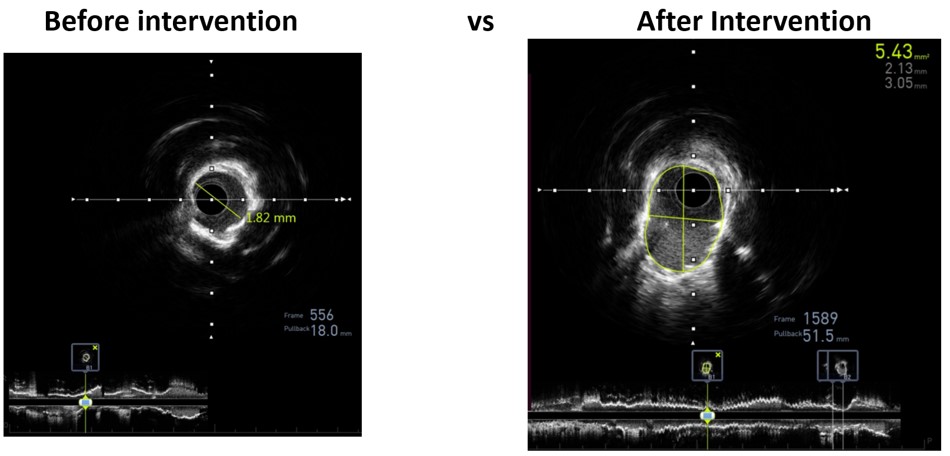
Through radial artery access, guiding catheter 1 (7F/EBU3.75) was inserted into the distal LAD. Guidewire 1 (Asahi Sion Blue) and guidewire 2 (Abbott) was unable to reach distal LAD segment and the distal D segment. Balloon 1 (1.0x10 mm, 8 atm) could not pass proximal LAD when sent along the guidewire 1. IVUS of the LAD-LM showed diffuse calcification with >2700 circular arc. Rotational atherectomy was targeted to distal LAD. High-speed rotational atherectomy and low-speed plaque modification was performed on proximal-mid LAD lesions. Then, guidewire 1 (Asahi Sion Blue) was advance to distal LAD. IVUS on LAD-LM revealed circumferential calcification. Intravascular shockwave energy was used to inflate the balloon (3.0 x 12 mm shockwave balloon) at 4-6 atm and then IVUS showed a rupture of deep LAD calcified ring. Then, the distal LAD was predilated [Balloon 2 (1.5x20 mm, 6-12 atm), balloon 3 (2.0x20mm, 6-12 atm), balloon 4 (2.0x20 mm, 6-12 atm) and balloon 5 (NC balloon 2.0x20 mm, 20 atm)]. Stent 1 (DES 2.25x23 mm, 9 atm), stent 2 (DES 2.75x30 mm, 9 atm), stent 3 (DES 3.00x30 mm, 9 atm), stent 4 (DES 3.50x 28mm, 9 atm) was planted on the mid LM-LAD segment and then balloon 6-10 (PTCA ballon 2.75 x12mm, 14-28 atm); (PTCA ballon 3.00x 12mm, 14-28 atm); (PTCA ballon 3.00x15 mm, 14-28 atm); (NC balloon 3.00 mm x 15 mm, 14-28 atm); (coronary mastoid 3.00x15 mm , 14-28 atm) was planted for post dillatation. Post procedural IVUS showed satisfactory result.
Case Summary
Complex calcified LAD lesions can be successfully treated with combined Rotational atherectomy with intravenous lithotripsy (IVL) to manipulate the heavily calcified lesion. Ensuring optimal stent expansion can lead to long-term procedural success.