Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_014
Successful Tip Detection Antegrade Dissection and Reentry Using Ultrasound for Vintage Chronic Total Occlusion
By Tetsuya Takahashi
Presenter
Tetsuya Takahashi
Authors
Tetsuya Takahashi1
Affiliation
Japanese Red Cross Ishinomaki Hospital, Japan1
View Study Report
CASE20251106_014
Coronary - Complex PCI - CTO
Successful Tip Detection Antegrade Dissection and Reentry Using Ultrasound for Vintage Chronic Total Occlusion
Tetsuya Takahashi1
Japanese Red Cross Ishinomaki Hospital, Japan1
Clinical Information
Relevant Clinical History and Physical Exam
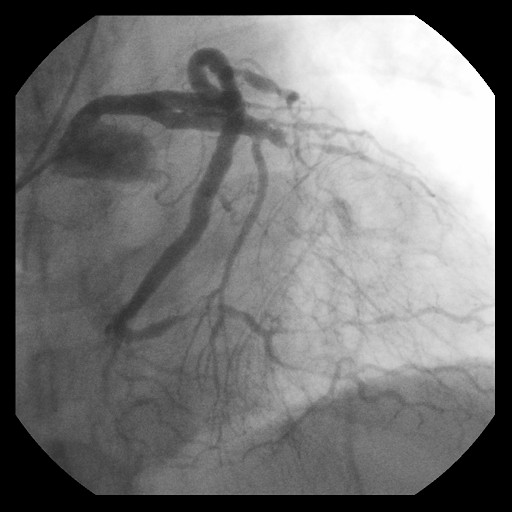
A 60-year-old man underwent percutaneous coronary intervention (PCI) for chronic total occlusion (CTO) of left anterior descending coronary (LAD) 9-years ago. However, the CTO PCI failed because the guide wire advanced into extra plaque. Because he presented with shortness of breath, which was thought to be due to coronary artery disease, we re-attempted PCI for LAD CTO.

Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
Interventional Management
Procedural Step
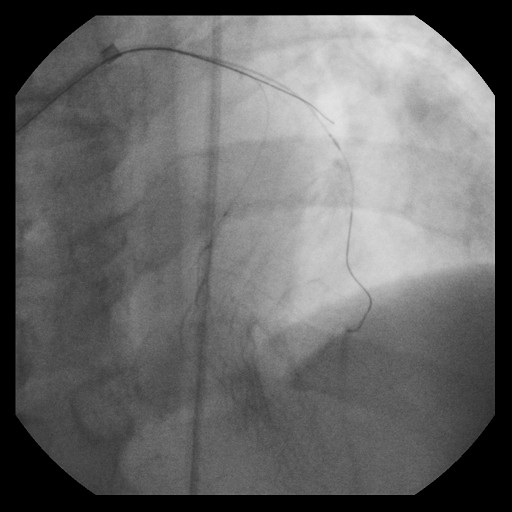
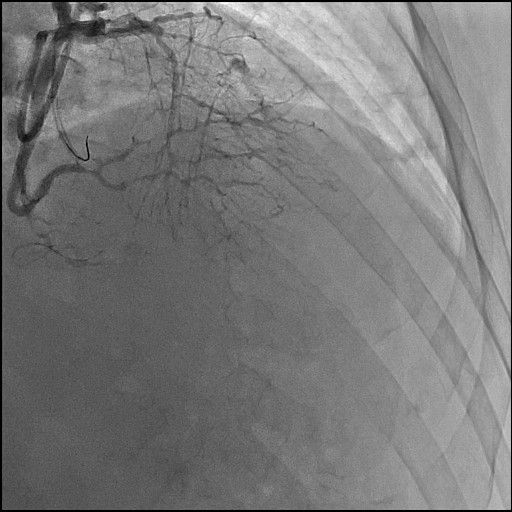
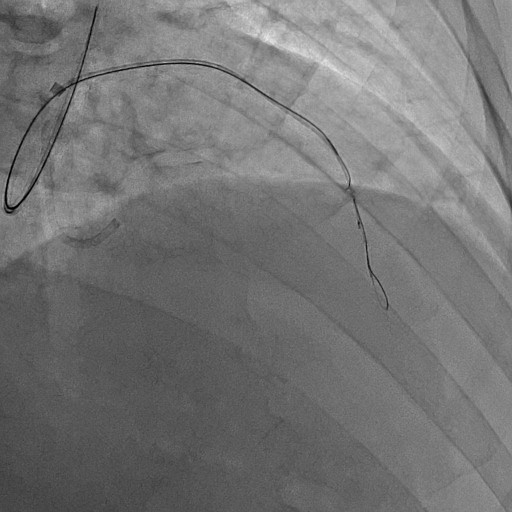
Re-attempted PCI for LAD CTO was planned. The procedure was performed with an 8-Fr, SPB 3.5 SH for the antegrade approach and a 6-Fr IMA for retrograde angiography. Primary antegrade approach was performed because there were no feasible collateral channels. Gaia Next 3 could penetrate the proximal cap of CTO. Since Gaia Next3 could not proceed into the CTO mid portion, the guide wire was escalated to Gaia Next 4. However, Gaia Next 4 advanced into extra plaque space beyond the CTO distal true lumen angiographically. Therefore, we decided to perform tip-detection (TD) method using intravascular ultrasound (IVUS). IVUS revealed that the guide wire proceeded into extra plaque from the CTO proximal portion, although the CTO entry was in the intra plaque space. At first, we tried TD-intra plaque tracking (IPT) in the CTO body. However, Conquest Pro 12 ST (CP-12ST) could not penetrate the CTO body. Therefore, we performed TD-antegrade dissection andreentry (ADR). Eventually, CP12 ST succeeded to puncture the distal true lumen supported by a Caravel. We implanted a drug-eluting stent, which resulted in successful revascularization.
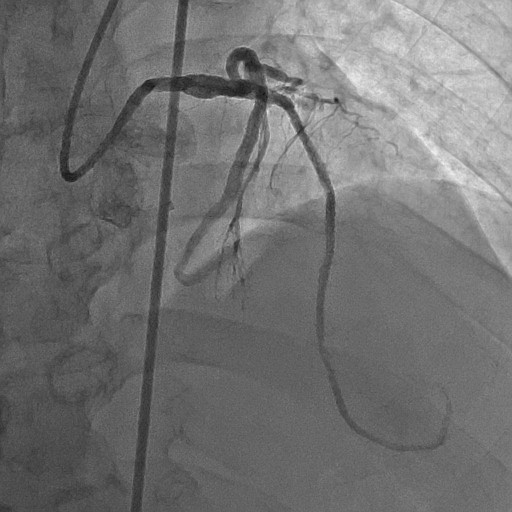
Case Summary
Recently, TD-ADR has been established as a novel PCI technology in CTO. We successfully revascularized a vintage hard CTO lesion using TD-ADR. TD-ADR is suitable treatment option in CTO PCI if there are no feasible collateral channels.