Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_012
Missed Ostium in PCI: Failure or Blind Intervention?
By Nazim Megherbi
Presenter
Nazim Megherbi
Authors
Nazim Megherbi1
Affiliation
King Abdulaziz Specialist Hospital, Sakaka, Saudi Arabia1
View Study Report
CASE20251106_012
Coronary - Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
Missed Ostium in PCI: Failure or Blind Intervention?
Nazim Megherbi1
King Abdulaziz Specialist Hospital, Sakaka, Saudi Arabia1
Clinical Information
Relevant Clinical History and Physical Exam
A 47-year-old diabetic, hypertensive man with chronic renal failure presented with NSTEMI (Killip II). He had prior LAD mid angioplasty for anterior STEMI, LCx angioplasty for stable angina, and LAD proximal angioplasty.
Relevant Test Results Prior to Catheterization
ECG showed lateral changes, LVEF 35%, elevated troponin, creatinine clearance 34.
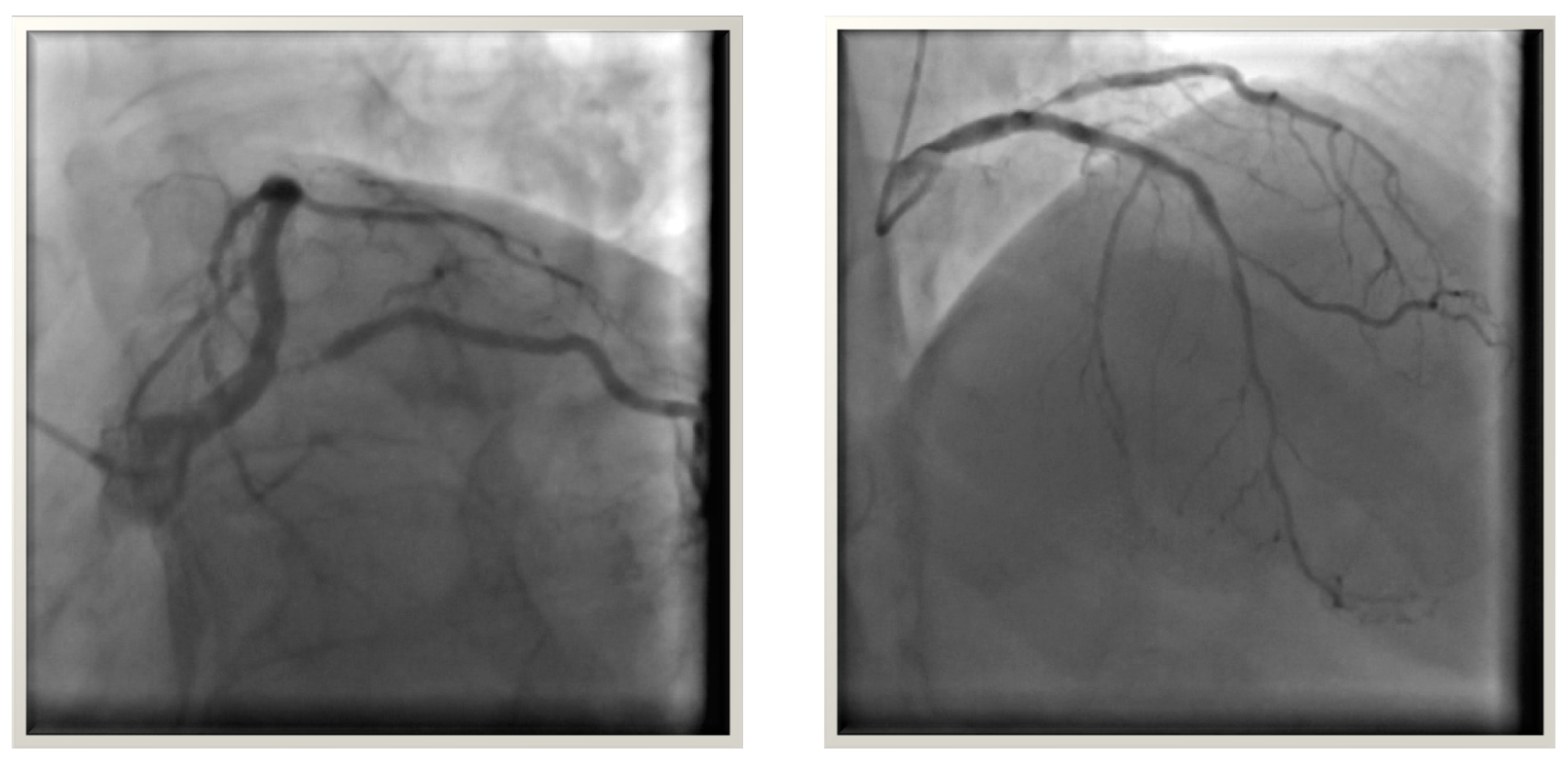
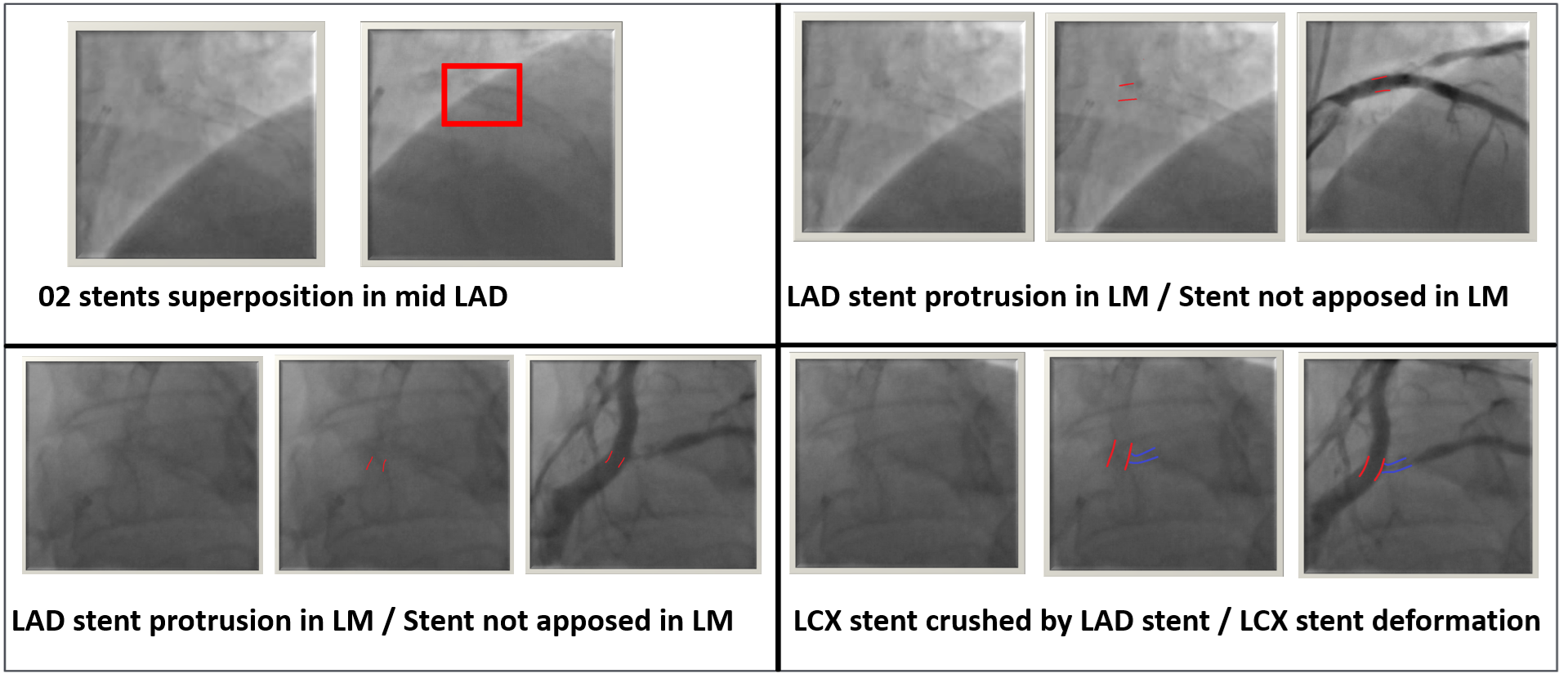
Relevant Catheterization Findings
Coronary angiography revealed severe LCx ostial severe in-stent restenosis due to a crushed stent from proximal LAD stent protrusion into the LM. Patient developed contrast induced nephropathy after coronary angiography.
Interventional Management
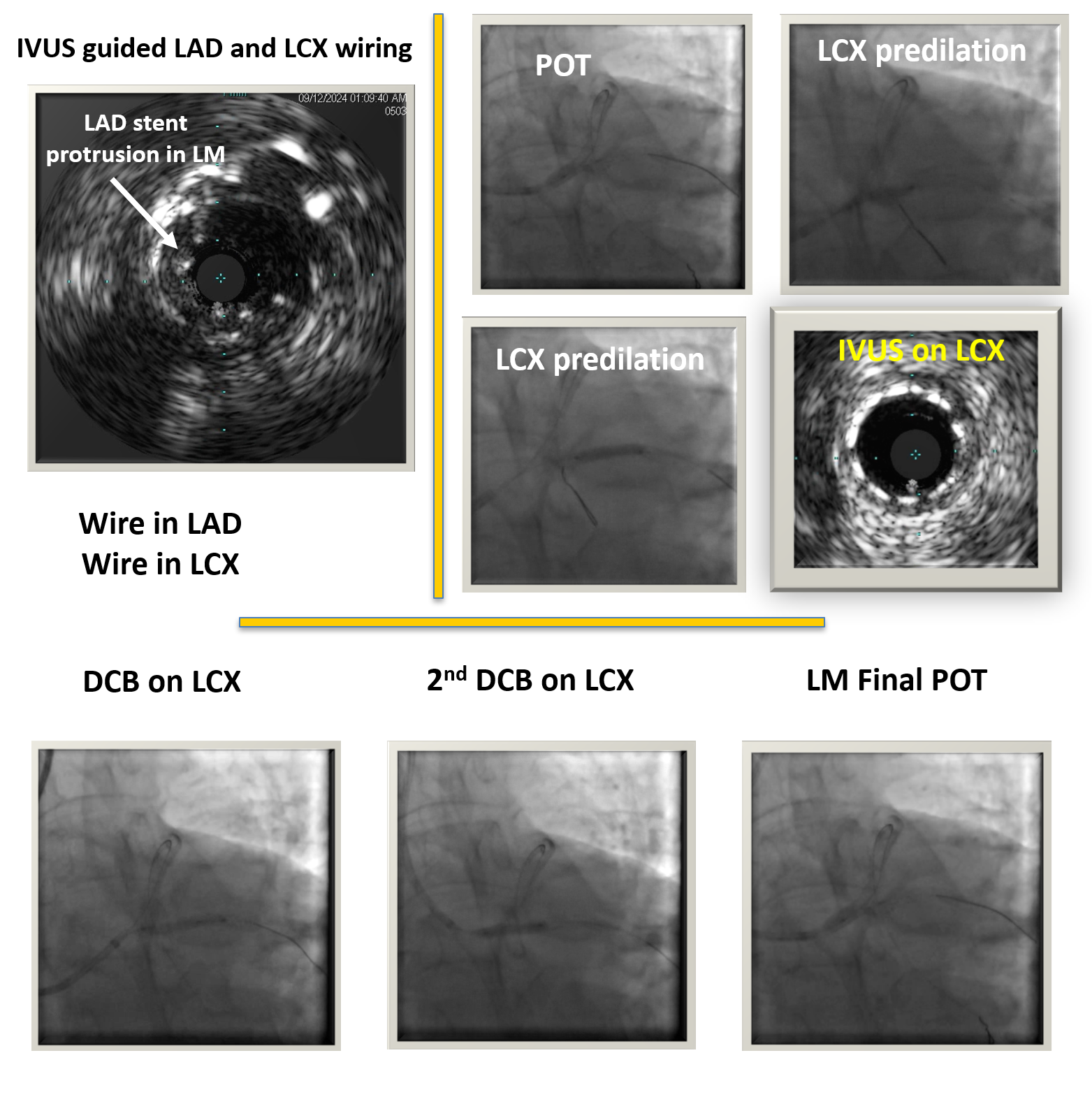
Procedural Step
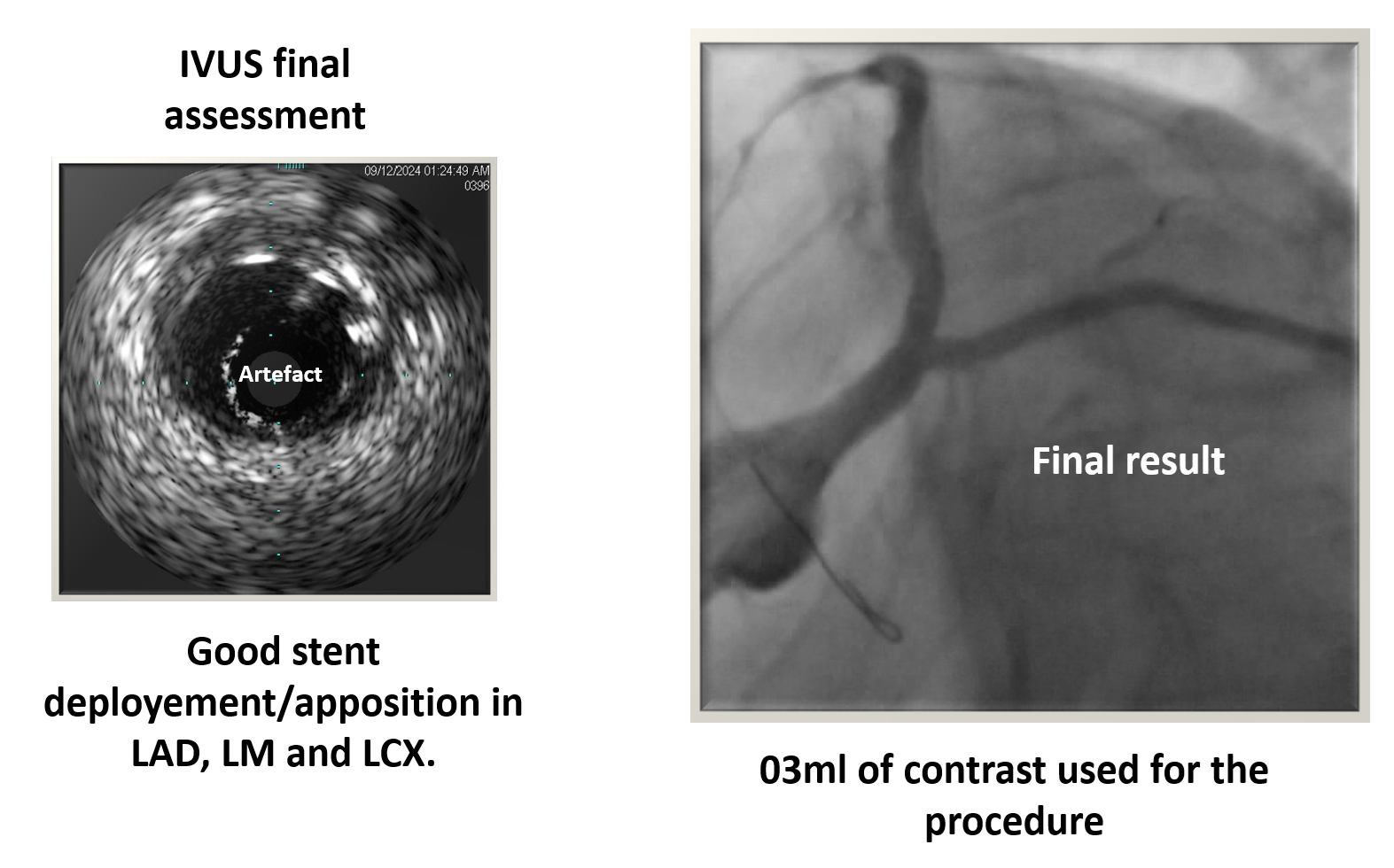
Challenges in this complex case included the risk of contrast-induced nephropathy, crossing the left main while avoiding floating struts of the LAD stent, and crossing to the LCx while avoiding the deformed LCx stent struts. IVUS-guided angioplasty was performed. Two guidewires were positioned intrastent: one in the LAD and one in the LCx through the protruding stent struts in the left main. After predilation of the LCx and POT on the left main under IVUS guidance, a drug-coated balloon was applied to the LCx. The procedure was finalized with a final POT on the left main. Final IVUS and angiography confirmed an excellent result. Total contrast used was 03 ml.
Case Summary
For ostial stenosis of the LAD or LCx, PCI can be limited to the ostium if guided by intravascular imaging, if favorable Medina classification, an adequate proximal landing zone, and careful consideration of the bifurcation angle. In cases left main PCI, in-stent restenosis or crushed stents, IVUS or OCT is essential for anatomical assessment, procedural planning, guidance, and result evaluation. Drug-coated balloons was particularly valuable in managing our complex lesions.