Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_010
From Setback to Success: Rescue Conversion of Left Main Bifurcation Intervention in Acute ST-Elevation Myocardial Infarction From Failed Provisional and T-and-Protrusion With Thrombosis to Final Reverse Double Kissing Crush
By Nattapong Thaiyanurak, Thanyalak Chotayaporn, Noparat Oniem, Noparat Thanachaikun
Presenter
Nattapong Thaiyanurak
Authors
Nattapong Thaiyanurak1, Thanyalak Chotayaporn1, Noparat Oniem1, Noparat Thanachaikun1
Affiliation
Nakornping Hospital, Thailand1
View Study Report
CASE20251106_010
Coronary - Complex PCI - Bifurcation
From Setback to Success: Rescue Conversion of Left Main Bifurcation Intervention in Acute ST-Elevation Myocardial Infarction From Failed Provisional and T-and-Protrusion With Thrombosis to Final Reverse Double Kissing Crush
Nattapong Thaiyanurak1, Thanyalak Chotayaporn1, Noparat Oniem1, Noparat Thanachaikun1
Nakornping Hospital, Thailand1
Clinical Information
Relevant Clinical History and Physical Exam
A 65-year-old Thai male with hypertension presented to the emergency department with acute chest pain and dyspnea. The ECG revealed anterolateral ST-segment elevation, new right bundle branch block, and atrial fibrillation. The emergency physician activated the primary PCI protocol. Prior to transfer to the cath lab, the patient was intubated using rapid sequence induction, and intravenous furosemide was administered. Aspirin and ticagrelor were loaded for dual antiplatelet therapy.

Relevant Test Results Prior to Catheterization
- Echo: LVEF 26.9%, akinesia at anterior, anterosepal & anteroseptal wall from basal to apical LV, no significant valvular heart disease, no intracardiac mass or thrombus- Serum creatinine 1.28 mg/dL (eGFR 55.4 ml/min/1.73sqm)
 echo1.mp4
echo1.mp4
PSAX2.mp4
Relevant Catheterization Findings
Coronary angiogram (Access site: RRA 6F sheath, Tiger 4.0 5F diagnostic catheter)
RAO CAU.mp4
Spider.mp4
RCA2.mp4
Interventional Management
Procedural Step
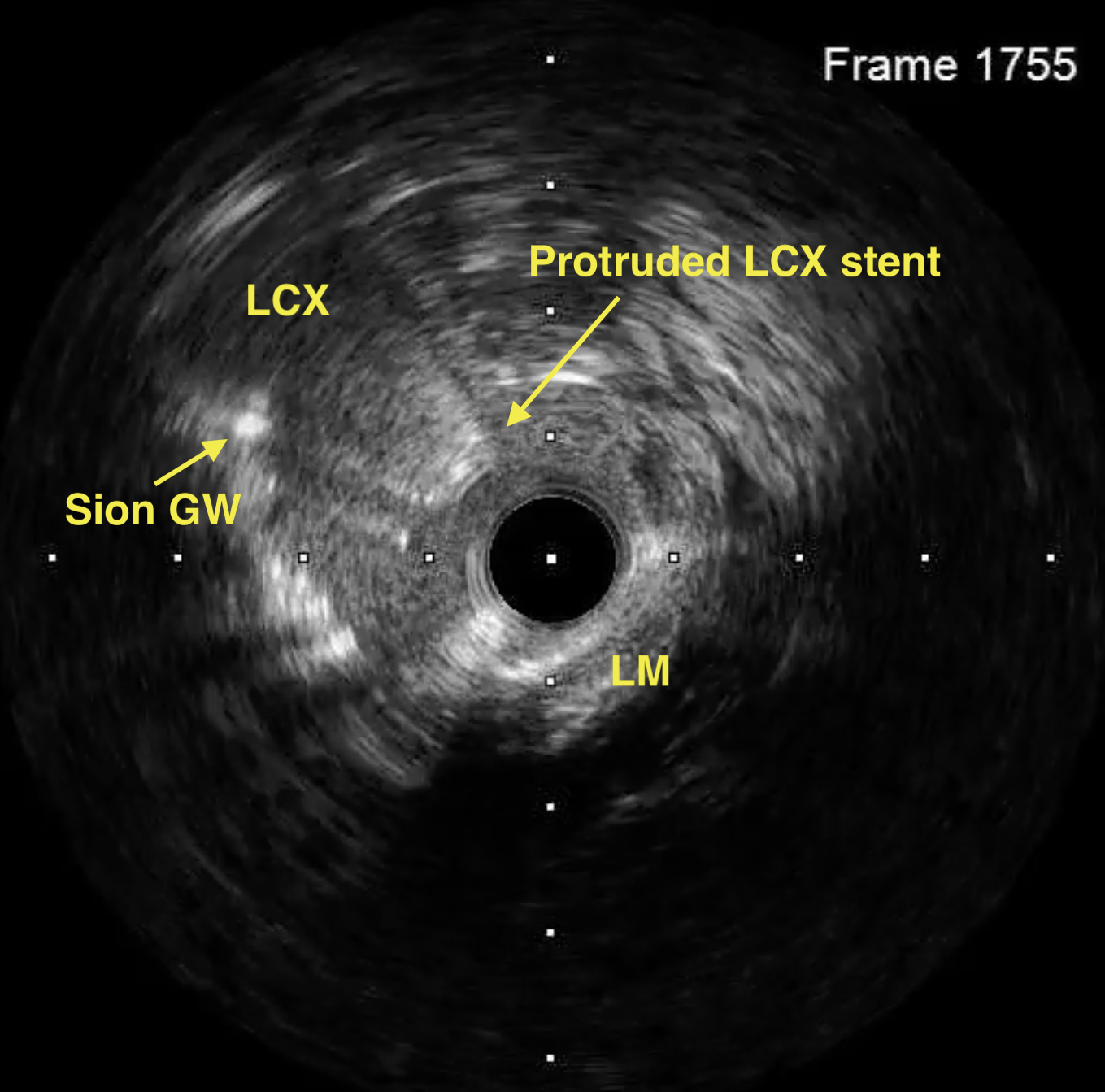
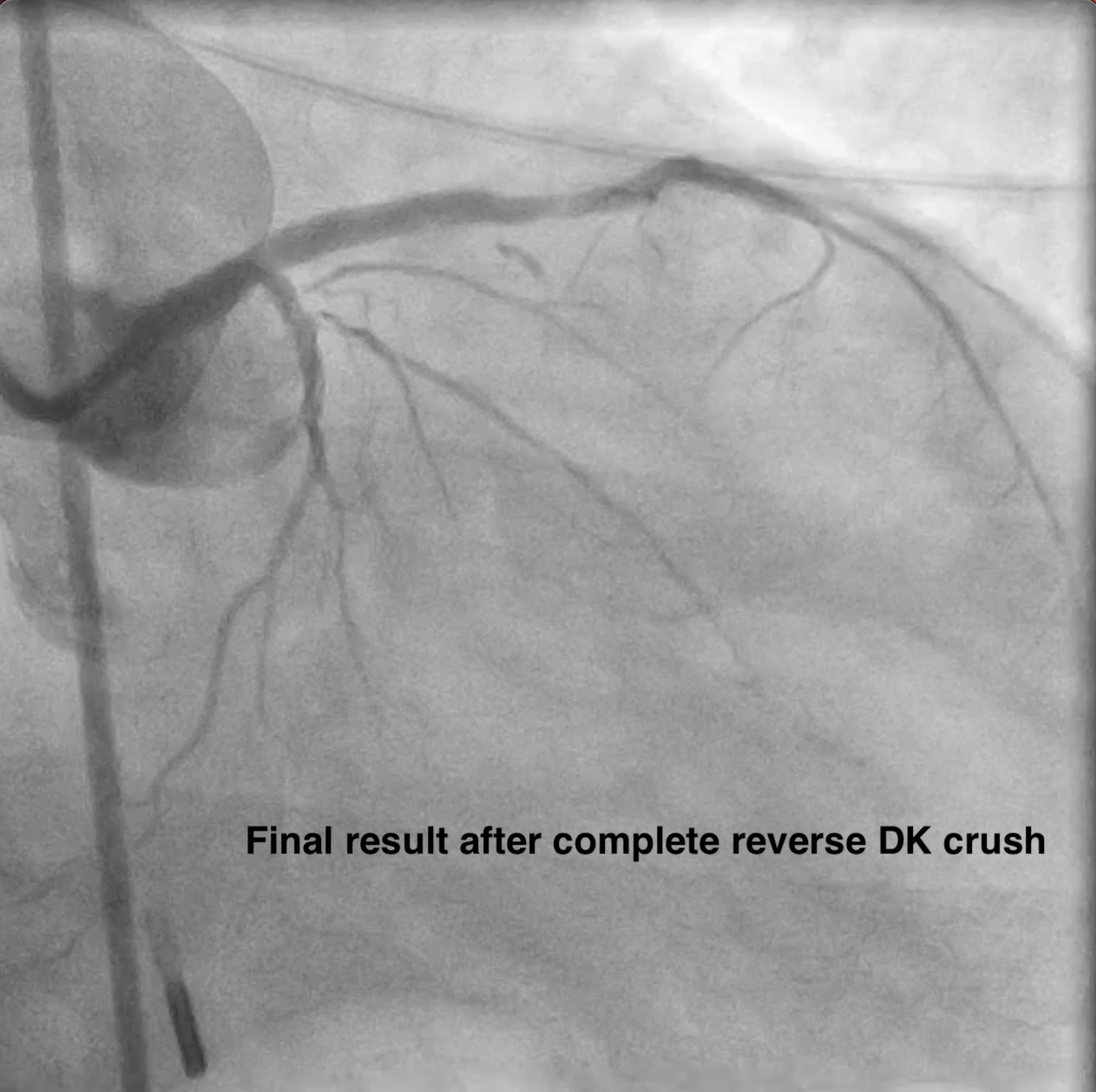
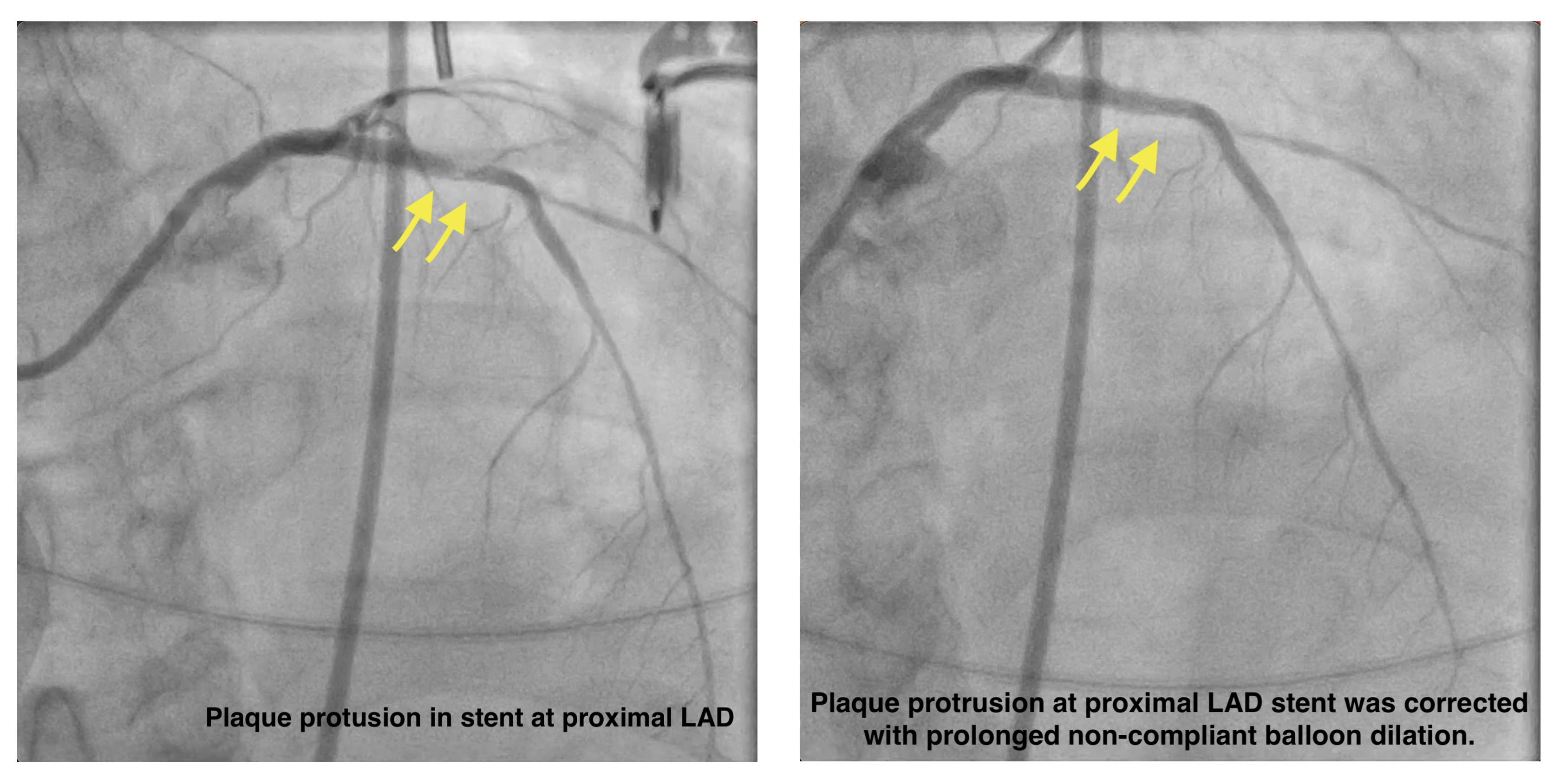
Access site: RRA 6F sheath, EBU 3.5 6F guiding catheter. IABP was inserted via RFA for hemodynamic support. A BMW guidewire (GW) was advanced into the LAD, & thrombus was aspirated. A Sion GW was then placed in LCX. IVUS guided a provisional strategy from LM to LAD restoring flow quickly. The lesion was pre-dilated with a 2.0 × 20 mm balloon & a 2.5 × 10 mm scoring balloon. Biomatrix Alpha stents (3.5 × 36 mm & 2.5 × 24 mm) were deployed from the LM to mid LAD & post-dilated. The LCX became jailed, so the T-and-Protrusion technique was initiated as a bailout, & a Biomatrix Alpha 2.5 × 19 mm stent was positioned for TAP. After TAP, acute thrombosis developed at the neocarina of the LM. The patient received adequate heparin, intracoronary eptifibatide, & vasopressors. The procedure was stopped after achieving TIMI 3 flow in LAD & resolution of ST elevation. The patient was transferred to the ICU for intensive antithrombotic therapy. 3 days later, a relook angiogram via the LFA (EBU 3.5 7F) showed total LCX occlusion. IVUS confirmed excessive LCX stent protrusion into LM. Reverse Double Kissing Crush was performed. The protruded LCX stent was crushed with a 4.0 × 12 mm non-compliant balloon, Sion Blue GW was advanced through the proximal strut, & final kissing inflation with proximal optimization was completed. Plaque protrusion at proximal LAD stent was corrected with prolonged NC balloon dilation. Final IVUS & angiography showed good result.
jailed LCX.mp4
Thrombosis after TAP.mp4
Relook CAG.mp4
Case Summary
◆ In high-risk left main bifurcation intervention during STEMI, a provisional stenting strategy may fail when the side branch is significantly compromised.