Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_006
Reverse Controlled Antegrade and Retrograde Tracking to Salvage Inadvertent Subintimal Stenting
By Bryan Rene Toledano, Jose Paolo Prado, Jeffrey Chua
Presenter
Bryan Rene Toledano
Authors
Bryan Rene Toledano1, Jose Paolo Prado1, Jeffrey Chua1
Affiliation
The Medical City, Philippines1
View Study Report
CASE20251106_006
Coronary - Complication Management
Reverse Controlled Antegrade and Retrograde Tracking to Salvage Inadvertent Subintimal Stenting
Bryan Rene Toledano1, Jose Paolo Prado1, Jeffrey Chua1
The Medical City, Philippines1
Clinical Information
Relevant Clinical History and Physical Exam
A 42-year-old male presented with exertional angina. He has known two-vessel coronary artery disease with prior successful percutaneous coronary intervention to the right coronary artery. He was referred to our center after an unsuccessful chronic total occlusion intervention of the left anterior descending artery complicated by inadvertent subintimal stenting. On evaluation, he was hemodynamically stable with an unremarkable cardiopulmonary examination.
Relevant Test Results Prior to Catheterization
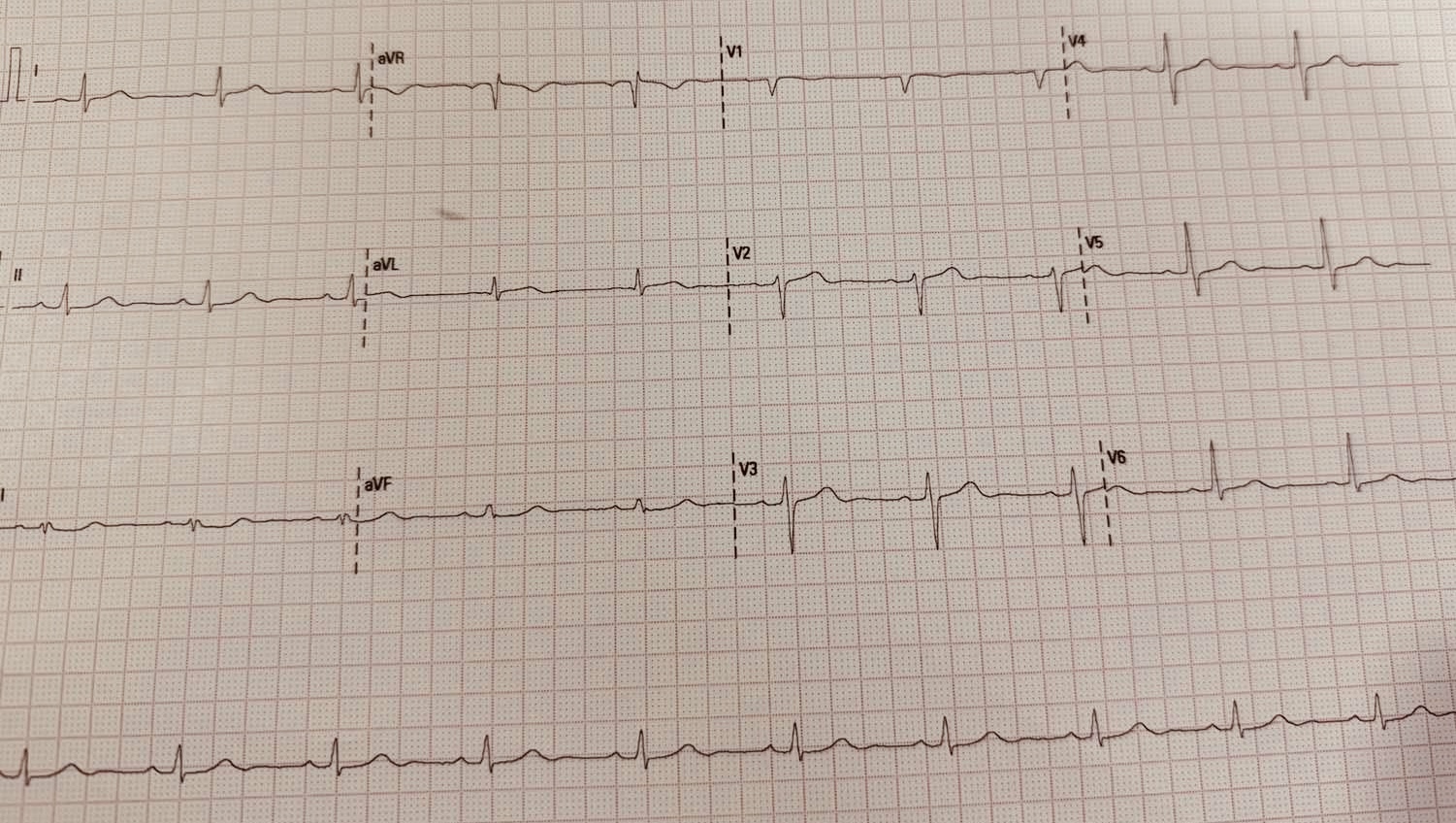
12-lead ECG demonstrated normal sinus rhythm without acute ischemic changes. Transthoracic echocardiography showed regional wall motion abnormality localized to the anteroseptal segment with preserved global systolic function (LVEF ≈55%).
Relevant Catheterization Findings
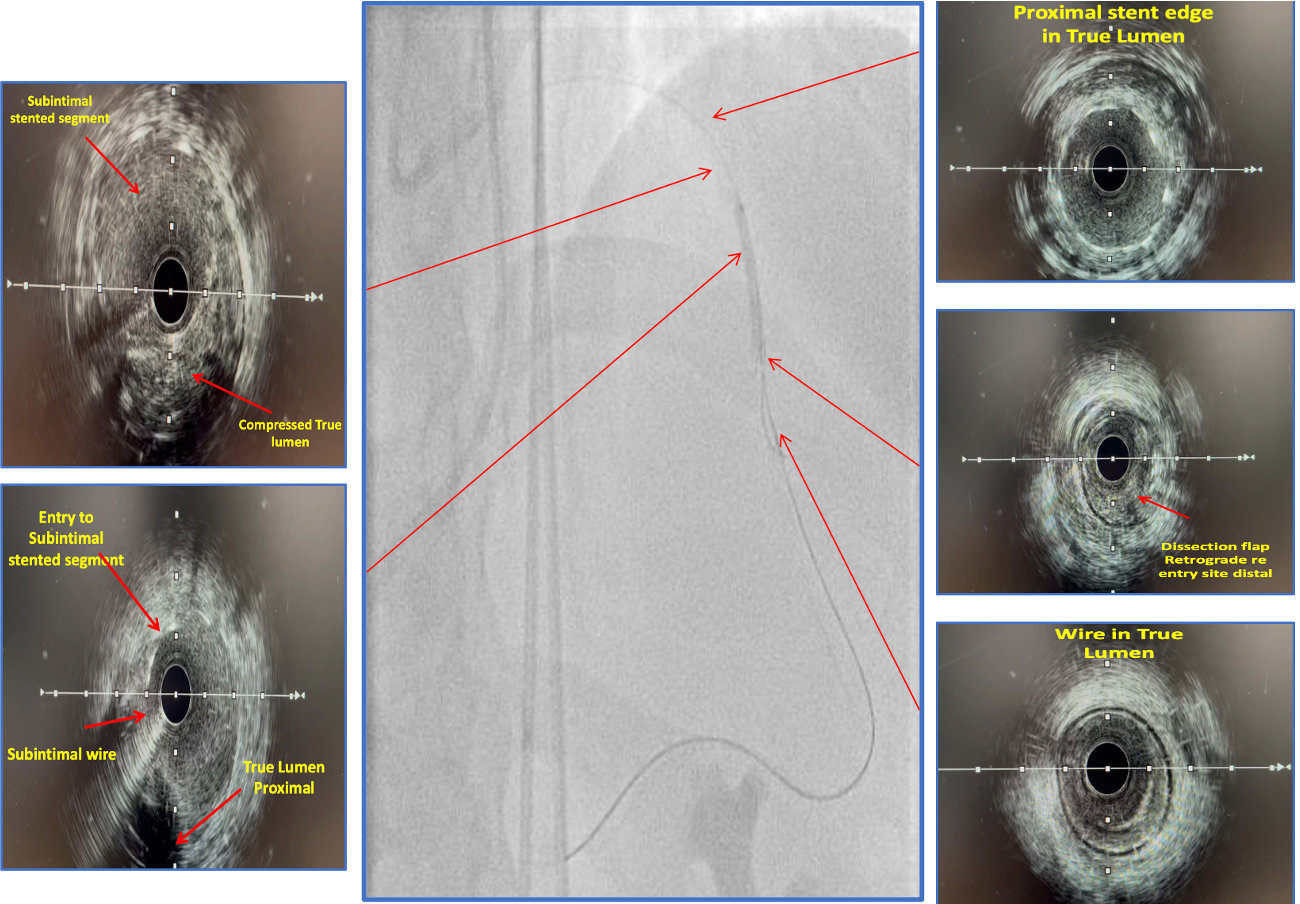
Diagnostic angiography demonstrated a borderline ostial LAD lesion followed by a proximal LAD CTO. The proximal edge of the previously deployed stent remained in the true lumen, while the majority of the stented segment tracked the subintimal plane with absent distal flow. The Left circumflex was without significant disease. The previously stented RCA was widely patent. Dual injections identified well-developed RCA-to-LAD collaterals
 3.mp4
3.mp4
7.mp4
8.mp4
Interventional Management
Procedural Step
Bilateral femoral arterial access was obtained using 7F sheaths. The left main and RCA were engaged with 7F EBU 3.5 and JR 4 guide catheters, respectively. Antegrade CTO strategies were performed initially. Wire escalation with Gaia 3rd and Conquest Pro 12 supported by a Caravel microcatheter was attempted, followed by a parallel wire technique using a Sasuke dual-lumen microcatheter. Subsequently, antegrade fenestration and re-entry was attempted using a Corsair Pro and short balloon inflations. Despite multiple efforts, true lumen passage could not be re-established, and the antegrade strategy was abandoned. A retrograde approach was then employed. Attempts to cross septal collaterals from the RPDA and diagonal collaterals from the OM were unsuccessful. A contralateral epicardial collateral from the RCA marginal branch allowed successful retrograde advancement using a Suoh 3 wire with Caravel support. Reverse CART was executed by inflating a 3.0 × 20 mm balloon within the subintimal stented plane, creating a controlled communication space. The retrograde Gaia 3rd wire entered this space and subsequently the antegrade true lumen, enabling RG3 externalization. Predilation was performed, and IVUS confirmed wire continuity from proximal true lumen to subintimal stented segment and distal true lumen. Three overlapping drug eluting stents (2.75 × 28 mm, 3.0 × 38 mm, 3.5 × 38 mm) were deployed from mid LAD to ostial left main ending with a POT using NC Balloon 5.0 x 8mm.
14.mp4
15.mp4
26.mp4
Case Summary
In this case, inadvertent subintimal stenting rendered further antegrade strategies both ineffective and unsafe. Antegrade wire escalation and parallel wiring were limited by fixed wire bias within the stented false lumen, preventing true lumen re-entry. Antegrade fenestration and re-entry were likewise futile, as the stent immobilized the dissection flap, eliminating the tissue mobility required for fenestration. In the absence of a Stingray balloon, Reverse CART proved effective by creating a controlled communication space between the subintimal stented segment and the distal true lumen, allowing the retrograde wire to safely re-enter and achieve successful revascularization.