Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_002
Reversing the Rules: Reverse Rotablation With RG3 Wire in Complex PCI
By David Te-Wei Kuan, Shih-Chi Liu
Presenter
David Te-Wei Kuan
Authors
David Te-Wei Kuan1, Shih-Chi Liu1
Affiliation
Fu Jen Catholic University Hospital, Taiwan1
View Study Report
CASE20251106_002
Coronary - Complex PCI - CTO
Reversing the Rules: Reverse Rotablation With RG3 Wire in Complex PCI
David Te-Wei Kuan1, Shih-Chi Liu1
Fu Jen Catholic University Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
A 51-year-old woman with a history of end-stage renal disease and coronary artery disease, for which she had previously undergone DES implantation in the LAD artery, presented to the emergency department with chest pain and was diagnosed with NSTEMI. She was a non-smoker with no history of diabetes mellitus or hypertension. Her regular medications included aspirin, bisoprolol, valsartan, and atorvastatin.
Relevant Test Results Prior to Catheterization
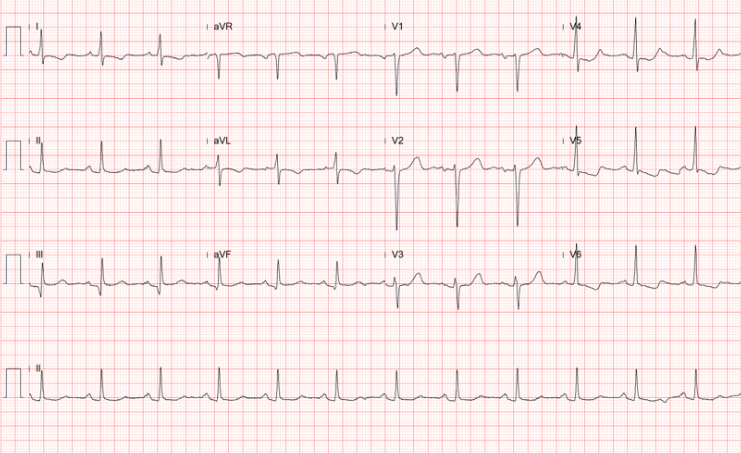
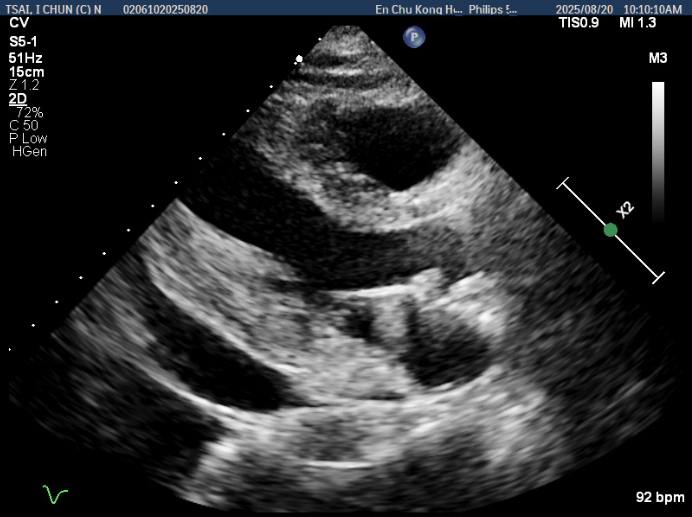
CAG identified ISR of the LAD as the culprit lesion, which was treated with a DCB. A CTO of the RCA was also noticed. A complete revascularisation strategy was planned, and she subsequently underwent a staged PCI three months after the index procedure. ECG showed sinus rhythm with chronic ST depression in the lateral leads. Transthoracic echocardiography revealed a LVEF of 65.2% without RWMA or significant valvular disease. A moderate amount of pericardial effusion was also noted.
Relevant Catheterization Findings
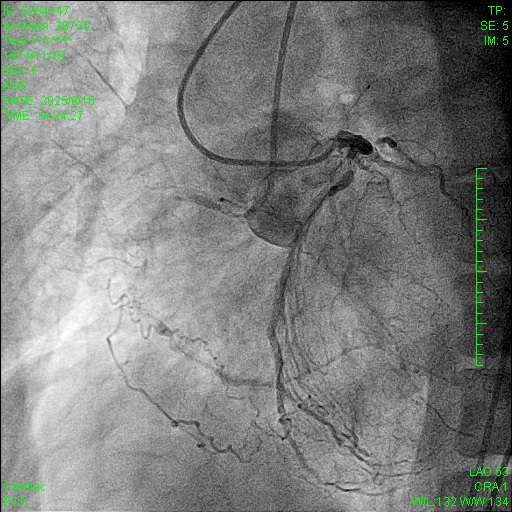
Current angiography showed ISR of the proximal LAD. Regarding the RCA CTO, the J-CTO score was 3 based on lesion calcification, long lesion length, and bending. Collateral circulation was observed through septal collaterals from the LAD and epicardial collaterals from the left circumflex artery, classified as Werner CC2 and J-channel score 0.
Interventional Management
Procedural Step
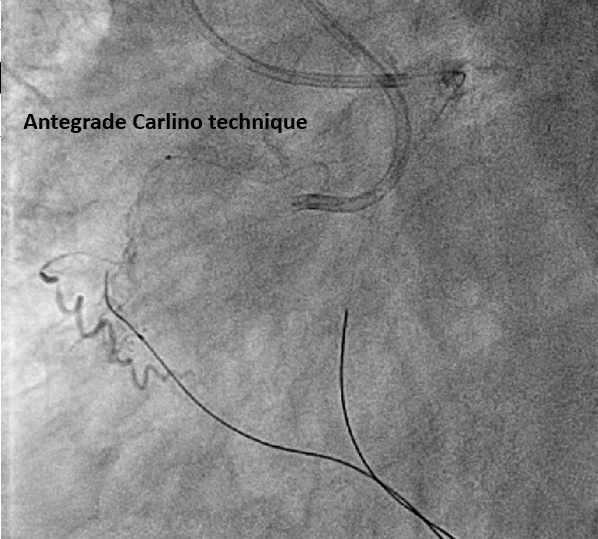
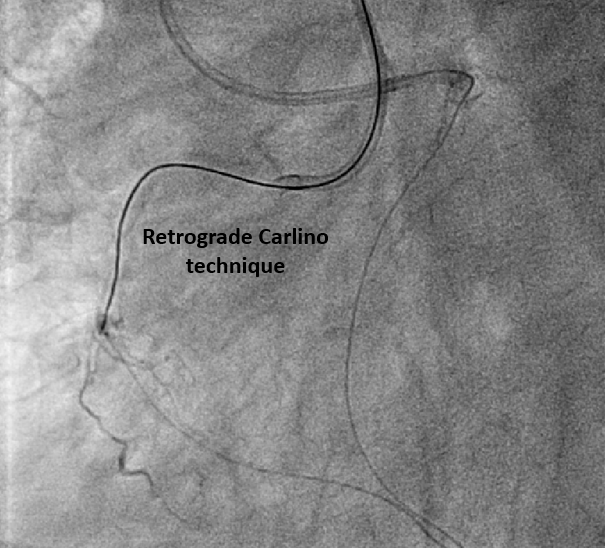
The pLAD ISR was treated first with balloon dilatation followed by DES implantation. An antegrade wire escalation strategy up to Conquest Pro 8-20 for RCA CTO was attempted without success. The wire was left in the subintimal space while a retrograde Sion wire supported by a Finecross microcatheter was advanced through a septal channel to reach the distal CTO cap. The retrograde wire was then exchanged for Gaia 2 and XTA for distal CTO cap penetration. However, a kissing wire technique could not be achieved within the CTO body. Following multiple unsuccessful attempts, the Carlino technique was performed via both the antegrade and retrograde microcatheter. Although a retrograde Fielder FC wire could cross the lesion to the antegrade guiding catheter, this could not be followed by a microcatheter. The retrograde Fielder FC wire was then advanced into the antegrade Tornus microcatheter which also couldn’t cross the lession. Consequently, the retrograde wire was exchanged to RG3. Successful tip-in and externalization with RG3 was achieved afterwards. An antegrade 1.0mm balloon failed to traverse the heavily calcified CTO segment. Therefore, antegrade rotational atherectomy was performed using a 1.25mm burr over the RG3 wire. Following that, the Tornus microcatheter was able to cross the lesion into the distal RCA. A Sion wire was advanced to the distal RCA and the RG3 wire was retrieved. Subsequent balloon dilatation and implantation of two DES were successfully completed

Case Summary
Bi-directional Carlino technique could facilitate intraplaque wire tracking. Usually, after externalisation by RG3 wire, an antegrade microcatheter is advanced distal to the CTO segment for wire exchange, such as a Rotawire in preparation for rotablation. However, in this case, the severe calcification prevented antegrade microcatheter passage. Although the RG3 wire is known to be compatible with rotational atherectomy due to its smaller diameter, its clinical use in this situation is rare. Our case demonstrates the feasibility of performing rotablation over an RG3 wire when neither antegrade nor retroagrde microcatheter passage across the CTO segment is possible.