Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251105_022
Breaking the Stone Without the Stent: Rotational Atherectomy and Intravascular Lithotripsy for Refractory Calcified LAD and Stent Underexpansion
By PeiJung Chen, Tzu-Chieh Lin, Shihhao Yu, Chun-Yuan Chu
Presenter
PeiJung Chen
Authors
PeiJung Chen1, Tzu-Chieh Lin1, Shihhao Yu1, Chun-Yuan Chu1
Affiliation
Kaohsiung Medical University Chung-Ho Memorial Hospital, Taiwan1
View Study Report
CASE20251105_022
Coronary - Complex PCI - Calcified Lesion
Breaking the Stone Without the Stent: Rotational Atherectomy and Intravascular Lithotripsy for Refractory Calcified LAD and Stent Underexpansion
PeiJung Chen1, Tzu-Chieh Lin1, Shihhao Yu1, Chun-Yuan Chu1
Kaohsiung Medical University Chung-Ho Memorial Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
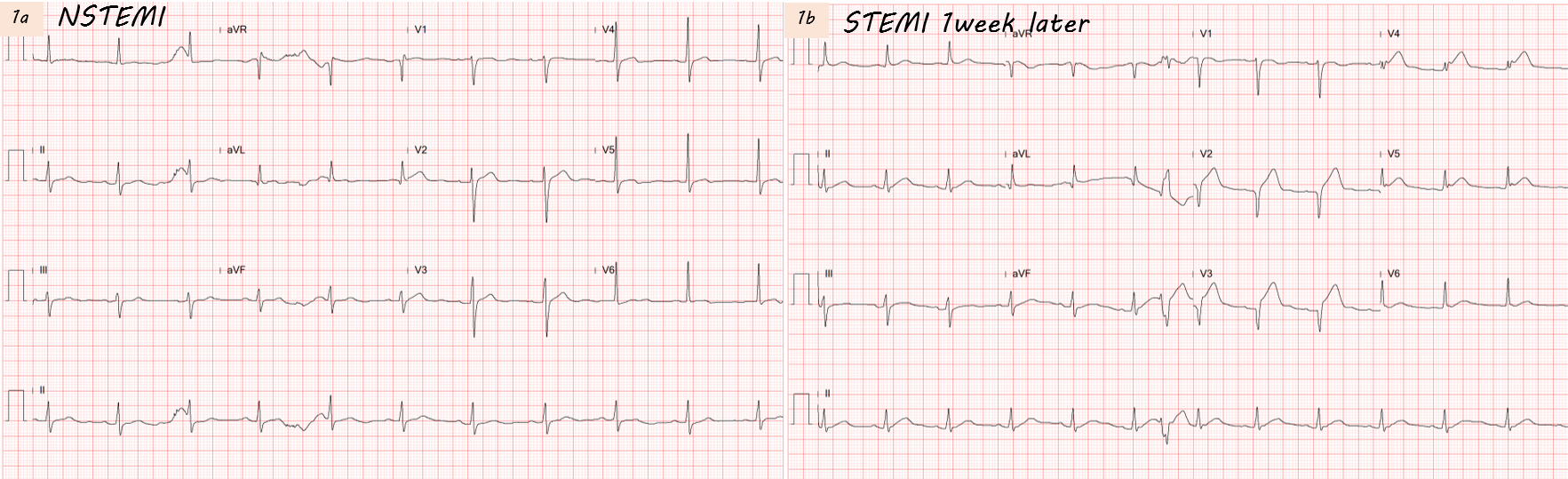
A 79-year-old man with a history of type 2 diabetes mellitus, hypertension, and dyslipidemia was admitted for non–ST-elevation myocardial infarction (NSTEMI) (Fig 1a) presenting with intermittent chest pain. Percutaneous coronary intervention (PCI) was performed during the initial admission; however, intolerable chest pain recurred one week later, and the electrocardiogram (ECG) showed anterior lead ST-segment elevation (Fig 1b).
Relevant Test Results Prior to Catheterization
During the index NSTEMI, cardiac troponin I was only mildly elevated (0.048 → 0.041 → 0.045 → 0.054 ng/mL). The initial ECG showed sinus rhythm with flat T waves (Fig. 1a). One week later, the ECG demonstrated deep Q waves in V2–V3 with persistent ST elevation in V2–V4.
Relevant Catheterization Findings
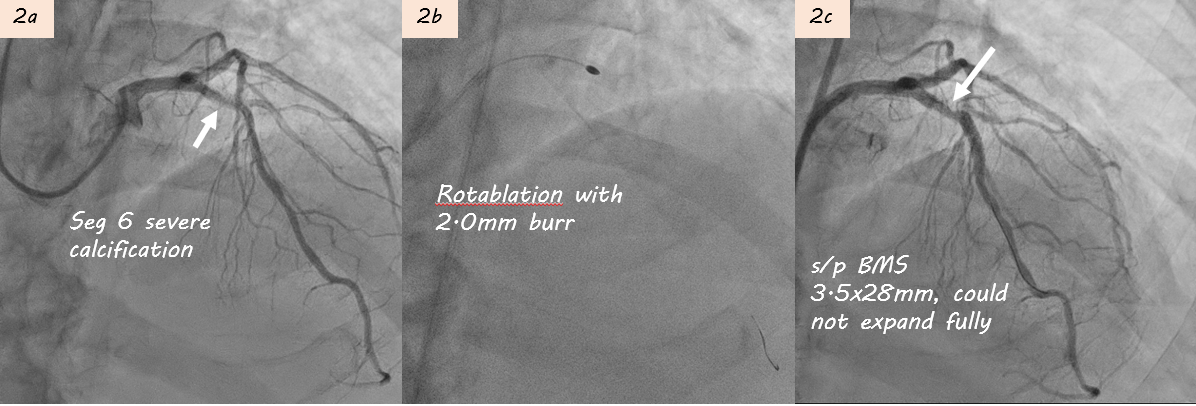
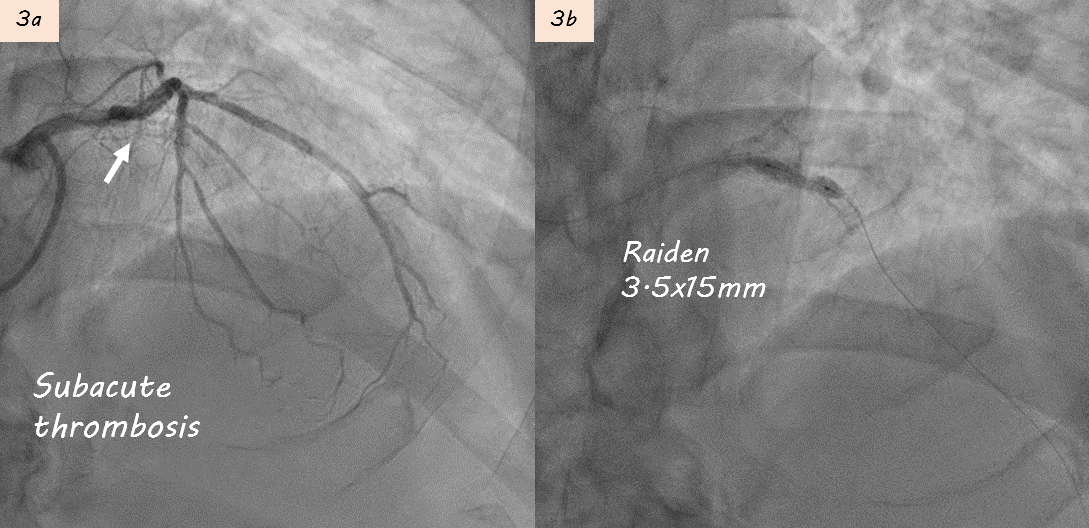
The first angiography revealed 2-vessel disease with 60% stenosis in RCA seg2 and 90% stenosis in LAD seg6. A 3.0×20 mm Euphora balloon could not fully expand, and intravascular ultrasound (IVUS) confirmed heavy calcification. Rotational atherectomy using a 2.0 mm burr was performed, followed by implantation of a 3.5×28 mm bare-metal stent (BMS) (Fig 2a-c). However, one week later, the patient developed STEMI, and repeat angiography showed subacute thrombosis within the LAD stent (Fig3).
Interventional Management
Procedural Step
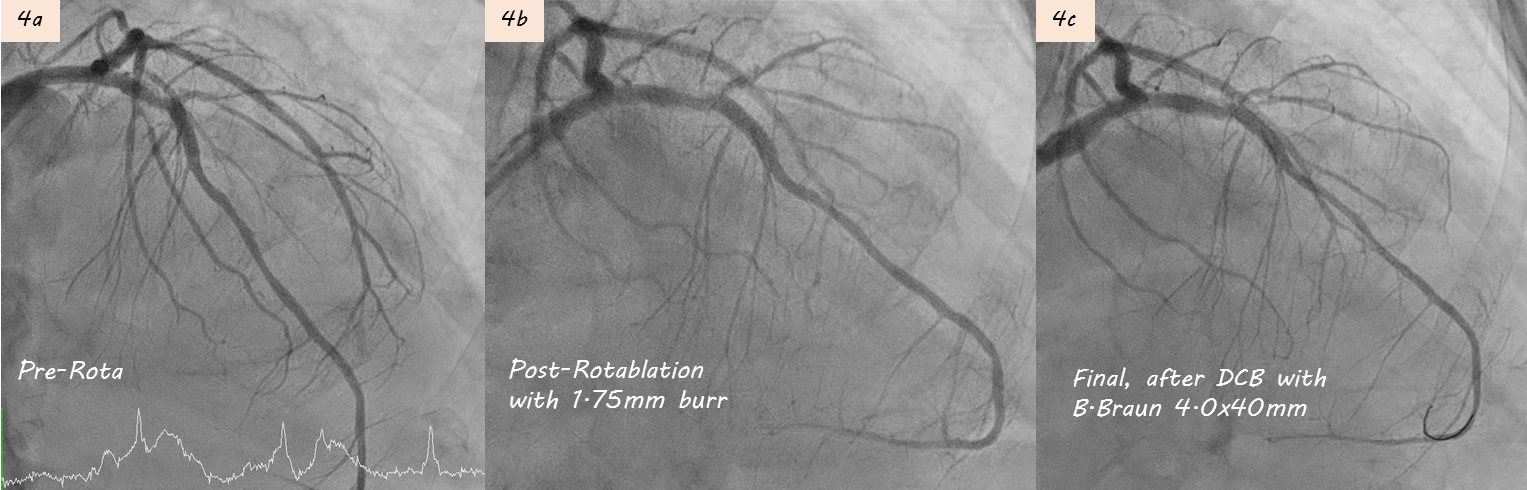
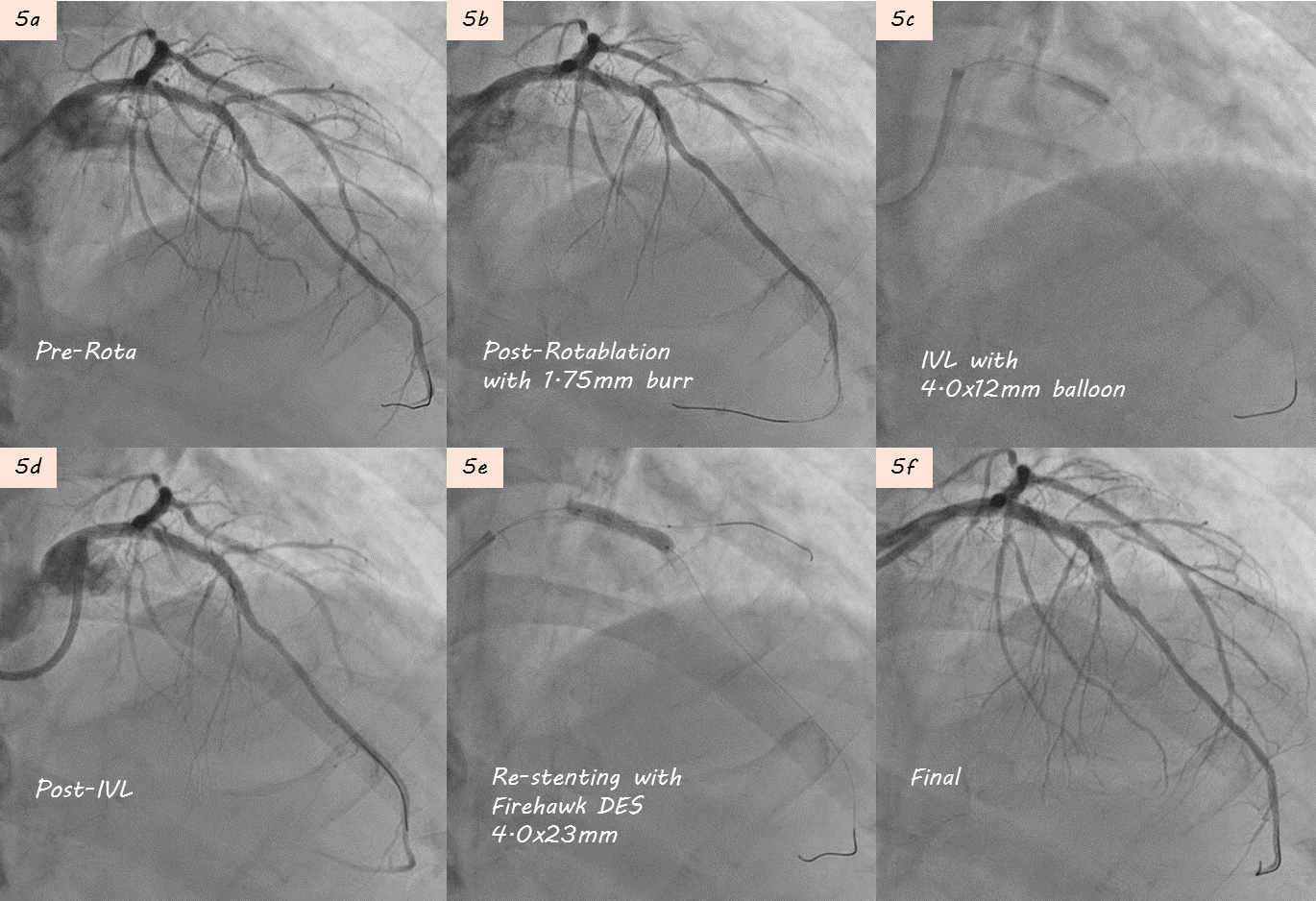
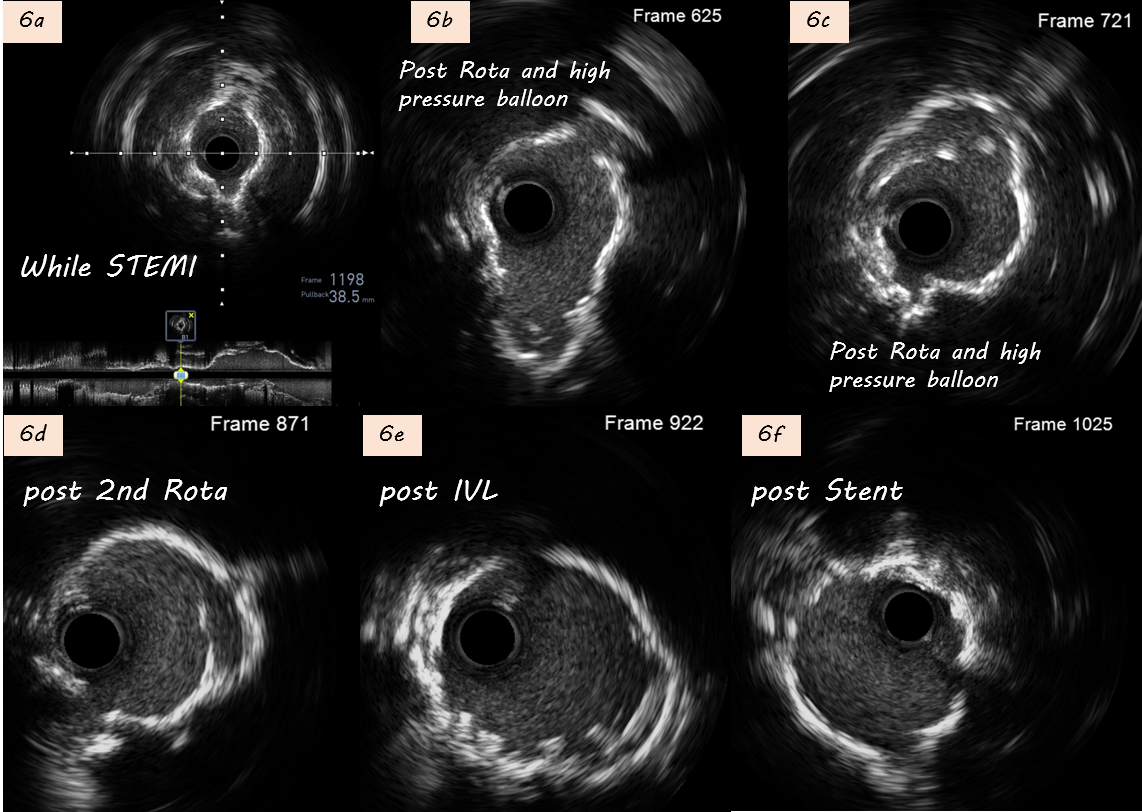
During 1st PCI, IVUS showed severe calcification in LAD seg6 (Fig. 2a). Rotablation with a 2.0 mm burr was performed (Fig. 2b), and a 3.5×28mm Multi-Link BMS was implanted but remained underexpanded (Fig. 2c).STEMI developed one week later prompted repeat CAG showing subacute thrombosis within LAD stent (Fig. 3a). Thrombus aspiration was performed. POBA with a 3.5×15mm Raiden balloon (up to 24 atm) failed to fully expand the stent (Fig 3b). Subsequently, a 3.5×30mm MagicTouch DCB was used.During 3rd PCI,rotational atherectomy was performed with 1.75mm and then 2.0mm burrs; however, 2.0 mm burr entrapment occurred during lesion crossing, and angiography showed limited debulking effect (Fig 4a-b). High-pressure balloon with APT NC 3.5x12mm were attempted but rupture(30 atm). We then POBA with Raiden 3.5×15mm (30 atm), Raiden 4.0×15 mm (32 atm), and NC Euphora 4.5×15mm (20 atm). Finally, 4.0x40mm B. Braun DCB angioplasty was performed (Fig 4c).4th PCI was performed 1 month later for intravascular lithotripsy (IVL) and new stent implantation. Second time rotablation with a 1.75 mm burr was performed (Fig. 5a-b). IVL with a 4.0×12mm balloon (100 pulses) achieved adequate expansion (Fig. 5c–d). Adequate POBA were followed by final stenting using a 4.0×23mm Firehawk DES (Fig. 5e). Proximal optimization technique and kissing balloon technique were performed (Fig. 5f). Serial IVUS showed better debulking after 2nd Rotablation and IVL, and adequate new stent expansion (Fig 6a-6f).
Case Summary
This case highlights stent underexpansion as a critical risk factor for subacute thrombosis, particularly in severely calcified LAD lesions. Despite multiple reinterventions with high-pressure balloons and rotational atherectomy, optimal luminal gain was only achieved after intravascular lithotripsy (IVL) and new DES implantation.For patients with high IVUS calcium scores, meticulous lesion preparation—including adequate balloon expansion before stenting—is essential to prevent stent underexpansion and subsequent restenosis.