Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251105_021
A STAR Is Reborn: Revalidating a Forgotten Technique in a Patient With Anterior STEMI
By Alimi Ahmad Hatib, Randal Low
Presenter
Alimi Ahmad Hatib
Authors
Alimi Ahmad Hatib1, Randal Low 1
Affiliation
Woodlands Health, Singapore1
View Study Report
CASE20251105_021
Coronary - ACS/AMI
A STAR Is Reborn: Revalidating a Forgotten Technique in a Patient With Anterior STEMI
Alimi Ahmad Hatib1, Randal Low 1
Woodlands Health, Singapore1
Clinical Information
Relevant Clinical History and Physical Exam
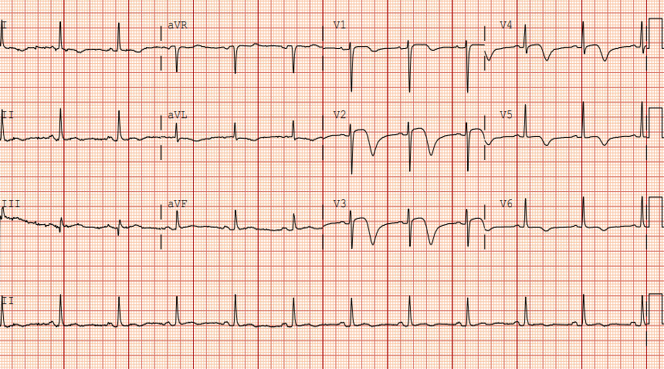
An 80 year old lady with diabetes mellitus, hypertension and dyslipidemia presented to the emergency department for 3 days of worsening chest discomfort radiating to the jaw. She was hemodynamically stable on arrival and the initial physical examination was unremarkable. Her pain was unremitting despite analgesia. An electrocardiogram revealed anterolateral ST elevations with deep T-wave inversions consistent with an anterior ST-elevation myocardial infarction.
Relevant Test Results Prior to Catheterization
The initial laboratory results indicated an elevated Troponin I level of 5890 ng/L (reference range 0-14). She otherwise had a normal hemoglobin level of 13 g/dL and a normal creatinine of 65 mmol/L (reference range 44-97 mmol/L). She was taken to the invasive cardiac lab for emergent percutaneous coronary intervention (PCI) in view of ongoing symptoms despite the delay in presentation.
Relevant Catheterization Findings
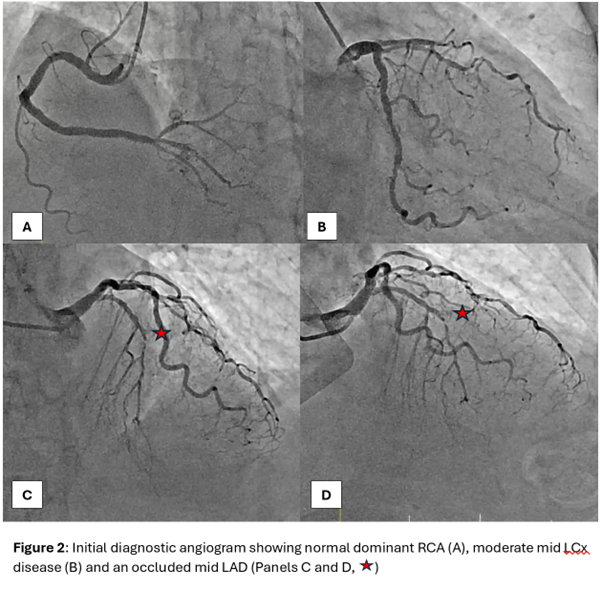
The diagnostic angiogram showed a right dominant circulation with a completely occluded mid left anterior descending (LAD) artery and mild to moderate disease elsewhere. Of note, there were no significant collaterals to the distal LAD from the left circumflex (LCx) and right coronary arteries (RCA).
 STAR diagnostic angiogram.mp4
STAR diagnostic angiogram.mp4
Interventional Management
Procedural Step
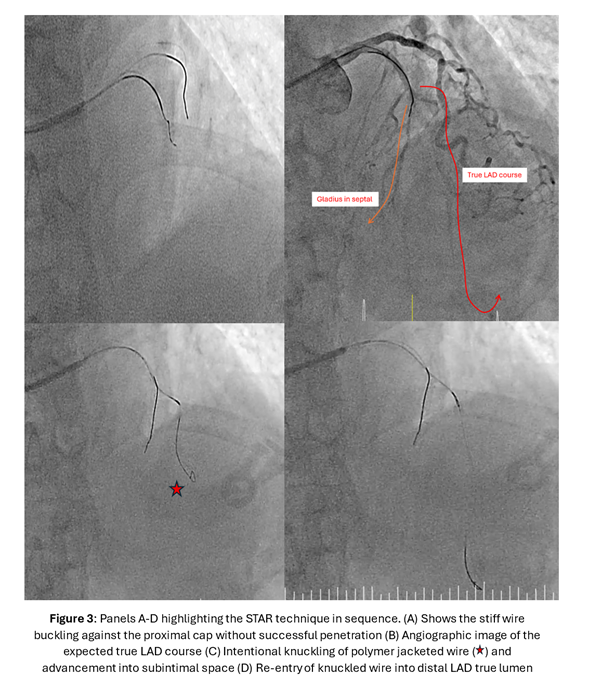
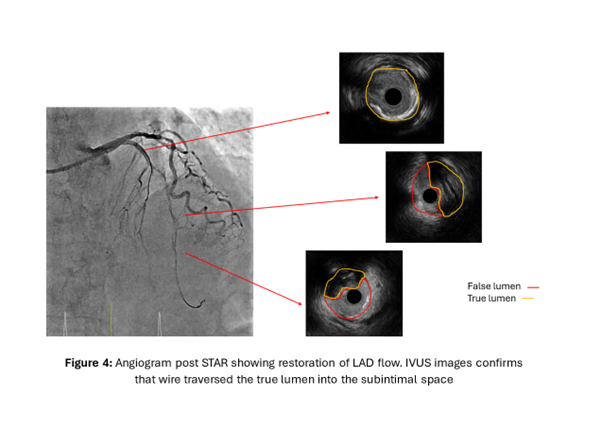
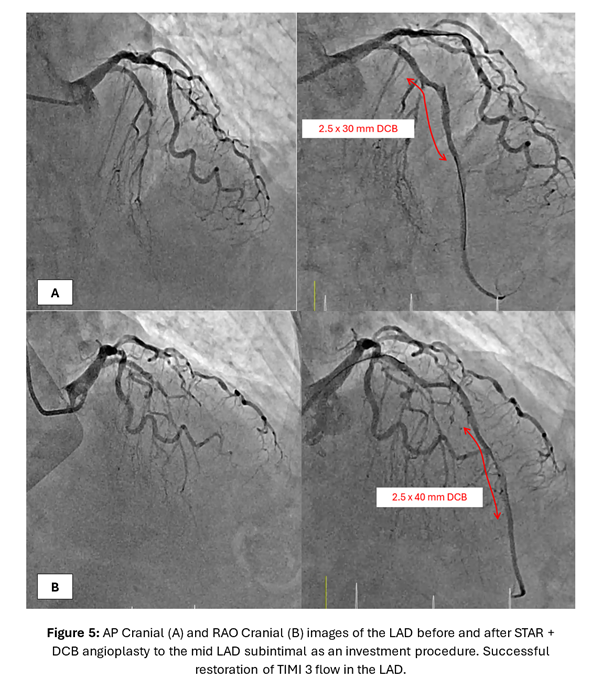
A torqueable microcatheter was used pre-emptively in view of expected difficulties wiring. The LAD occlusion was unsuccessfully crossed despite wire escalation from workhorse wires to polymer-jacketed and finally stiff wires with high tip loads. The wires either deflected into the septal branches or entered the subintimal space. Faced with the difficult situation of a patient with anterior STEMI with ongoing symptoms compounded by an acute-on-chronic mid LAD occlusion with no distal vessel visualization from collaterals to guide wiring, a decision was made to perform the Subintimal Tracking and Re-entry (STAR) technique. As a subintimal space had already been created from previous wiring attempts, a polymer jacketed wire with a pre-formed U-bend was advanced into the space forming a loop. Thereafter, the knuckled wire was pushed forward with the intention of bluntly dissecting the subintimal space and re-entering the distal true lumen. This successfully restored flow in the LAD and intravascular ultrasound images confirmed the wire to be in the mid LAD subintimal space. As the primary objective was to re-establish LAD flow and patient's symptoms improved, drug-coated balloon angioplasty of the subintimal space as an "investment" for subsequent definitive PCI was performed. A relook angiogram 3 months later showed patent mid LAD subintimal DCB segments with TIMI 3 flow. 2 drug eluting stents were placed in the left main to mid LAD for definitive PCI.
STAR technique.mp4
STAR and DCB investment.mp4
STAR Relook and final DES.mp4
Case Summary
The STAR technique is typically utilized in PCI for chronic total occlusions as a bailout or investment strategy. This unique case highlights the challenge of a wire uncrossable LAD occlusion with no distal visualization in a patient with STEMI and ongoing ischemia. Nevertheless, flow was re-established with resolution of symptoms after STAR and subsequent DCB. The 3-month relook angiography showing TIMI 3 flow through the newly created subintimal tract into the apical LAD is a testament to the effectiveness and safety of the STAR even in the setting of non-CTO and acute PCIs. This re-validates the forgotten STAR technique as a viable option for acute wire uncrossable lesions.