Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251105_020
Ureteric Stent Migration Into the Right Atrium: Retrieve Through Endovascular Approach
By Kirankumar Dyawarkonda
Presenter
Kirankumar Dyawarkonda
Authors
Kirankumar Dyawarkonda1
Affiliation
CDSIMER, India1
View Study Report
CASE20251105_020
Endovascular - Other Endovascular Interventions
Ureteric Stent Migration Into the Right Atrium: Retrieve Through Endovascular Approach
Kirankumar Dyawarkonda1
CDSIMER, India1
Clinical Information
Relevant Clinical History and Physical Exam
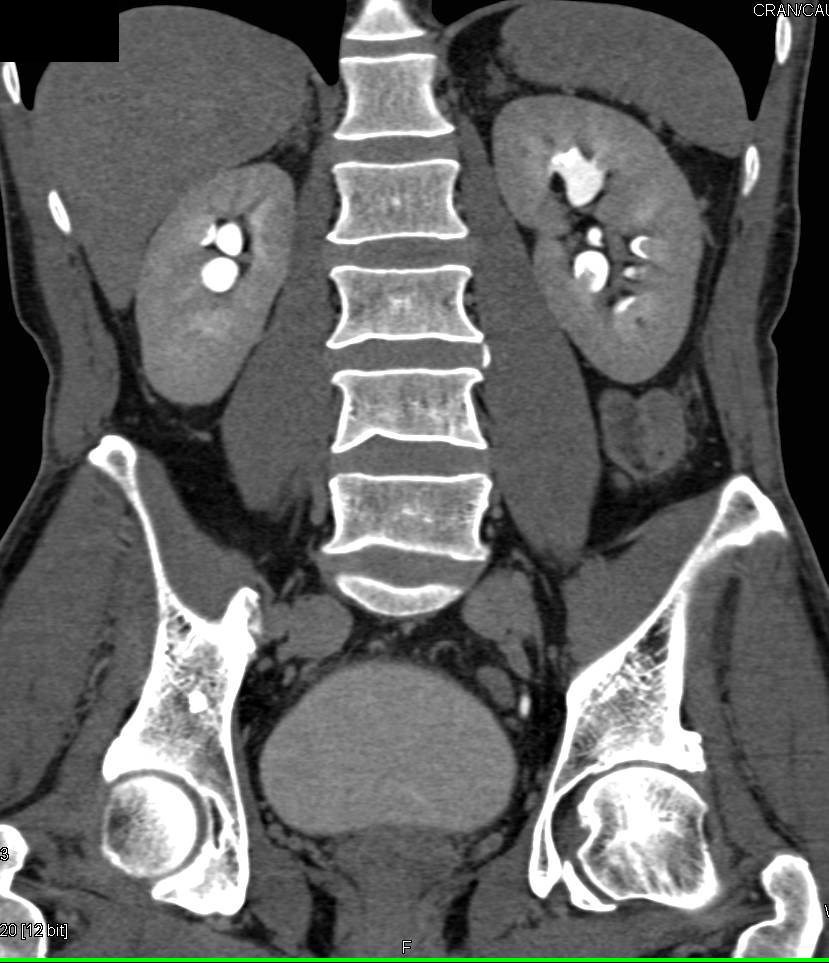
A middle-aged female patient presented with acute onset, severe, colicky left flank pain radiating to the groin for four days. There was no associated history of fever, gross hematuria.Pre-operative CT Kidney Ureter Bladder with contrast revealed right ureteric and left renal calculi.On admission, vital signs were stable: Physical examination was unremarkable, with a soft, non-tender abdomen and normal bowel sounds. The patient remained hemodynamically stable throughout the initial evaluation.
Relevant Test Results Prior to Catheterization
Initial laboratory work-up showed normal renal function (details of specific values withheld for privacy/length). Imaging confirmed the diagnosis of right ureteric calculus and left renal calculus, which was the target of the initial intervention. The left kidney appeared hydronephrotic due to the obstruction.
Relevant Catheterization Findings
Initial attempts at retrograde left ureteric stenting were hampered by a completely adherent stone, preventing the passage of a standard guide wire. A subsequent thinner, hydrophilic Terumo guide wire was easily negotiated past the obstruction. A diagnostic anomaly was noted when the passage showed an unusual rightward curvature upon successful navigation, leading to suspicion of misplacement.
Interventional Management
Procedural Step
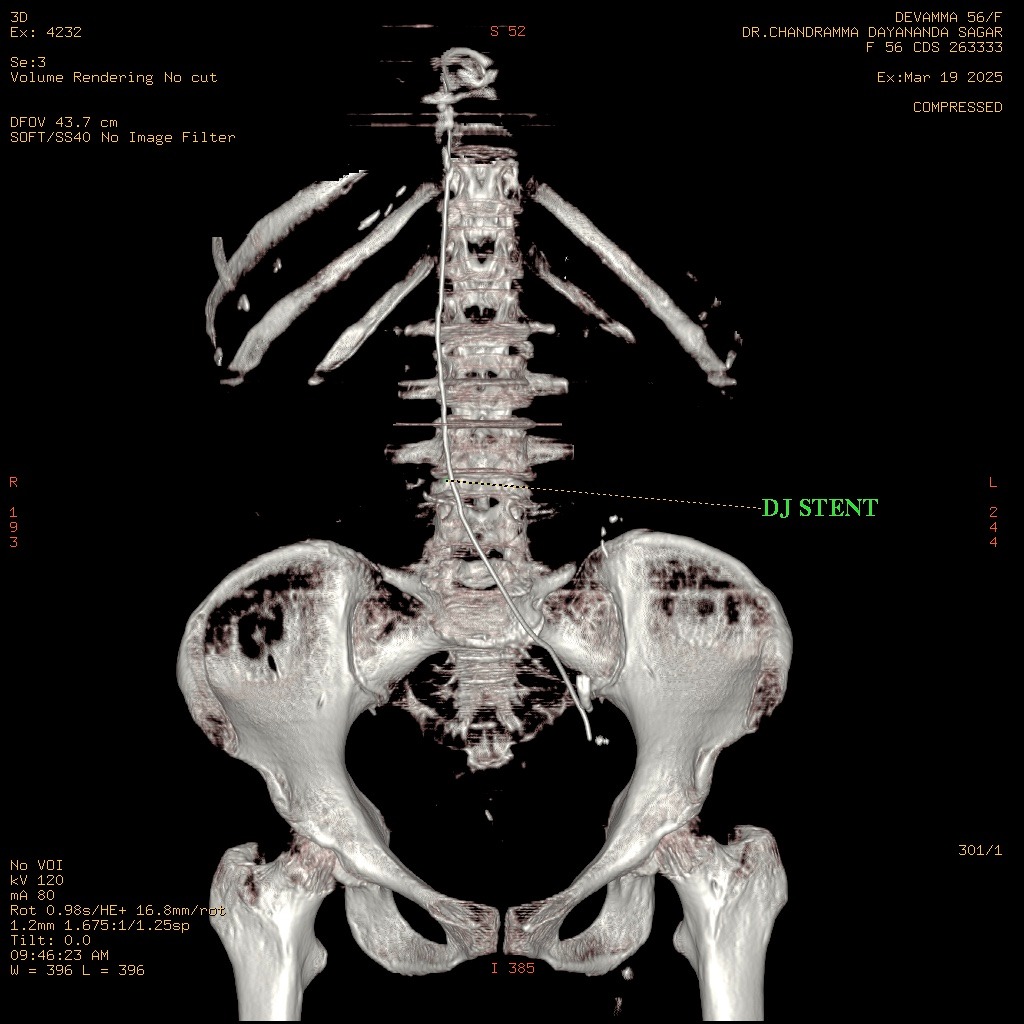
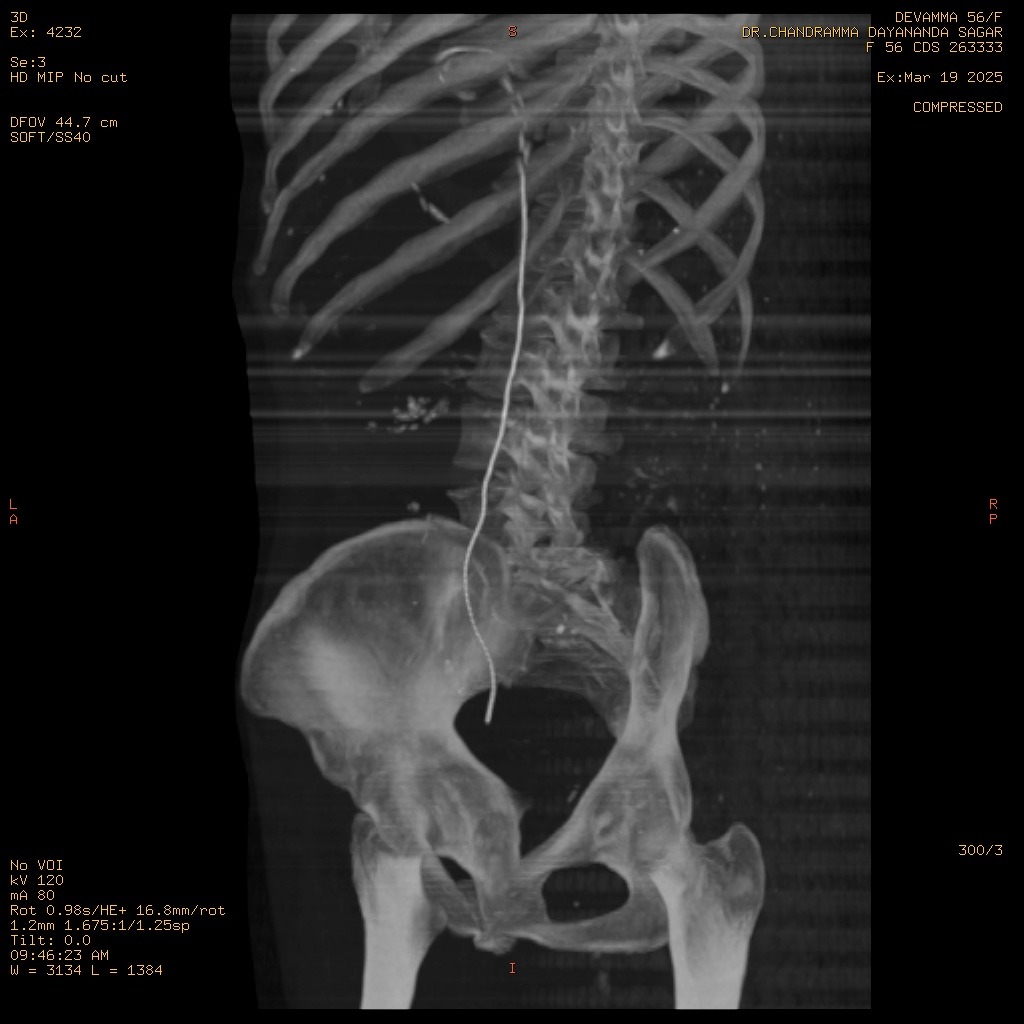
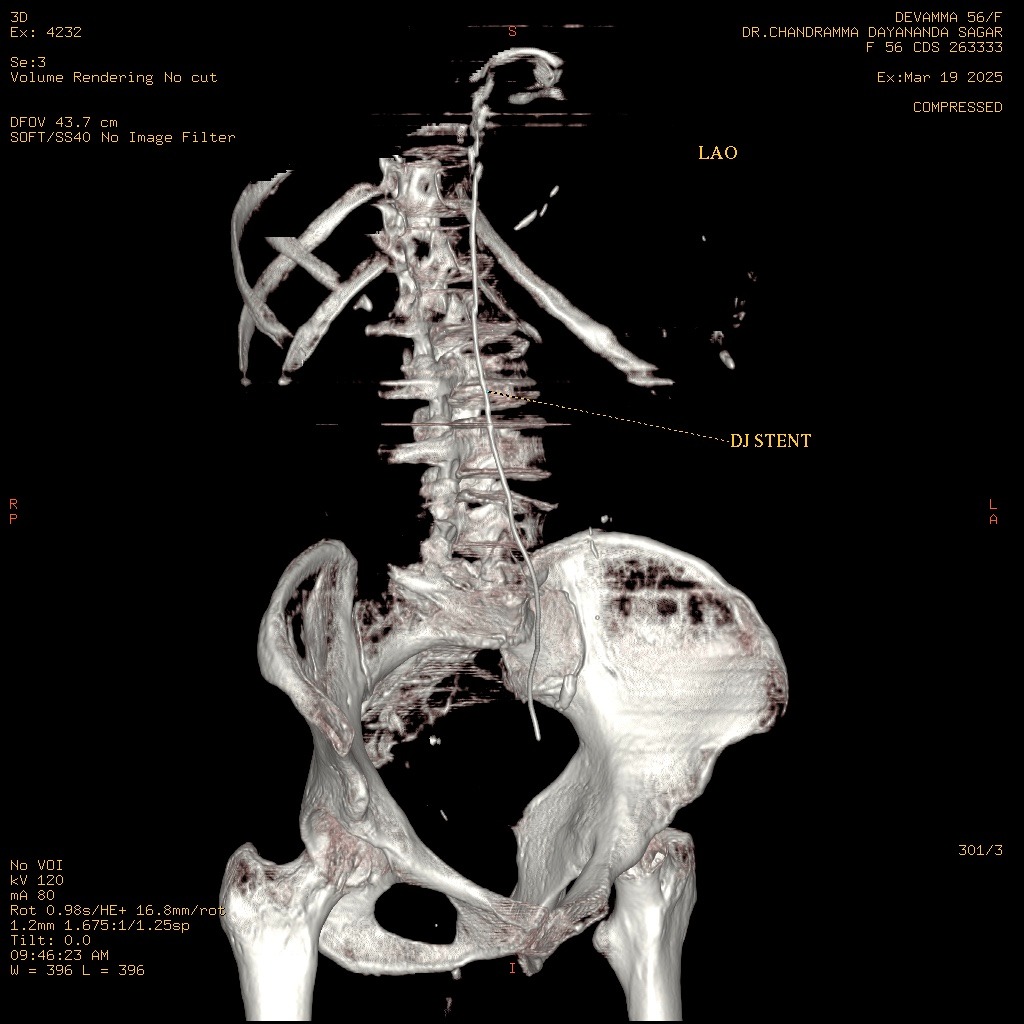
Following the easy passage of the hydrophilic wire, a 3Fr ureteric stent was passed over it. The stent advanced without resistance, but the proximal pigtail did not coil in the renal pelvis, heightening the suspicion of misplacement. An immediate post-procedure CT scan confirmed the stent's location: the distal end was correctly within the bladder, but the main body and proximal end were located outside the ureter, passing into the Inferior Vena Cava. However, further investigation with MRI of Abdomen revealed that the stent had migrated from the bladder to the left internal iliac vein and reached in the Right Atrium. The patient remained hemodynamically stable. A team meeting was sought, including the opinions of the Cardiologist, Cardiothoracic surgeon, and Urologist, and came to a conclusion that a attempt via endovascular retrieval of the stent. Initial attempts by interventional cardiology via the femoral vein to the Right Atrium failed. Successful retrieval was achieved by an alternative access via the right internal jugular vein, direct entry into the left internal iliac vein. A snare catheter was skillfully deployed to secure the distal end of the DJ stent. The stent was removed successfully without any immediate vascular complication. The patient was monitored in the MICU post-procedure. On the second day post procedure, patient developed mild hematuria and was treated conservatively, and repeat CT KUB with contrast was done, which did not show any remnant fistula.
 Img1 - Copy.mp4
Img1 - Copy.mp4
Img6.mp4
Img8.mp4
Case Summary
DJ Stent migration into the cardiac chambers represents a catastrophe, with published literature frequently describing the need for emergency cardiothoracic surgery (e.g., sternotomy or thoracotomy) to prevent life-threatening sequelae such as arrhythmias, tricuspid valve damage, or myocardial perforation. Ureteral stent migration, particularly rare vascular displacement to the heart requires immediate diagnosis and retrieval. Our case demonstrates that a rapid, endovascular approach provides the safest template for management, setting a new standard for emergent care. Careful placement and sizing remain vital to prevent migration