Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251105_016
A Complex Chronic Total Occlusion Percutaneous Coronary Intervention Case: A Retrograde Approach via Ipsilateral Collateral Circulation to Revascularize a Left Circumflex Artery Chronic Total Occlusion, Facilitated by the Ping-Pong Guiding Catheter Technique and Stent-Based Reverse Controlled Antegrade and Retrograde Tracking
By Shun Hei Wong
Presenter
Shun Hei Wong
Authors
Shun Hei Wong1
Affiliation
Tseung Kwan O Hospital, Hong Kong, China1
View Study Report
CASE20251105_016
Coronary - Complex PCI - CTO
A Complex Chronic Total Occlusion Percutaneous Coronary Intervention Case: A Retrograde Approach via Ipsilateral Collateral Circulation to Revascularize a Left Circumflex Artery Chronic Total Occlusion, Facilitated by the Ping-Pong Guiding Catheter Technique and Stent-Based Reverse Controlled Antegrade and Retrograde Tracking
Shun Hei Wong1
Tseung Kwan O Hospital, Hong Kong, China1
Clinical Information
Relevant Clinical History and Physical Exam
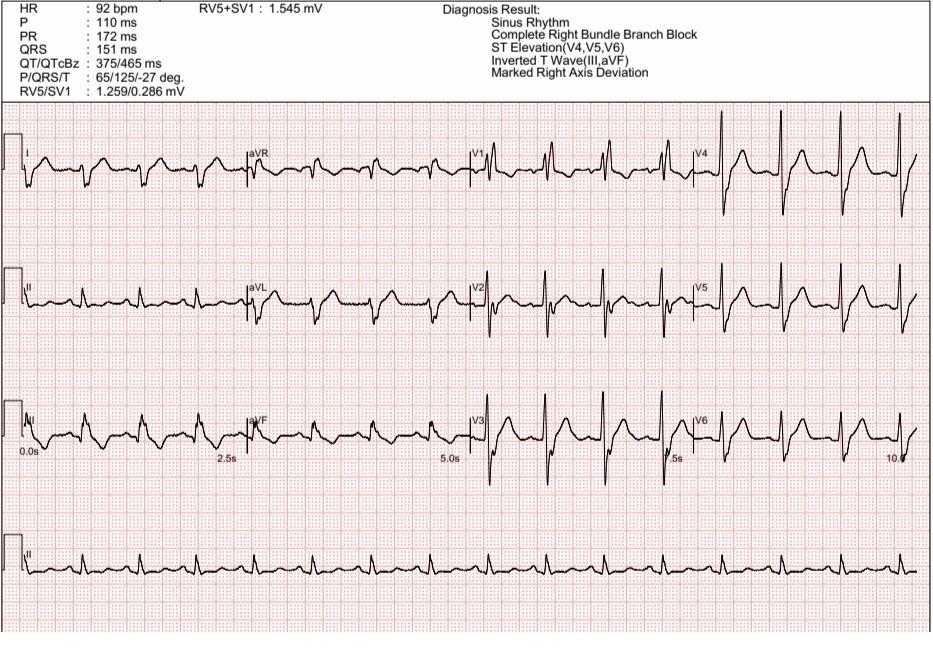
A 55-year-old male ex-smoker with a history of diabetes, hypertension, and hyperlipidaemia presented with progressive stable angina. ECG demonstrated sinus rhythm with RBBB. Initial coronary angiogram done by a private cardiologist showed severe triple vessel disease with severe stenoses in the pLAD, p-mD2, and pRCA, and CTOs in mLCx and mRCA. Following private PCI with DES to the LAD and D2, his persistent angina remained. Consequently, he was referred to our unit for PCI to RCA and LCx CTOs.
Relevant Test Results Prior to Catheterization
The echocardiogram showed satisfactory LV systolic function LVEF 60% without regional wall abnormalities or significant valvular lesions. His renal function was normal, with an eGFR >90 mL/min/1.73 m², which is favorable for planning a complex PCI.
Relevant Catheterization Findings
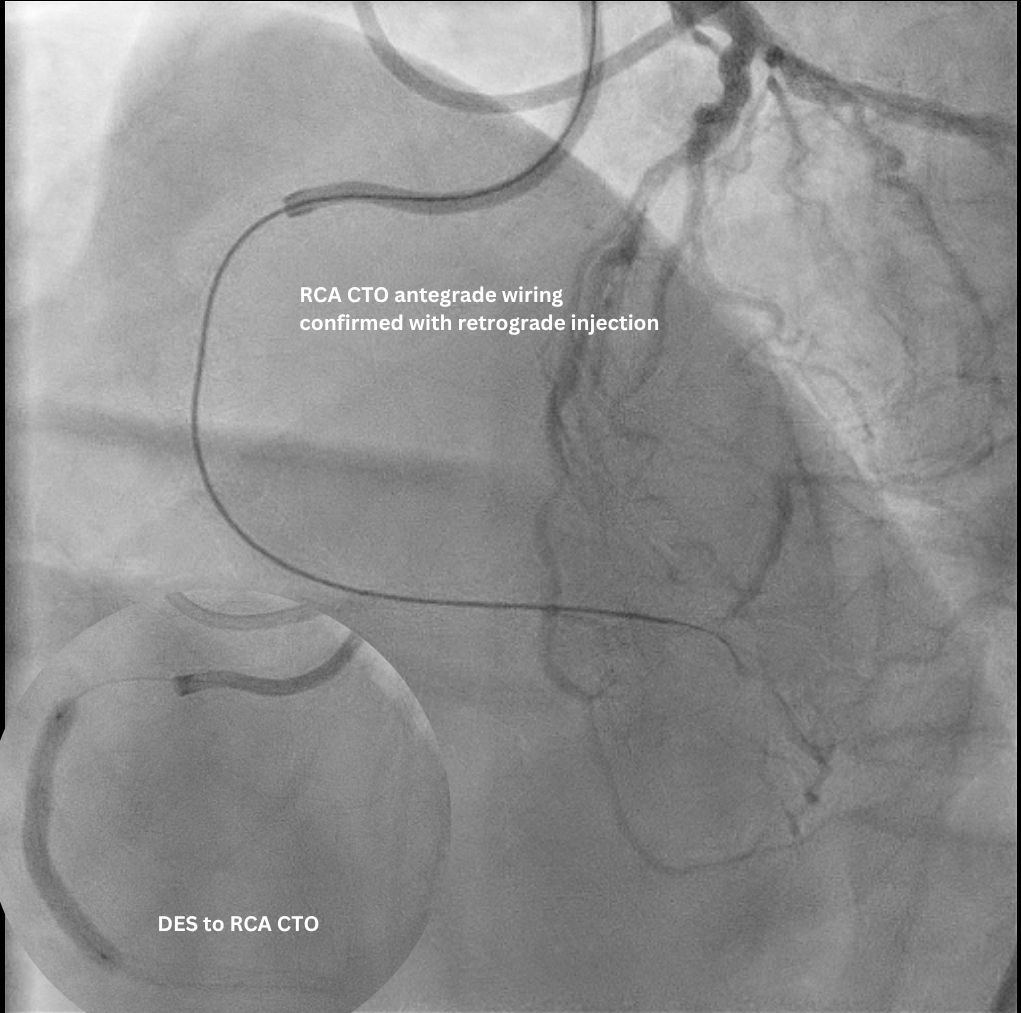
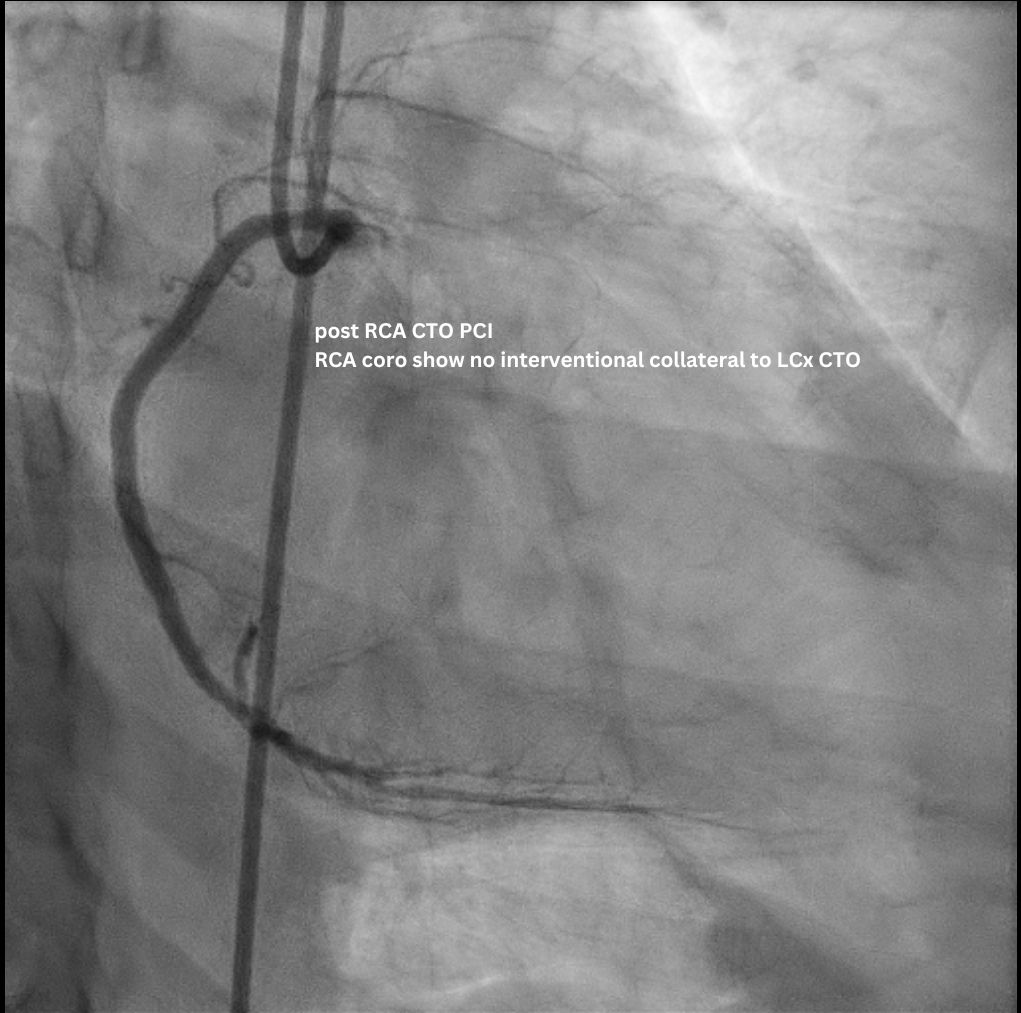
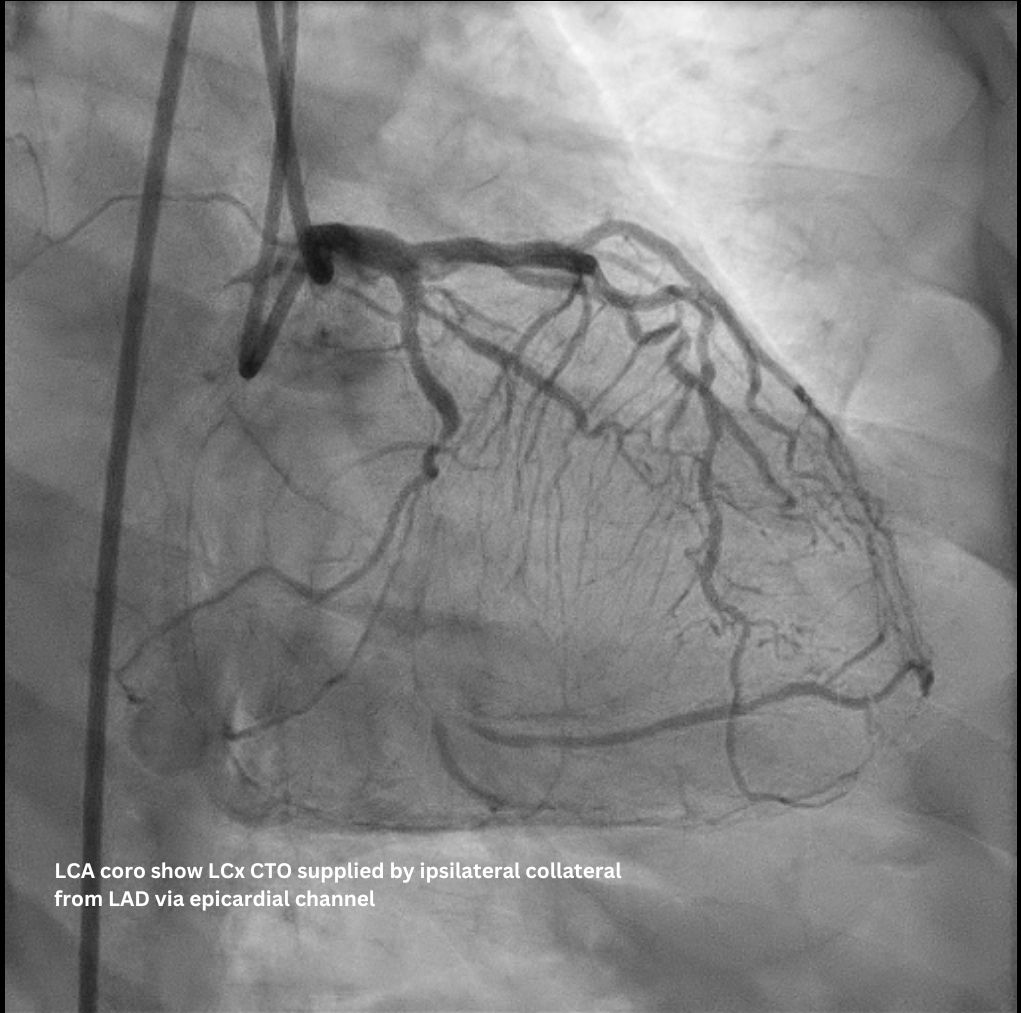
The staged PCI for the RCA CTO was completed uneventfully via an antegrade approach. Subsequent LCA angiogram showed a p-d LCx CTO supplied by an ipsilateral collateral from the D1/ LAD via an epicardial channel. RCA angiography confirmed no interventional contralateral supply. Detailed lesion analysis showed an ambiguous proximal cap (with the atrial branch as a large side branch), ~20 mm CTO length, a bend > 45°, and the distal cap located precisely at the dLCx/OM2 bifurcation.
 2025-9 LCx CTO coro bilateral injection RAO CAU after RCA CTO PCI.mp4
2025-9 LCx CTO coro bilateral injection RAO CAU after RCA CTO PCI.mp4
2025-9 LCx CTO coro RCA injection RAO CAU after RCA CTO PCI.mp4
Interventional Management
Procedural Step
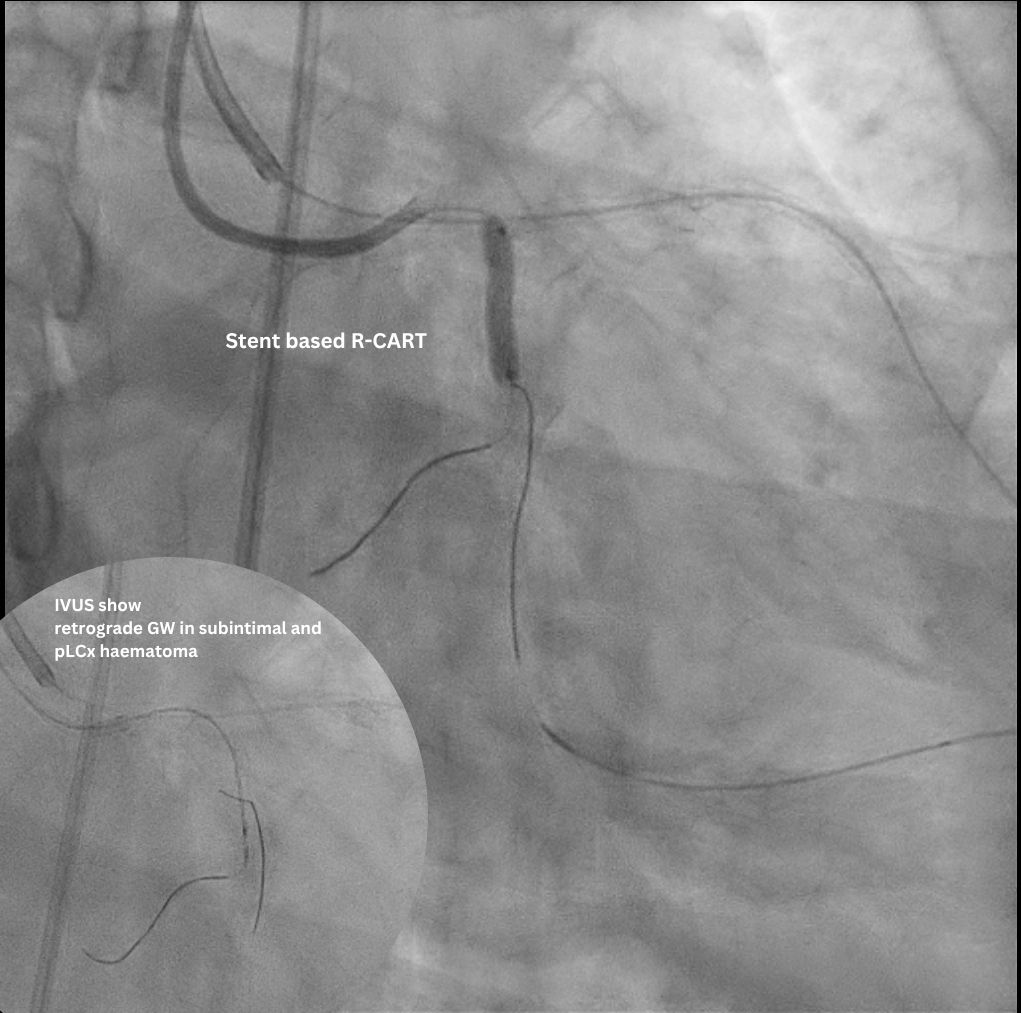
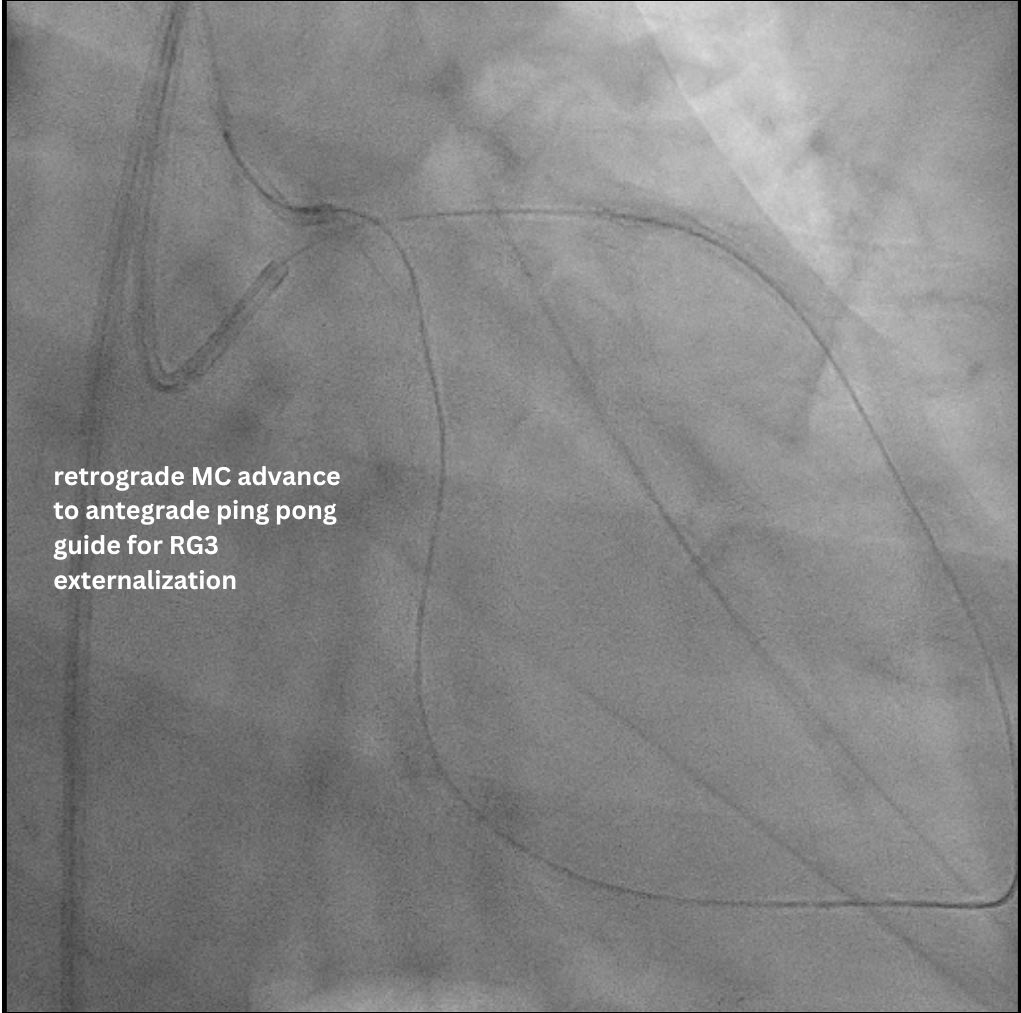
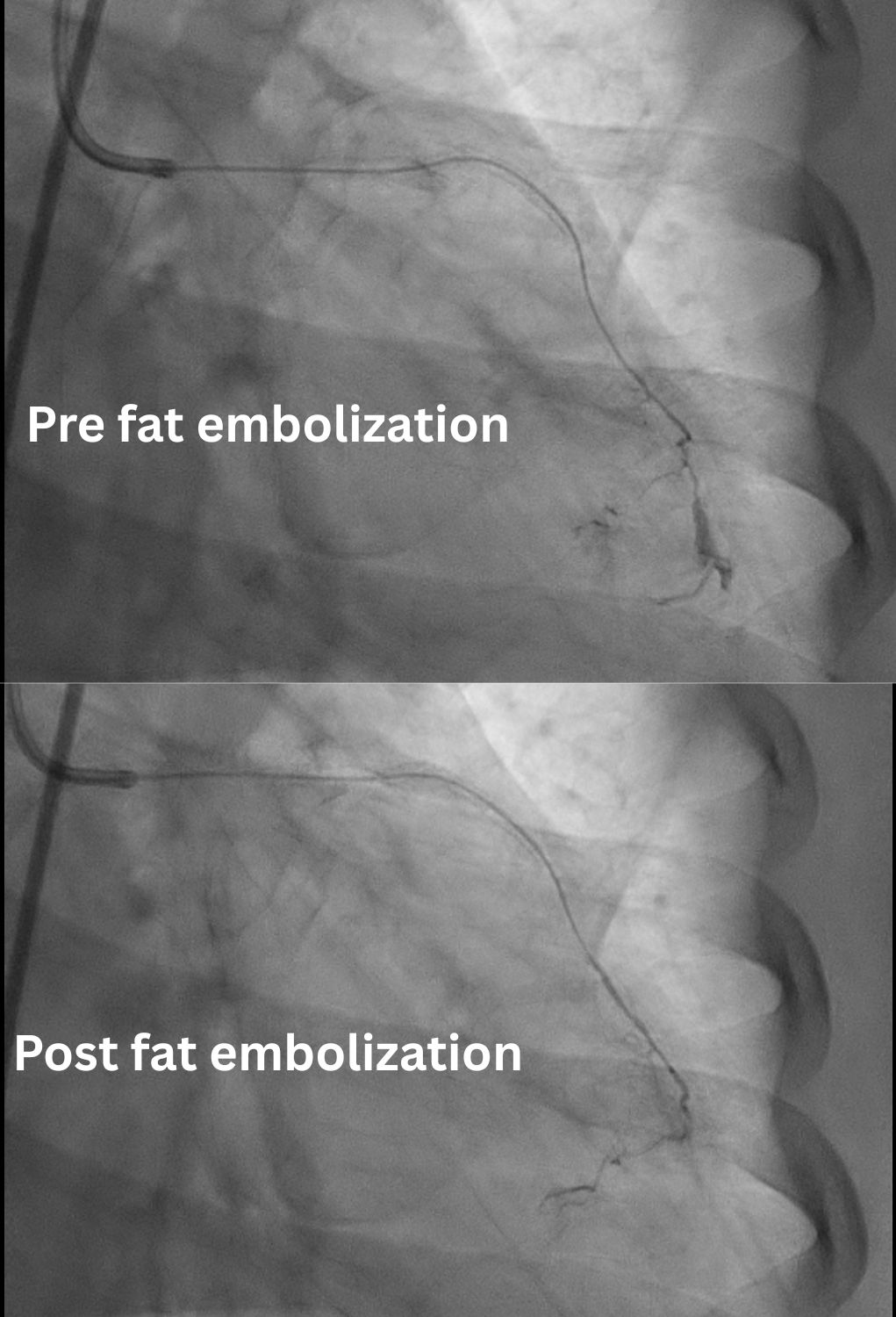
Access was achieved via RRA and US-guided RFA puncture. A 7F SBP 3.5 guide was engaged to LM, and a 6F IL 3.5 guide was in oRCA, confirming no contralateral supply to LCx CTO. After a failed antegrade IVUS guided puncture by GW Gaia Next 2, the strategy shifted retrograde. GW Sion supported by microcatheter Caravel successfully navigated D1 across LAD stent struts, visualizing the ipsilateral epicardial collateral to OM2. The wire was exchanged to SUOH 03 and then advanced to OM2. After initial retrograde wiring failures by a UB3, a Gladius MG successfully crossed the CTO body to pLCx. IVUS to pLCx confirmed retrograde wire in subintimal plane. Multiple attempts R-CART failed in p-mLCx despite wire escalation to GW Gaia Next 3. Repeat IVUS showed enlarging pLCx hematoma, necessitating deployment of a DES (ULTIMASTER NAGOMI 3.0 mm/18 mm) to seal the entry point. Successful stent based R-CART was then achieved with Gaia Next 3, confirmed by IVUS. The IL 3.5 guide was moved to LM as an antegrade Ping-Pong guide for RG3 externalization after successfully advancing retrograde wire and microcatheter to the IL guide. The m-dLCx was prepared by SC balloons and a DES (ULTIMASTER NAGOMI 2.5 mm/50 mm) was deployed to the p-dLCx-OM2, overlapping the proximal DES. A D1 perforation was noted and then successfully treated with fat embolism via the retrograde microcatheter. Final angiogram and IVUS confirmed optimal results.
2025-9 LCx CTO MC tip injection RAO25 CAU25 (for ipsilateral channel).mp4
2025-9 LCx CTO finishing RAO CAU.mp4
2025-9 LCx CTO finishing LAO CRA.mp4
Case Summary
This intervention successfully revascularized a challenging LCx CTO despite antegrade failure and absent contralateral collaterals. Success hinged on strategic retrograde access via an uncommon ipsilateral epicardial collateral from the LAD, and overcoming pLCx hematoma via a specialized, IVUS-guided, stent-based R-CART technique using localized stent deployment. The Ping-Pong guide setup streamlined the complex wire externalization process. This case demonstrates that combining advanced hybrid techniques and modifying the R-CART strategy is essential for optimal outcomes in high-complexity CTO PCI.