Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251105_015
OCT-Guided Diagnosis of Early Stent Thrombosis in a Patient Presenting With OHCA and Inferior Wall STEMI
By Chia-Yi Lin, Yen-Lien Chou
Presenter
Chia-Yi Lin
Authors
Chia-Yi Lin1, Yen-Lien Chou2
Affiliation
Tri-Service General Hospital, National Defense Medical University; Taoyuan Armed Forces General Hosp, Taiwan1, Tri-Service General Hospital, National Defense Medical University, Taiwan2
View Study Report
CASE20251105_015
Coronary - ACS/AMI
OCT-Guided Diagnosis of Early Stent Thrombosis in a Patient Presenting With OHCA and Inferior Wall STEMI
Chia-Yi Lin1, Yen-Lien Chou2
Tri-Service General Hospital, National Defense Medical University; Taoyuan Armed Forces General Hosp, Taiwan1, Tri-Service General Hospital, National Defense Medical University, Taiwan2
Clinical Information
Relevant Clinical History and Physical Exam
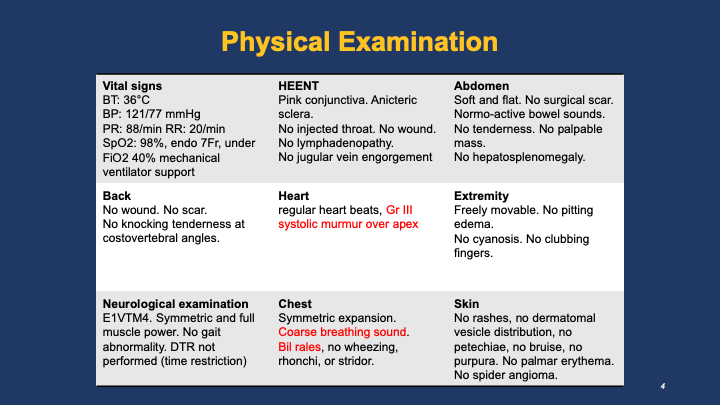
A 91-year-old man with hypertension, diabetes, and advanced dementia, chronically bed-ridden, underwent PCI with two stents one week earlier. He was found pulseless at a nursing home; CPR for 10 min with one AED shock achieved ROSC. On arrival, he was comatose (GCS 5), BP 121/77 mmHg, HR 88 bpm, SpO₂ 98 % on ventilation. Physical exam showed Gr III systolic murmur over apex; the remainder was unremarkable.
Relevant Test Results Prior to Catheterization
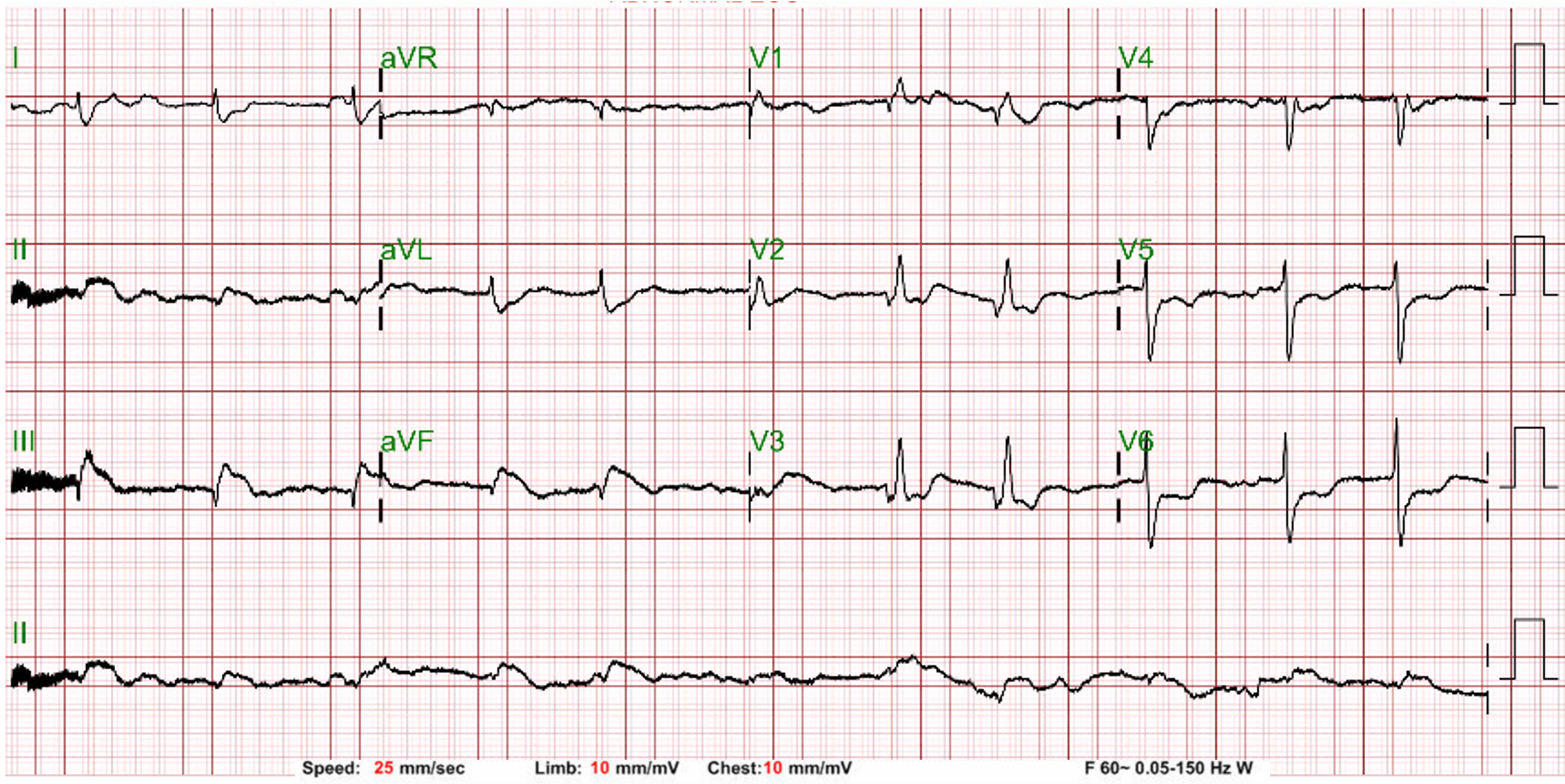
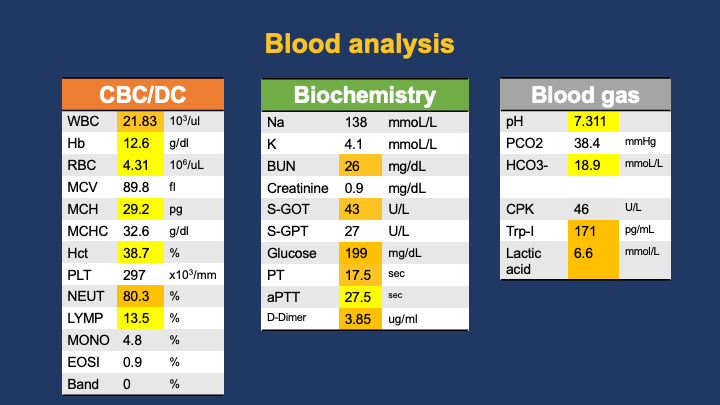
ECG showed sinus rhythm with pathologic Q waves and ST-segment elevation in leads II, III, and aVF with reciprocal changes in precordial leads. Brain and chest CECT revealed no significant abnormalities. Laboratory data revealed mild CPK elevation (46 U/L) and markedly elevated HS-troponin I (171 pg/mL).
Relevant Catheterization Findings
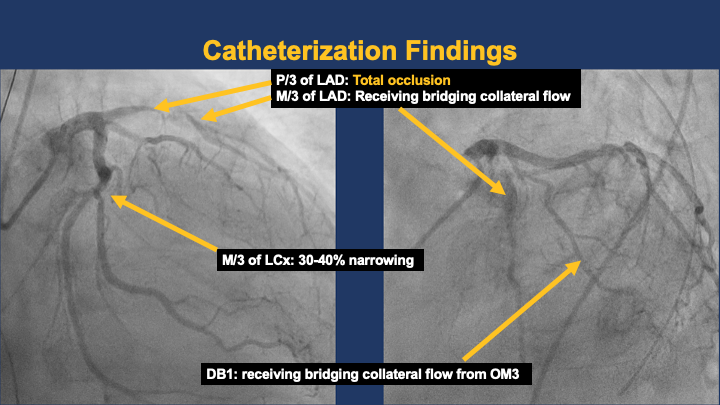
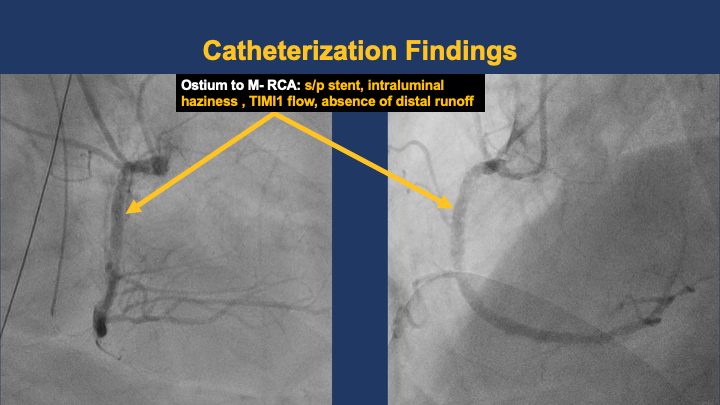
LMCA patent. LAD : proximal CTO ( about 2 cm, blunt end, non-calcified, no bending). DB1 and mid LAD received bridging collaterals. LCX showed luminal irregularity with 30–40 % tubular narrowing at mid segment. RCA proximal stent segment suspicious for acute thrombosis, mid segment possible de-novo lesion or stent fracture, distal stent patent with haziness suggesting thrombus.
 Left RAOCAU.mov
Left RAOCAU.mov
RCA1.mov
OCT 1st.mov
Interventional Management
Procedural Step
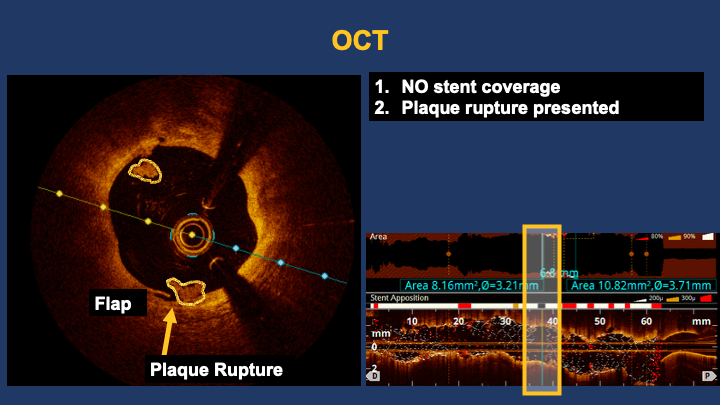
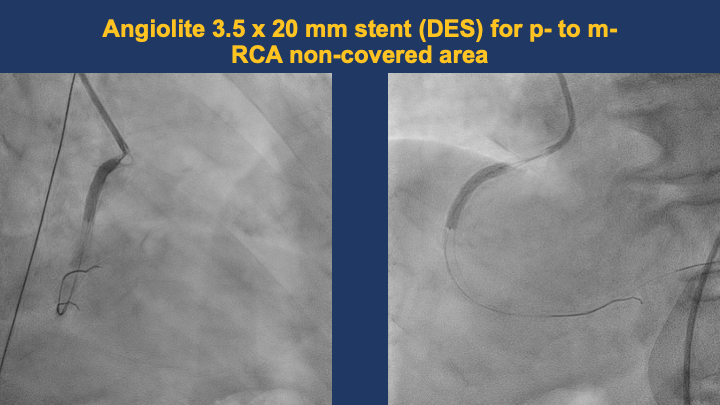
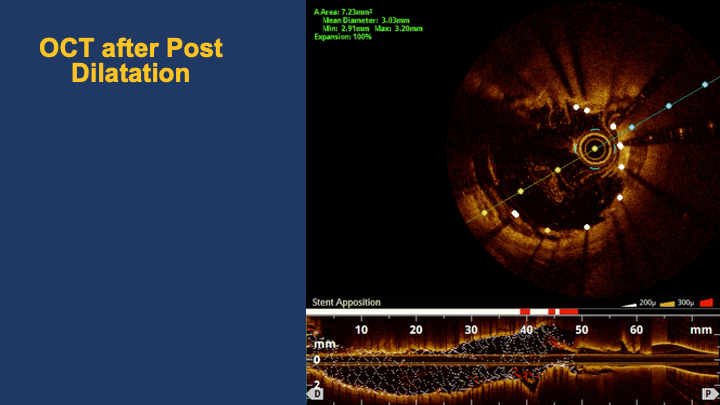
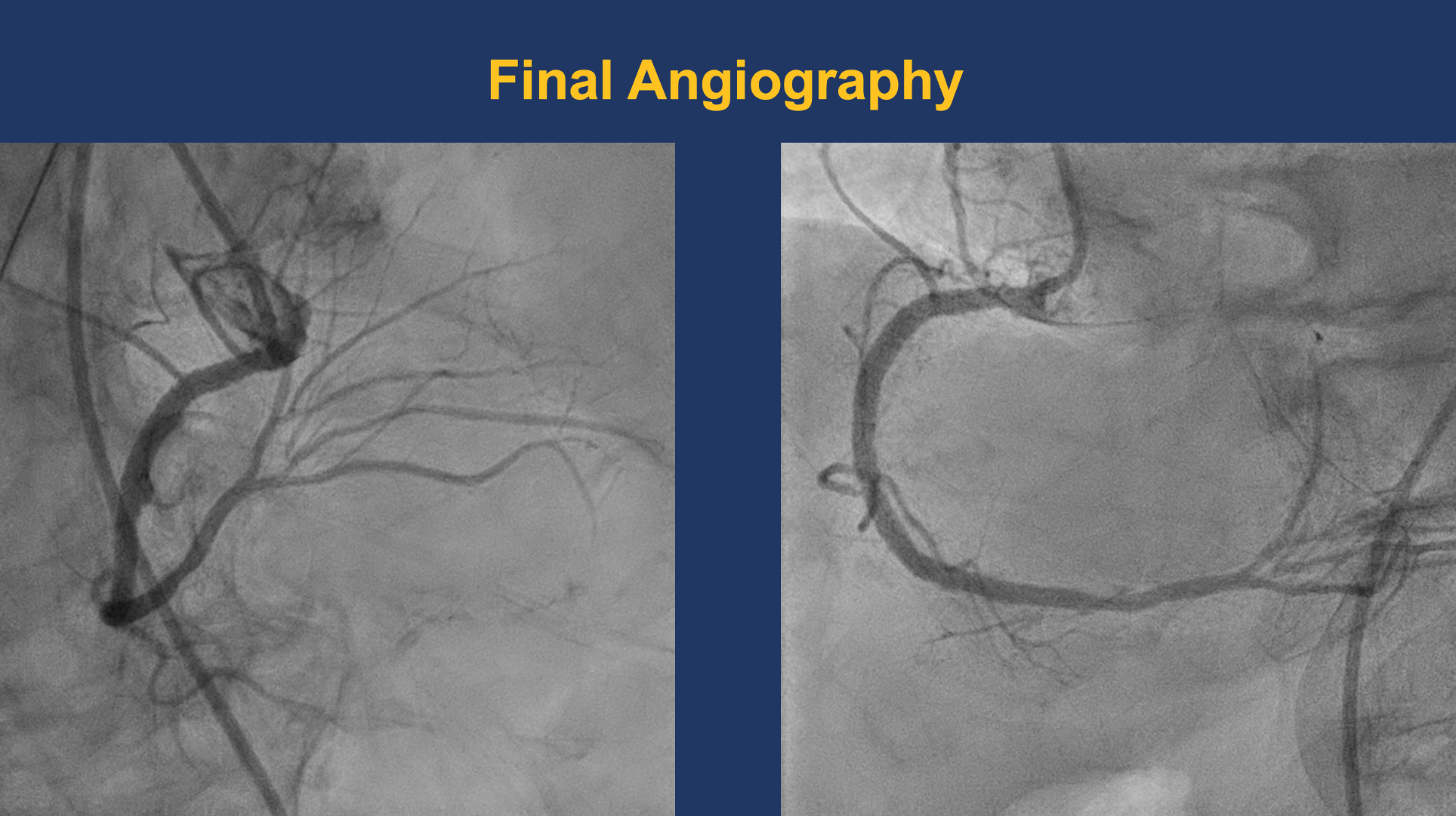
A JR 4.0 6F guiding catheter was successfully engaged at the RCA ostium. A Sion wire was advanced across the distal RCA lesion into the posterolateral branch, and a Sion Blue wire was placed in another PL branch for support.OCT pullback from the distal to proximal RCA confirmed the wire within the true lumen and demonstrated a minimal lumen area of 8.67 mm². Massive low-attenuating signals were observed, indicating the presence of white thrombus consistent with acute in-stent thrombosis. Notably, there was an uncovered segment without stent coverage and evidence of plaque rupture between the stents. No evidence of stent fracture or overlap with the distal stent.The lesion was predilated with a 3.0 × 20 mm NC Trek balloon inflated at 18–24 atm for 5–10 s (five inflations) and then with a 3.5 × 20 mm NC Trek balloon at 12–18 atm for 10 s (four inflations). Subsequently, a 3.5 × 20 mm Angiolite stent was deployed at the uncovered area of proximal-to-mid RCA.Post-dilatation was performed using a 3.5 × 20 mm NC Trek balloon (22–24 atm, three inflations) and a 3.75 × 8 mm NC Trek balloon (18 atm, six inflations).Repeat OCT revealed good stent expansion and apposition with resolution of the previous thrombus signal.Final angiography demonstrated well-expanded stents and restored TIMI 3 flow.
10. stenting 2.mov
Final OCt.mov
13. Post Dilate LAT.mov
Case Summary
OCT revealed acute in-stent thrombosis driven by white thrombus formation, plaque rupture, and an uncovered stent segment—mechanistic hallmarks of ISR in acute myocardial infarction. Intravascular imaging clarified the etiology beyond angiography, guiding mechanical correction with high-pressure post-dilatation and achieving optimal stent expansion and TIMI 3 flow. This case emphasizes that defining, identifying, and correcting ISR mechanisms are essential before definitive therapy.