Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251105_014
A Challenging Case Report of Anteroseptal Wall STEMI With LUCAS CPR in Cardiac Arrest During PCI and POT-PUFF Sign-Guided Revascularization in SVD PCI to LAD
By Lalitwadee Kingmaiklang, Wittawat Wattanasiriporn
Presenter
Lalitwadee Kingmaiklang
Authors
Lalitwadee Kingmaiklang1, Wittawat Wattanasiriporn1
Affiliation
Internal Medicine Department, Division of Cardiology, Rajavithi Hospital, Thailand1
View Study Report
CASE20251105_014
Coronary - Hemodynamic Support
A Challenging Case Report of Anteroseptal Wall STEMI With LUCAS CPR in Cardiac Arrest During PCI and POT-PUFF Sign-Guided Revascularization in SVD PCI to LAD
Lalitwadee Kingmaiklang1, Wittawat Wattanasiriporn1
Internal Medicine Department, Division of Cardiology, Rajavithi Hospital, Thailand1
Clinical Information
Relevant Clinical History and Physical Exam
A Thai 44-year-old man with history DVD with HFmrEF LVEF 44% status post PCI to LAD with 01DES in 2023, presented to emergency department with acute chest pain 5 hour PTA
He had history of Amphetamine used in every 3 months prior to presentation.
V/S: T 35.9 C, BP 145/95 mmHg, PR 102 bpm, RR 24 /min. PS 10/10
Heart : No surgical scar, no murmur, Lung: clear both lungs. Subcostal retraction
 Echo video 1.mp4
Echo video 1.mp4
12.53 LAD stent thrombosis.mp4
He had history of Amphetamine used in every 3 months prior to presentation.
V/S: T 35.9 C, BP 145/95 mmHg, PR 102 bpm, RR 24 /min. PS 10/10
Heart : No surgical scar, no murmur, Lung: clear both lungs. Subcostal retraction
Relevant Test Results Prior to Catheterization
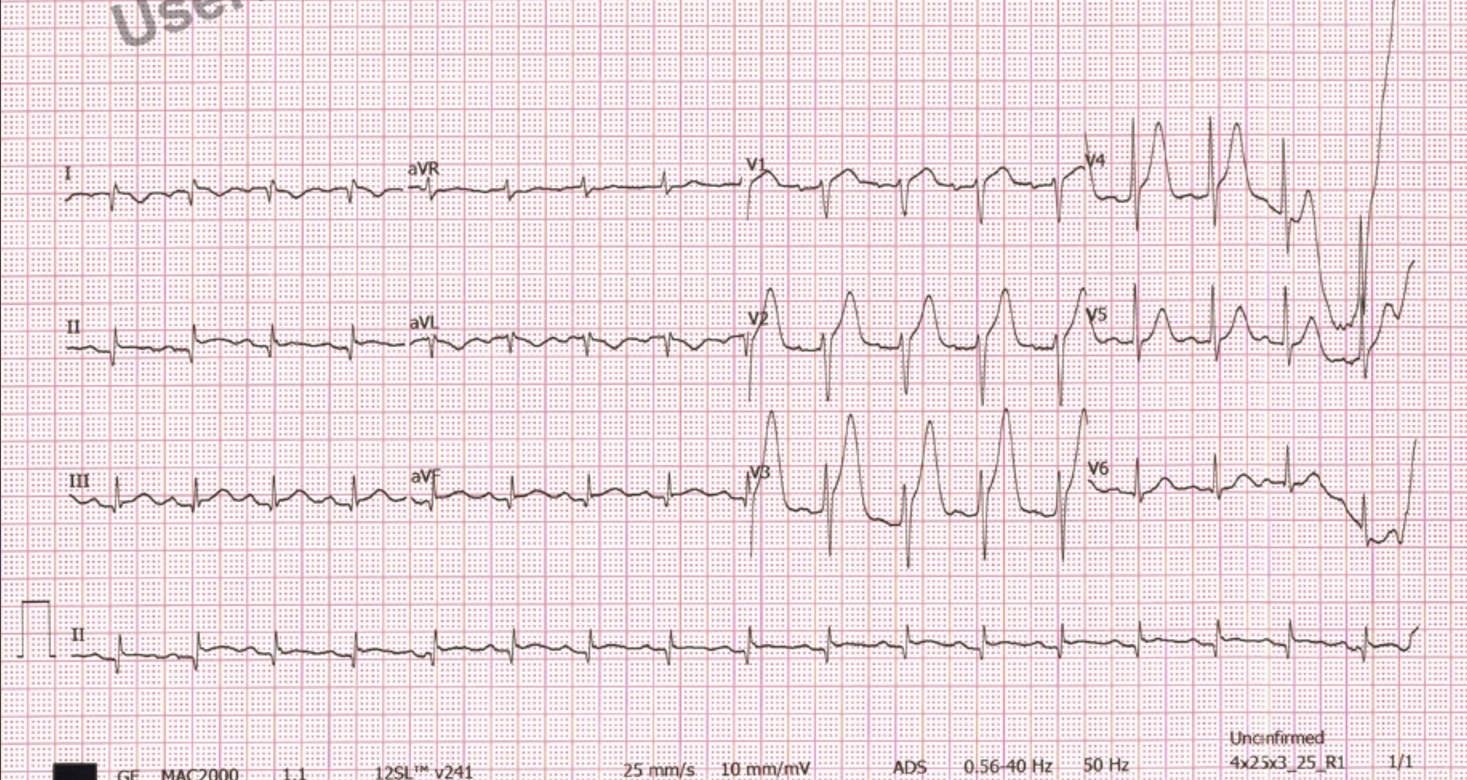
EKG showed normal sinus rhythm with ST segment elevation at V1-V4, Q wave in II III aVF.
Echocardiogram showed impaired LV systolic function, EF29.90% by Teichholz, 33.00 % by modified Simpson-biplane, global wall hypokinesia with anteroseptal wall hypokinesia at basal to apical LV part, Impaired RV systolic function. No significant VHD
1.18 sc balloon.mp4
Echocardiogram showed impaired LV systolic function, EF29.90% by Teichholz, 33.00 % by modified Simpson-biplane, global wall hypokinesia with anteroseptal wall hypokinesia at basal to apical LV part, Impaired RV systolic function. No significant VHD
Relevant Catheterization Findings
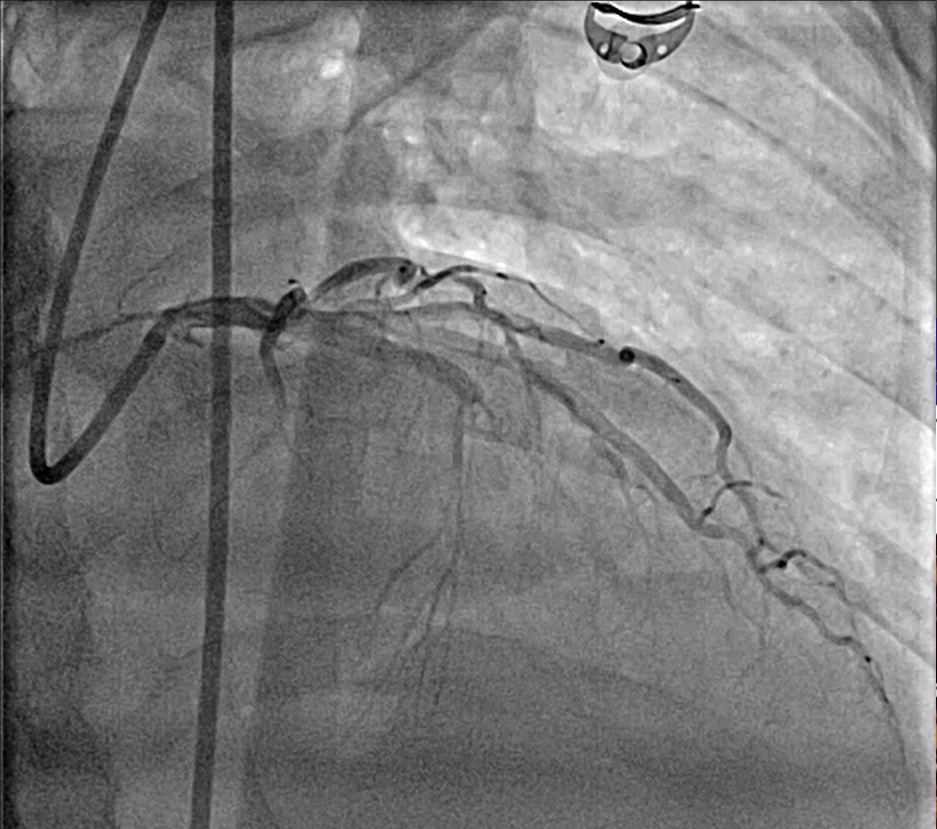
CAG was performed with Right femoral approach with Dx catheterJR 6/4 Fr, GD EBU 7/3.5 Fr showed
Right dominant
LM : normal.
LAD : total occlusion LAD stent thrombosis.
LCx : normal.
RCA : normal.
1.24 pot puff sign.mp4
Right dominant
LM : normal.
LAD : total occlusion LAD stent thrombosis.
LCx : normal.
RCA : normal.
Interventional Management
Procedural Step
Patient arrived to procedure lab
Then consciousness E1VTM1 , ECG rhythm PEA
Patient on Lucus, start Adrenaline 1 mg IV(Then run every 4 minutes), On external defibrillator pads.
CAG was performed with Right femoral approach with Dx catheterJR 6/4 Fr, GD EBU 7/3.5 Fr showed
Right dominant
LM : normal.
LAD : total occlusion LAD stent thrombosis.
LCx : normal.
RCA : normal.
On Lucas CPR Proceed directly to PCI of LAD,
Guiding : EBU 7/3.5 to LCA
Guide wire : Turntrac to LAD
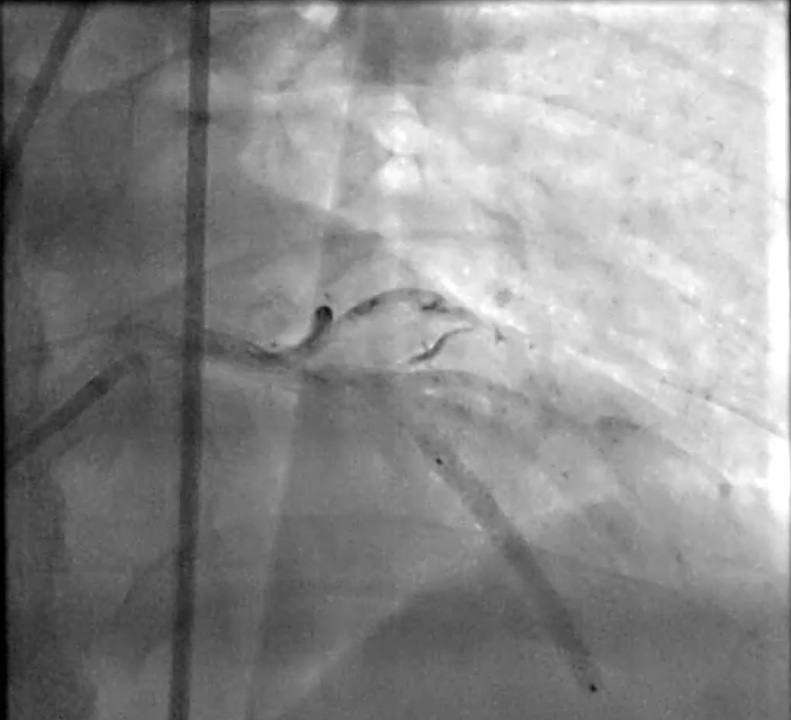
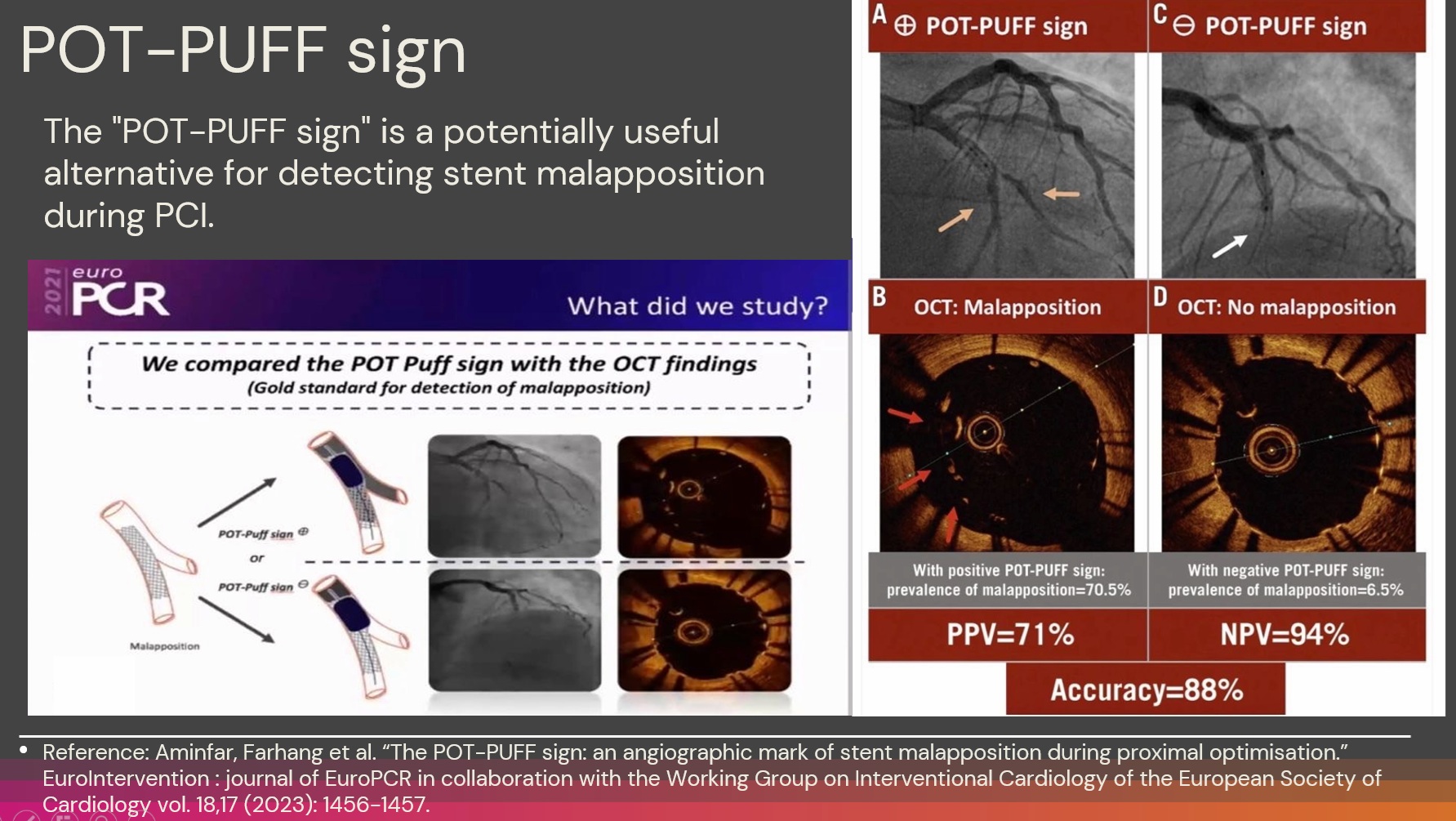
Pre dilatation : SC balloon 2.0 x 15 inflated mLAD upto 12 atm, inserted IVUS to LAD IVUS revealed neoatherosclerotic mLAD stent, SC balloon 3.0 x 15 mm inflated mLAD upto 12 atm, Rapamycin eluting stent 3.5 x 31 mm deployed mLAD upto 12 atm with POT Puff sign. Acceptable angiographic result.
Case Summary
Key principles in cardiac arrest management during PCI: prompt recognition of the arrest rhythm, initiation of high‐quality CPR, immediate consideration for mechanical support when appropriate, and rapid revascularization.
The LUCAS device can provides consistent mechanical chest compressions and can be effectively employed for CPR in the cardiac catheterization laboratory setting.
The role of LUCAS and similar devices continues to evolve.
There is growing support for their use not only as a bridge during resuscitation but also in procedural facilitation for complex coronary interventions in patients with cardiac arrest.
Intravascular imaging is beneficialindetermining mechanism of CAD, informing therapeutic strategy and confirmingeffective treatment of PCI.