Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251105_013
Electrical Chaos to Optimal Flow: Managing Inferior STEMI With ST-Segment Elevation in PVCs
By Apichart Setthajit, Wittawat Wattanasiriporn
Presenter
Apichart Setthajit
Authors
Apichart Setthajit1, Wittawat Wattanasiriporn1
Affiliation
Rajavithi Hospital, Thailand1
View Study Report
CASE20251105_013
Coronary - DES/BRS/DCB
Electrical Chaos to Optimal Flow: Managing Inferior STEMI With ST-Segment Elevation in PVCs
Apichart Setthajit1, Wittawat Wattanasiriporn1
Rajavithi Hospital, Thailand1
Clinical Information
Relevant Clinical History and Physical Exam
A 69 year-old Thai woman with hypertension and dyslipidemia. She presented to the emergency department with acute chest pain for 5 hrs prior to admission, chest pain radiates to left shoulder without dyspnea and orthopnea. Vital signs: BT 36.9 C BP 137/81 mmHg PR 66 bpm RR 16/min. Cardiovascular examinations are unremarkable, without jugular venous distension or murmur and gallops. Pulmonary examinations are unremarkable.
Relevant Test Results Prior to Catheterization
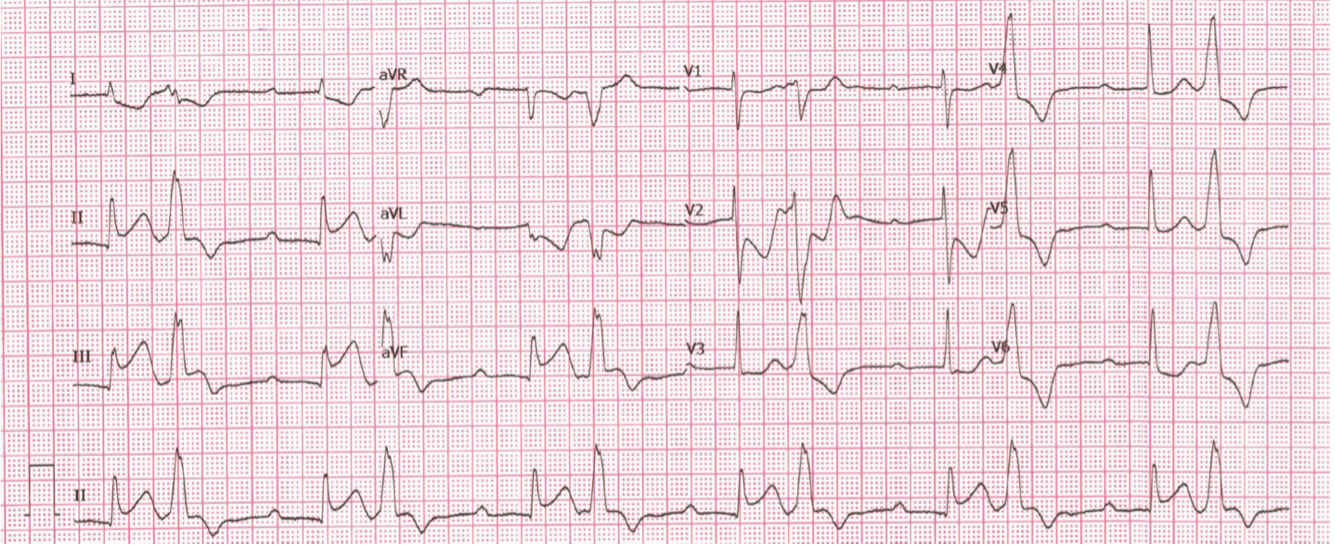
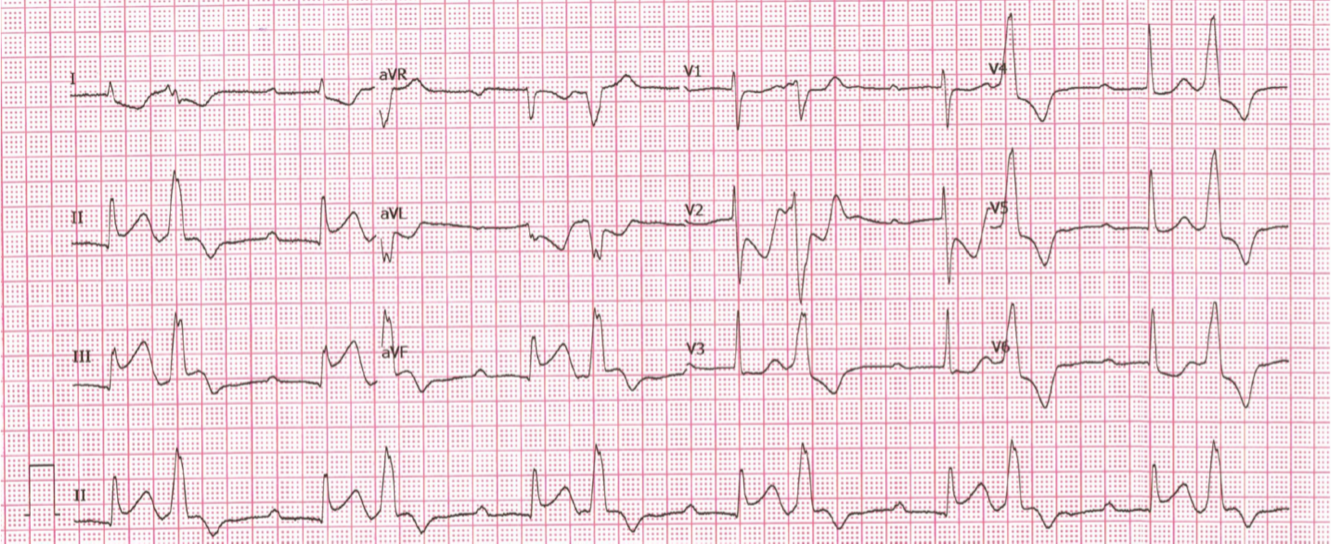
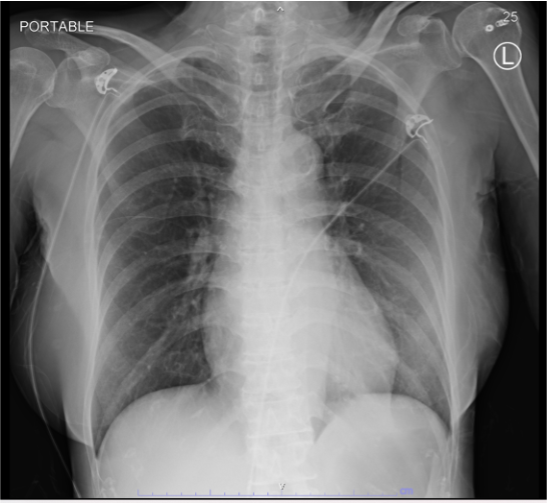
Electrocardiogram (ECG) was performed-showing sinus rhythm 60 bpm with ST-segment elevation in leads II, III, aVF, ST-segment depression in leads I, aVL. ECG show AV dissociation develop to 3rd degree AV block and present bigeminy ST segment elevation PVCs . CXR no pulmonary congestion . High sensitivity troponin-I was requested with highly elevated result as 1,957 ng/L. Echocardiogram showed LVEF 50%, Inferior, inferoseptal and inferolateral wall hypokinesia
 PLAX.mp4
PLAX.mp4
PSAX_Basal.mp4
Relevant Catheterization Findings
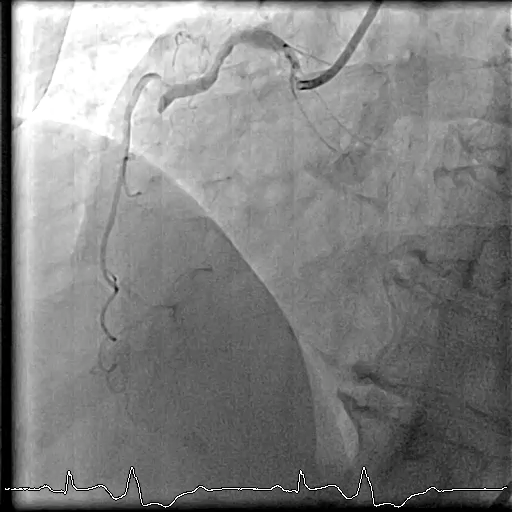
Right femoral approach with JL6/4, JR 6/4 diagnostic catheter show total occlusion mRCA, 30% stenosis at proximal-LAD, 90% stenosis at mid-LAD, 95% stenosis mid-LCx.
Rt_LAO__CRA.mp4
Balloon_Dilate.mp4
Potpuff_LAO.mp4
Interventional Management
Procedural Step
Cardiac catheterization was performed via right femoral approach with JL6/4, JR 6/4 diagnostic catheter show total occlusion mRCA, 30% stenosis at proximal-LAD, 90% stenosis at mid-LAD, 95% stenosis mid-LCx. PCI with JR 6/4. PCI to mid-RCA. GD: JR 6/4. Turntrac with Guidezilla to RCA. SC balloon 2.0x12 mm inflated mRCA up to 12 atm. Rapamycin eluting stent 3.0x18 mm deployed mRCA 12 atm with POT-PUFF sign technique. The final angiogram was acceptable result. After successful reperfusion of the right coronary artery, the premature ventricular complexes (PVCs) was subsides.

Balloon_Dilate.mp4
Potpuff sign.mp4
Final_RCA.mp4
Case Summary
STEMI patterns can occasionally be observed during premature ventricular contractions (PVCs), which may assist in establishing the diagnosis of STEMI. It is important to take advantage of all available information, as PVCs can often provide valuable diagnostic clues.In this case, successful restoration of RCA flow resulted in resolution of conduction disturbances and PVCs. POT-PUFF sign technique during PCI. This method allows real-time confirmation of optimal stent expansion and apposition.