Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251105_011
Impella-Assisted Complex PCI for Ischemic Cardiomyopathy With Very Low Ejection Fraction and Triple-Vessel Disease: From Cardiogenic Instability to Complete Revascularization
By Chen Shu Wu, Yen-Lien Chou
Presenter
Chen Shu Wu
Authors
Chen Shu Wu1, Yen-Lien Chou2
Affiliation
Tri-Service General Hospital, National Defense Medical University, Taiwan1, Tri-Service General Hospital, National Defense Medical Center, Taiwan2
View Study Report
CASE20251105_011
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
Impella-Assisted Complex PCI for Ischemic Cardiomyopathy With Very Low Ejection Fraction and Triple-Vessel Disease: From Cardiogenic Instability to Complete Revascularization
Chen Shu Wu1, Yen-Lien Chou2
Tri-Service General Hospital, National Defense Medical University, Taiwan1, Tri-Service General Hospital, National Defense Medical Center, Taiwan2
Clinical Information
Relevant Clinical History and Physical Exam
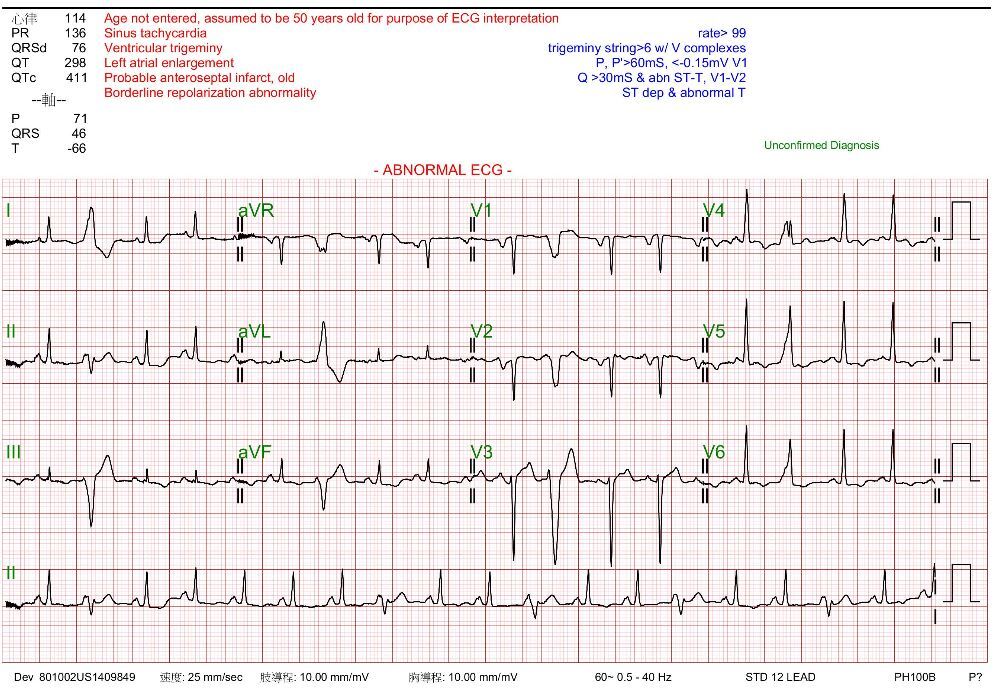
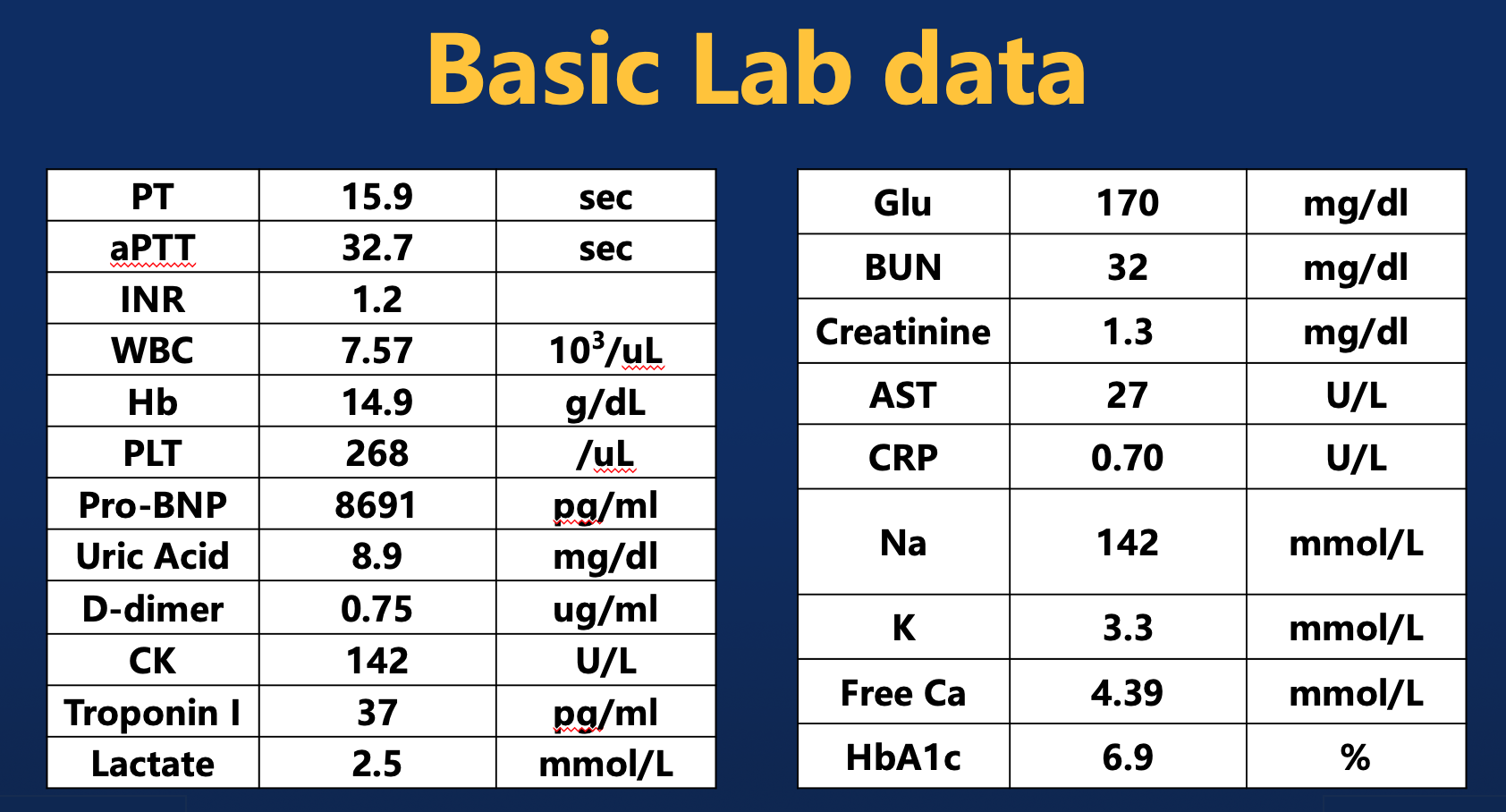
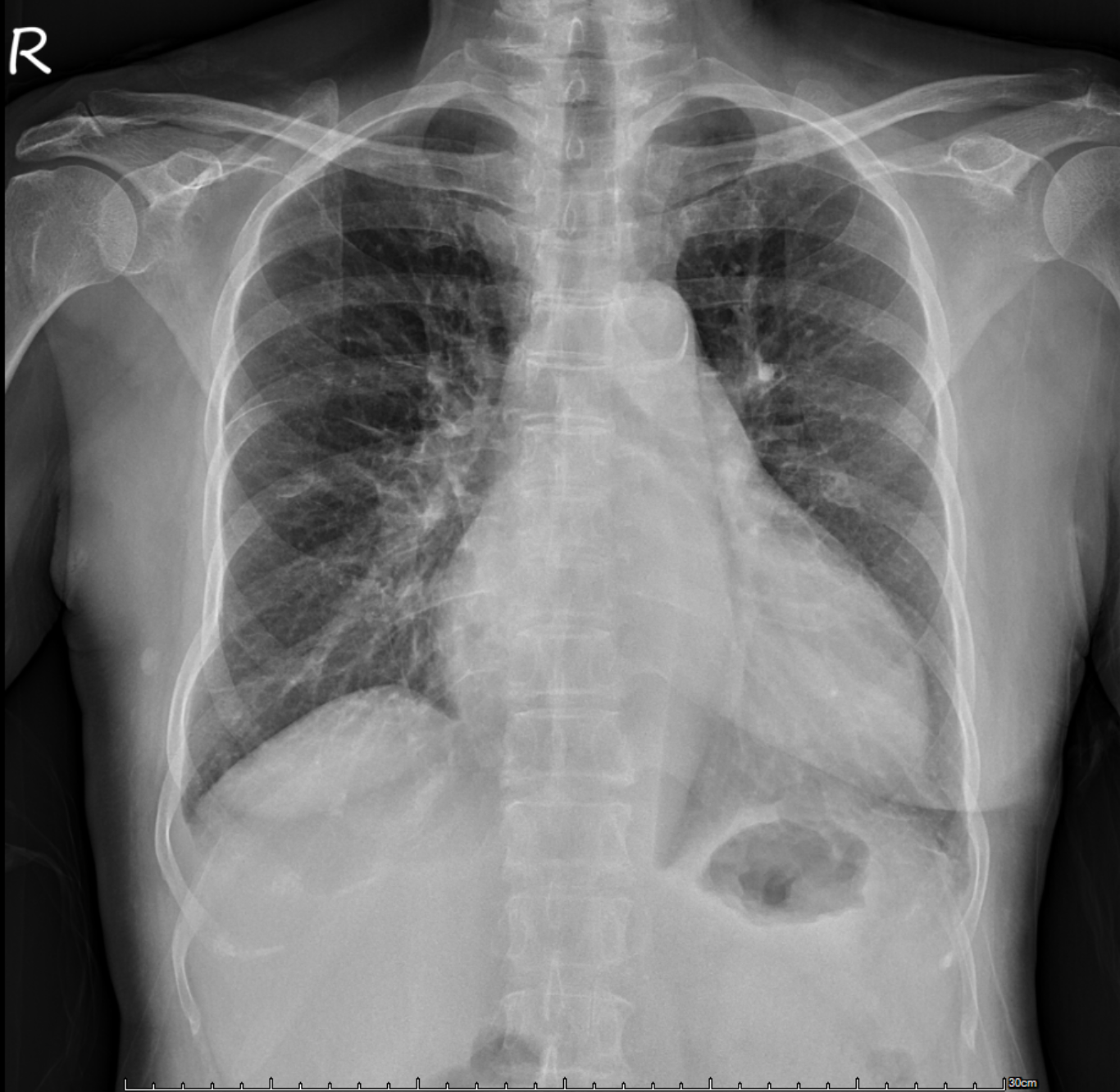
A 72-year-old woman with paroxysmal AFL, severe MR, DM, HTN, and HLD presented with 2 months of progressive dyspnea, orthopnea, and worsening bilateral leg swelling. On exam, she was dyspneic in the upright position, with elevated JVP, 3+ pitting edema, and a loud apical holosystolic murmur.
Relevant Test Results Prior to Catheterization
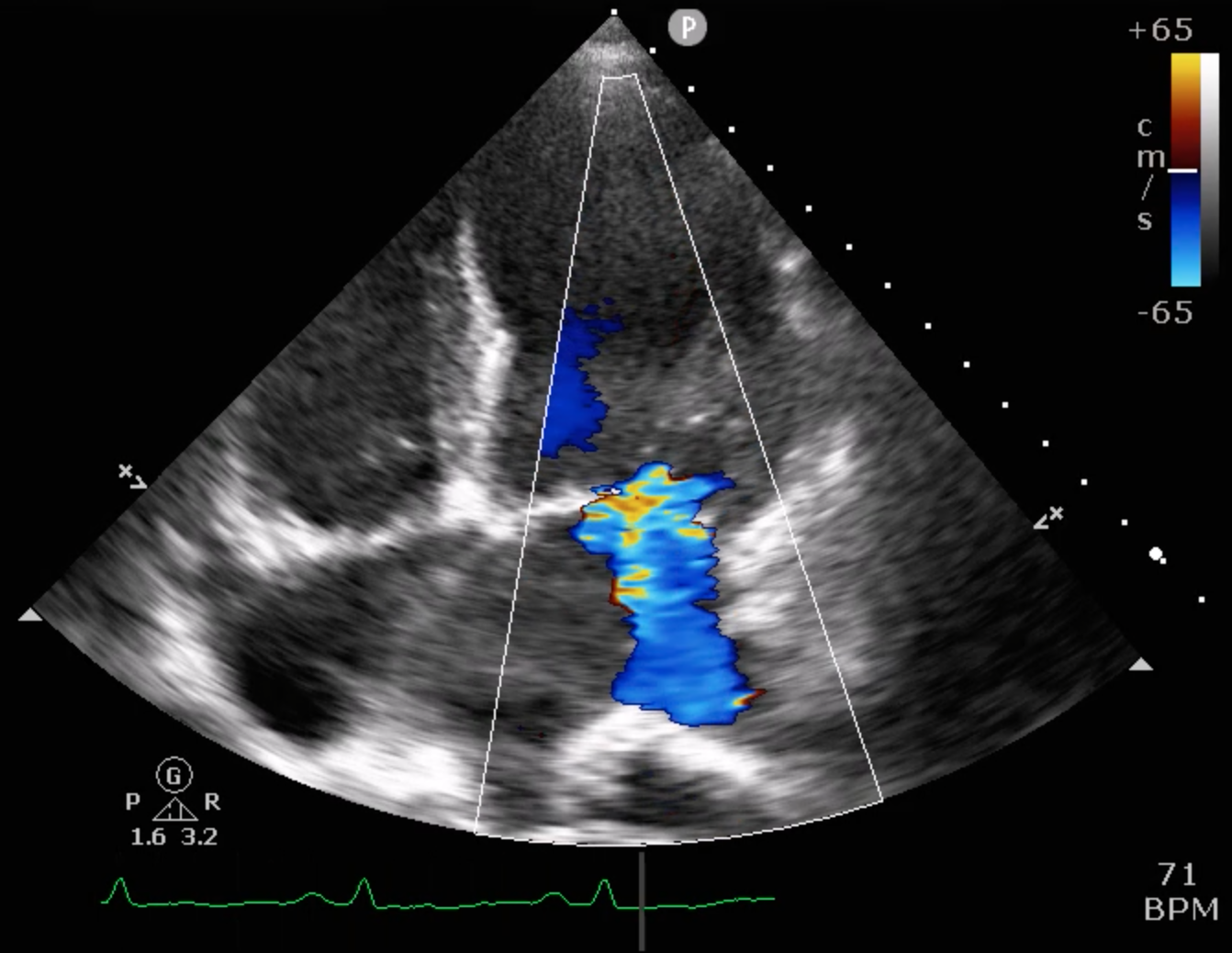
Echocardiography showed severely reduced LV systolic function with an EF around 20%, global hypokinesia, and anterior septal hypokinesia. Severe mitral regurgitation with left atrial enlargement was noted. Mild RV dysfunction was present, and Doppler suggested elevated filling pressures. These findings were obtained prior to catheterization.
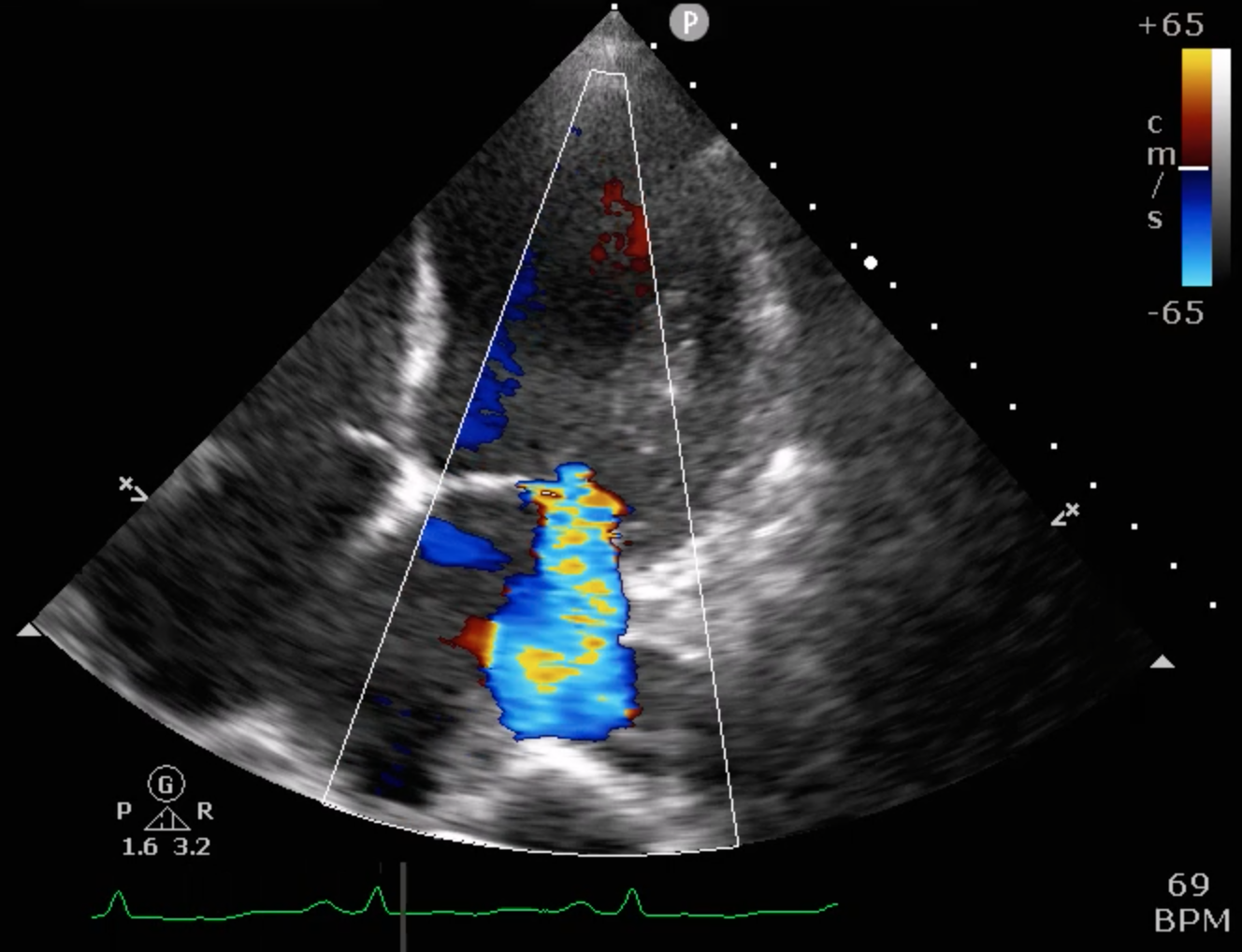
 8_6 ECHO 4 chamber MR+++.mp4
8_6 ECHO 4 chamber MR+++.mp4
8_6 ECHO 4 chamber.mp4
8_6 ECHO long asix.mp4
Relevant Catheterization Findings
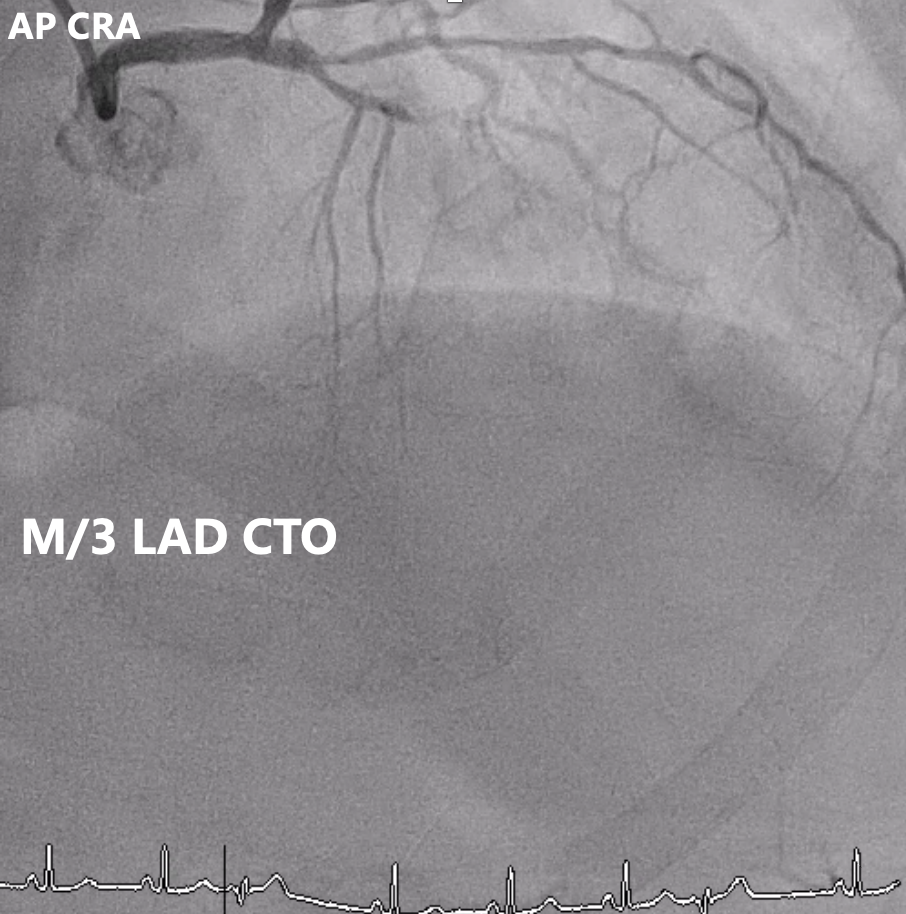
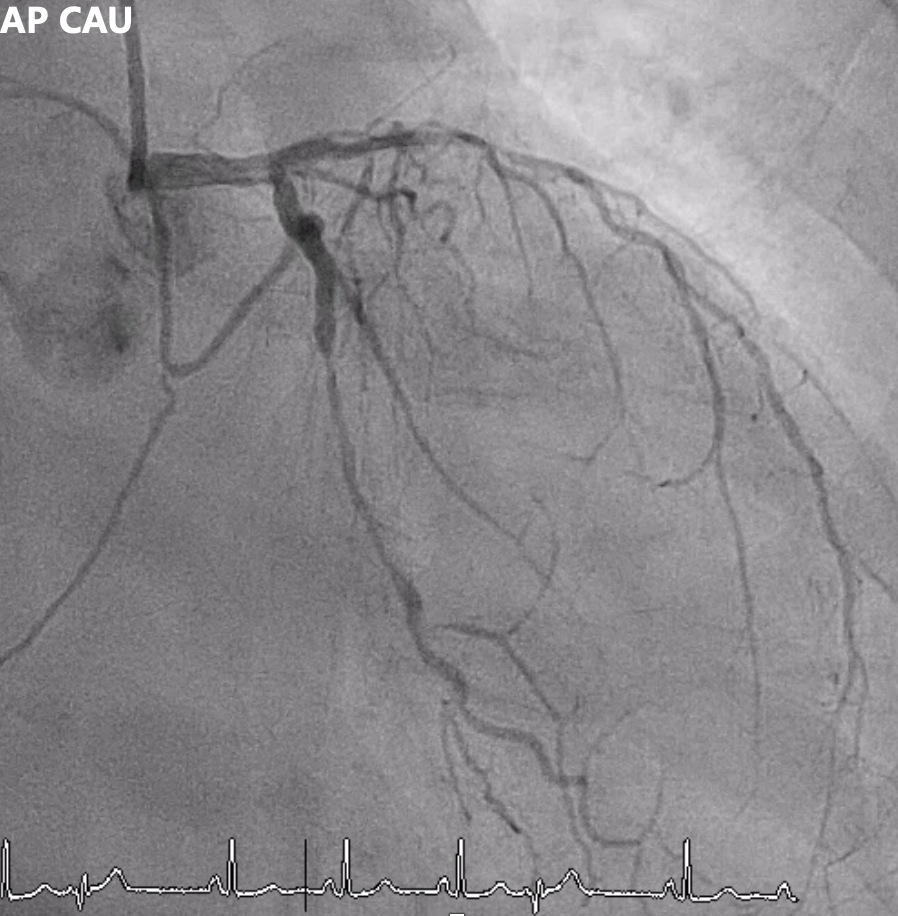
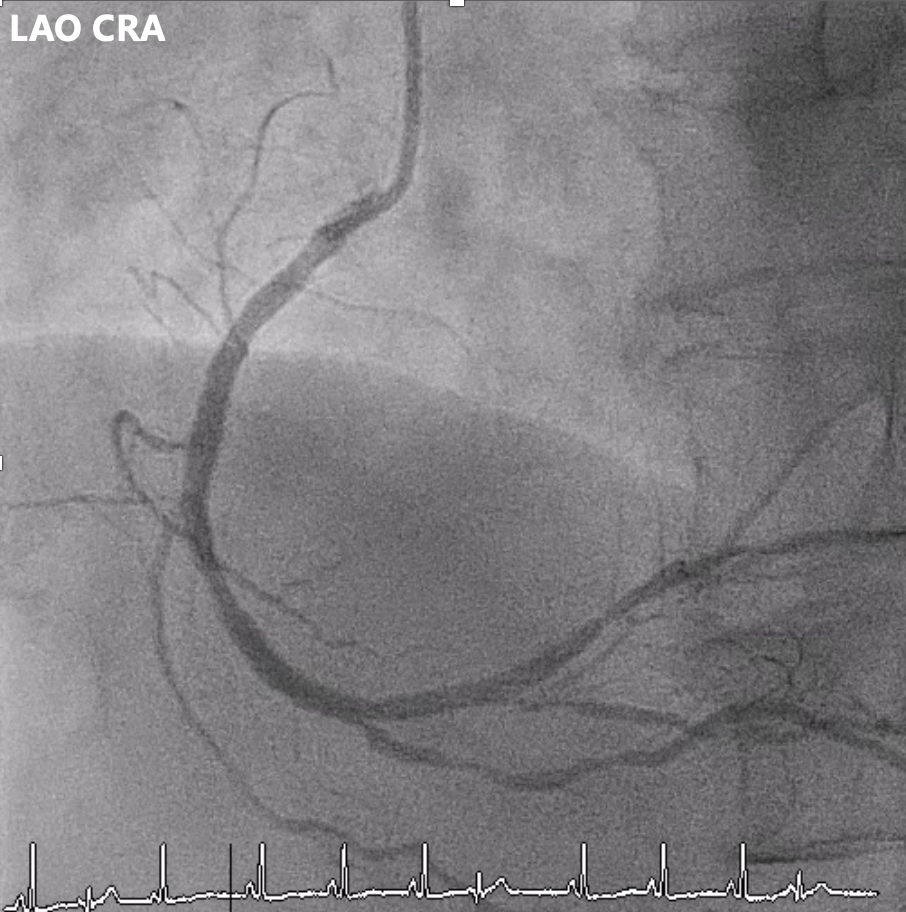
Angiography showed multivessel atherosclerosis with the LAD being the most critical lesion. The mid LAD had tubular eccentric 70–80% stenosis with a Medina (0,1,1) bifurcation and a mid-segment CTO (~2 cm, blunt end). DB1 had 70–80% ostial stenosis with 50–70% diffuse disease, and DB2 had a short CTO with distal collateral flow from DB1. Other vessels had non-critical or moderate diffuse disease.
Left AP CAU.mp4
Left RAO CRA.mp4
Right AP CRA.mp4
Interventional Management
Procedural Step
Impella Placement:
Left CFA was accessed under fluoroscopy/ultrasound, a 14 Fr sheath inserted, and a pigtail advanced into the LV before exchanging to the Impella system. The device was positioned across the aortic valve to 76 cm with correct waveforms. Adequate support was achieved. Atrial flutter occurred and was cardioverted with 100 J.LAD Intervention:
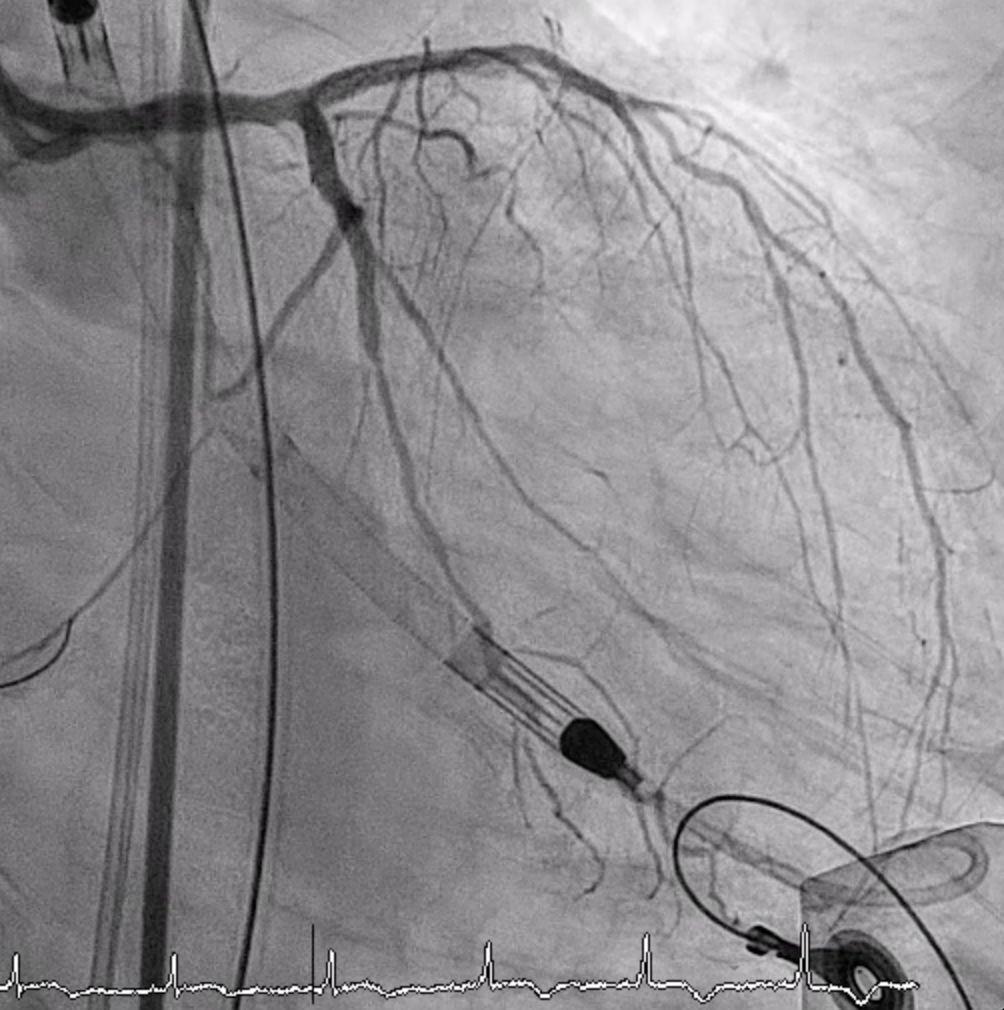
LMCA was engaged with an EBU 3.5. Several wires failed to cross the p-LAD CTO, but Gaia 1st entered the true lumen and advanced to DB2 via Finecross. Small-balloon predilation (1.2–2.0 mm) was done. IVUS confirmed true lumen and MLA 2.43 mm² at the CTO entry. A double-catheter Sasuke technique enabled CTO crossing. A 2.0×38 mm X-Skypoint stent was deployed, followed by POT and high-pressure post-dilation, achieving TIMI 3 flow.LCX Intervention:
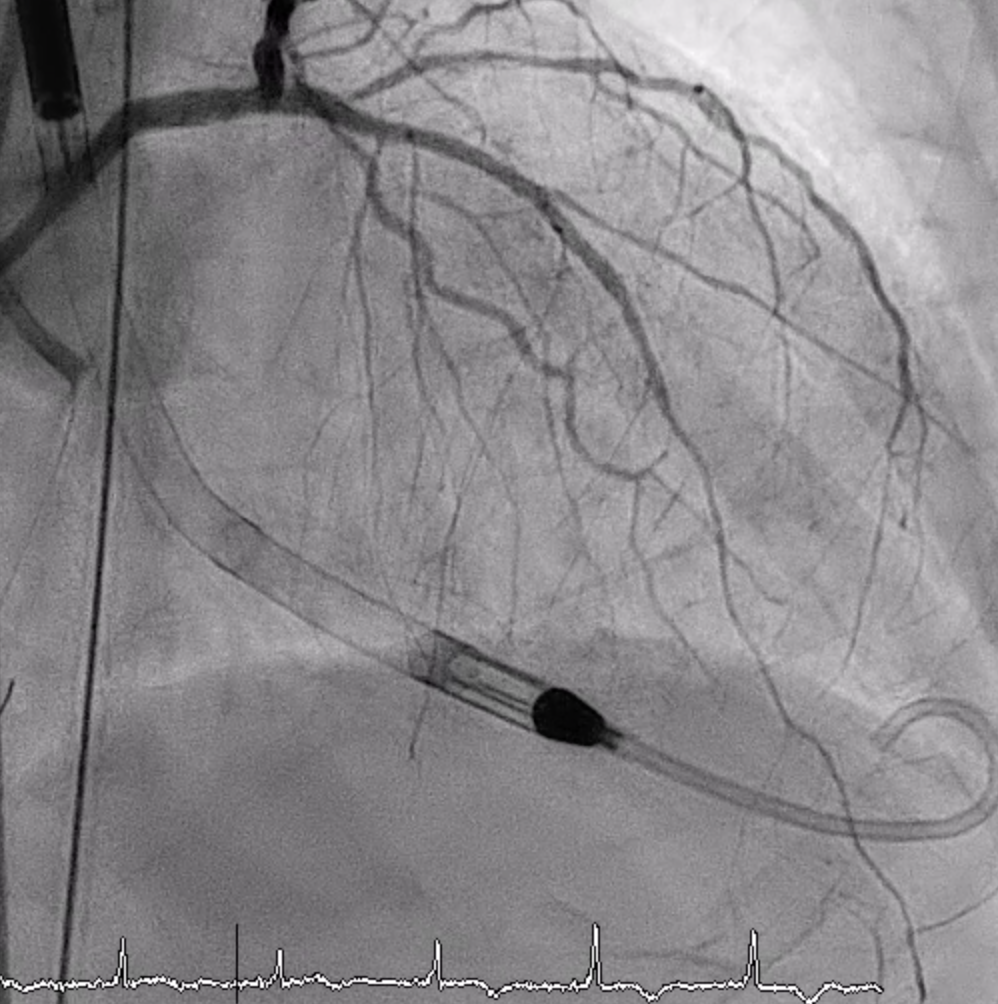
A wire was advanced to distal LCx. IVUS showed MLA 2.24 mm². The ostial–proximal LCx was dilated with 2.0–2.75 mm NC balloons, followed by a 2.75×12 mm X-Skypoint stent and post-dilation. Final IVUS showed good expansion (MSA 5.93 mm²) without LAD protrusion. TIMI 3 flow achieved.RCA Intervention:
IVUS showed MLA 2.27 mm². PL and mid-RCA lesions were dilated with 2.5–3.0 mm NC balloons. A 3.0×24 mm Nagomi stent was deployed and further dilated with a 3.5 mm balloon. Final angiography showed TIMI 3 flow.
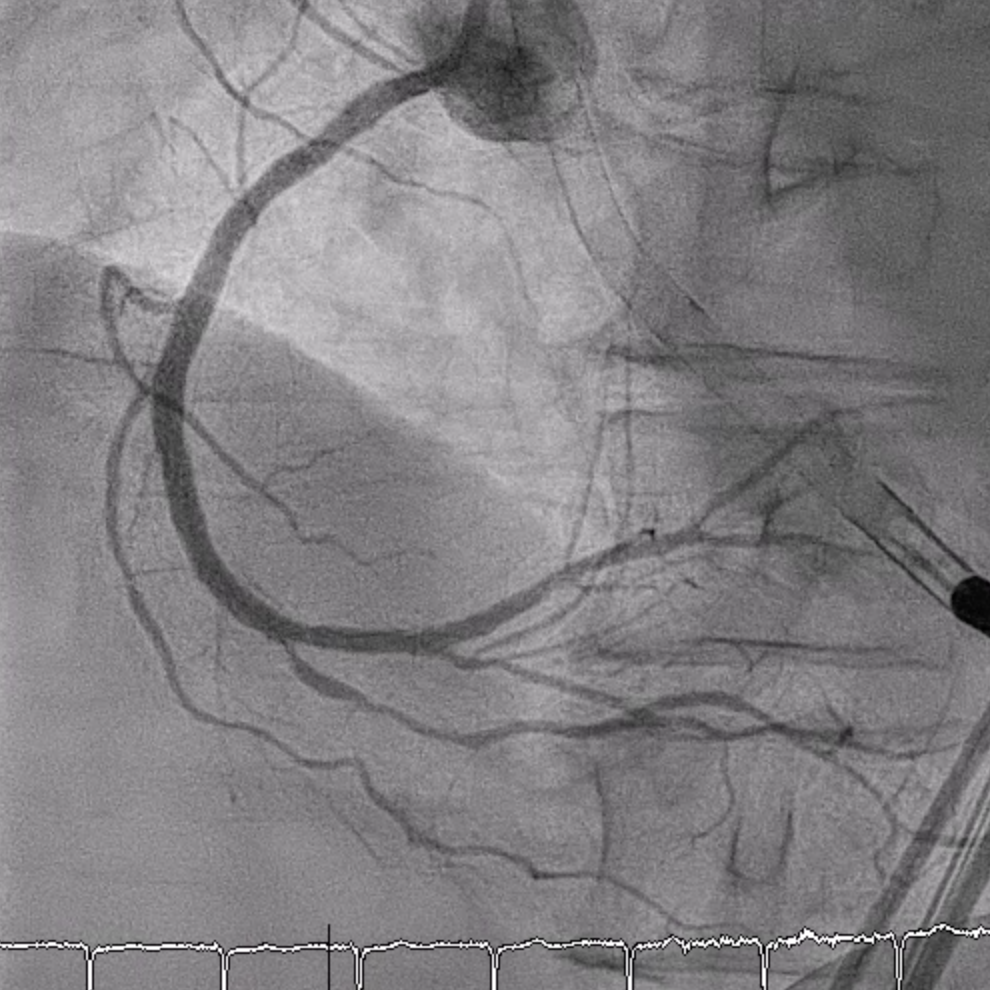
RCA LAO CRA Final.mp4
LCx Final RAO CAU.mp4
Final LAD.mp4
Left CFA was accessed under fluoroscopy/ultrasound, a 14 Fr sheath inserted, and a pigtail advanced into the LV before exchanging to the Impella system. The device was positioned across the aortic valve to 76 cm with correct waveforms. Adequate support was achieved. Atrial flutter occurred and was cardioverted with 100 J.LAD Intervention:
LMCA was engaged with an EBU 3.5. Several wires failed to cross the p-LAD CTO, but Gaia 1st entered the true lumen and advanced to DB2 via Finecross. Small-balloon predilation (1.2–2.0 mm) was done. IVUS confirmed true lumen and MLA 2.43 mm² at the CTO entry. A double-catheter Sasuke technique enabled CTO crossing. A 2.0×38 mm X-Skypoint stent was deployed, followed by POT and high-pressure post-dilation, achieving TIMI 3 flow.LCX Intervention:
A wire was advanced to distal LCx. IVUS showed MLA 2.24 mm². The ostial–proximal LCx was dilated with 2.0–2.75 mm NC balloons, followed by a 2.75×12 mm X-Skypoint stent and post-dilation. Final IVUS showed good expansion (MSA 5.93 mm²) without LAD protrusion. TIMI 3 flow achieved.RCA Intervention:
IVUS showed MLA 2.27 mm². PL and mid-RCA lesions were dilated with 2.5–3.0 mm NC balloons. A 3.0×24 mm Nagomi stent was deployed and further dilated with a 3.5 mm balloon. Final angiography showed TIMI 3 flow.
Case Summary
This case shows that Impella-assisted complex PCI provided effective hemodynamic support in a patient with ischemia cardiomyopathy with reduced ejection fraction and triple-vessel disease, enabling complete revascularization under stable conditions. The device was removed immediately after PCI, and the patient recovered well, being discharged one week later. This highlights the value of mechanical circulatory support in enhancing safety and outcomes in high-risk PCI.