Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251105_010
Successful Retrieval of an Entrapped Rotational Atherectomy Burr Using False Lumen-Delivered Intravascular Lithotripsy
By Toku Sakashita
Presenter
Toku Sakashita
Authors
Toku Sakashita1
Affiliation
IMS Fujimi General Hospital, Japan1
View Study Report
CASE20251105_010
Coronary - Complication Management
Successful Retrieval of an Entrapped Rotational Atherectomy Burr Using False Lumen-Delivered Intravascular Lithotripsy
Toku Sakashita1
IMS Fujimi General Hospital, Japan1
Clinical Information
Relevant Clinical History and Physical Exam
A 68-year-old woman was admitted to our hospital with acute decompensated heart failure. Her medical history included hypertension, type 2 diabetes mellitus, dyslipidaemia, and a prior percutaneous coronary intervention (PCI) for anterior myocardial infarction, with stent implantation in the left anterior descending artery.
The condition was easily compensated with diuretics.
Relevant Test Results Prior to Catheterization
Chest radiography showed pulmonary congestion, and transthoracic echocardiography demonstrated a left ventricular ejection fraction of 36%. Laboratory findings revealed an estimated glomerular filtration rate (eGFR) of 59.4 ml/min/1.73 m², B-type natriuretic peptide (BNP) level of 2415.1 pg/ml, and high-sensitivity troponin I level of 48 pg/ml.
Relevant Catheterization Findings
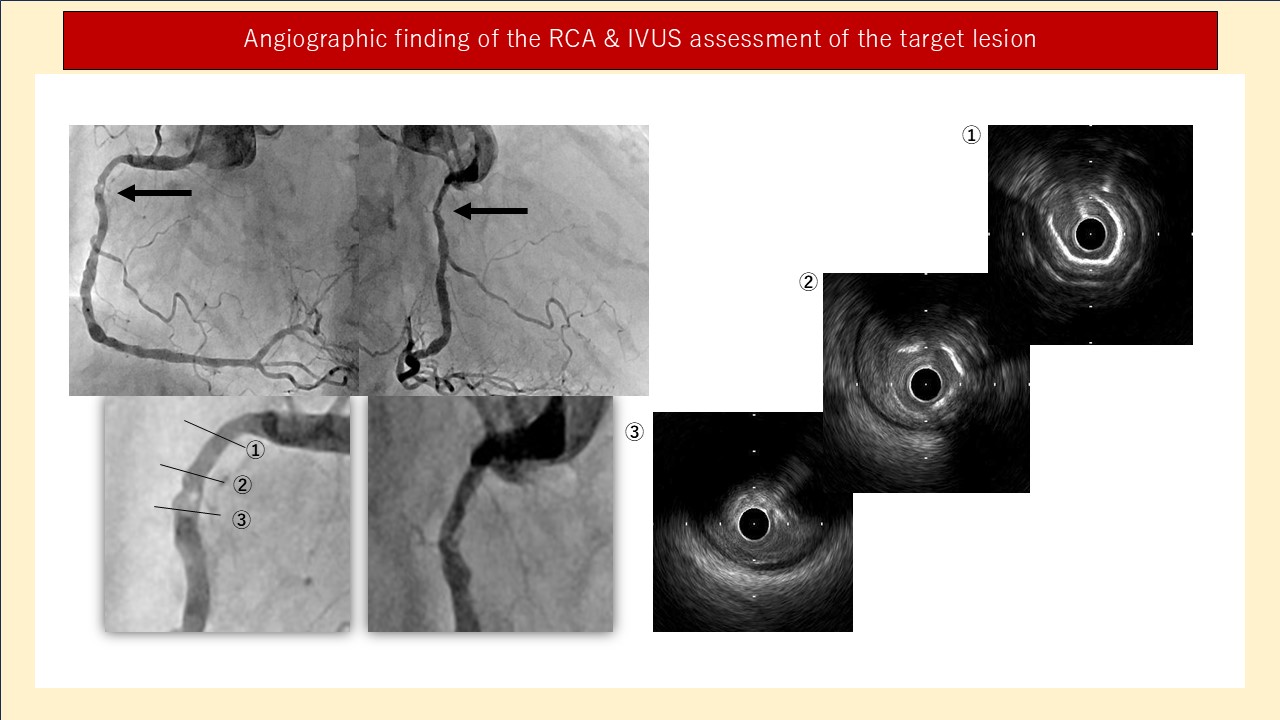
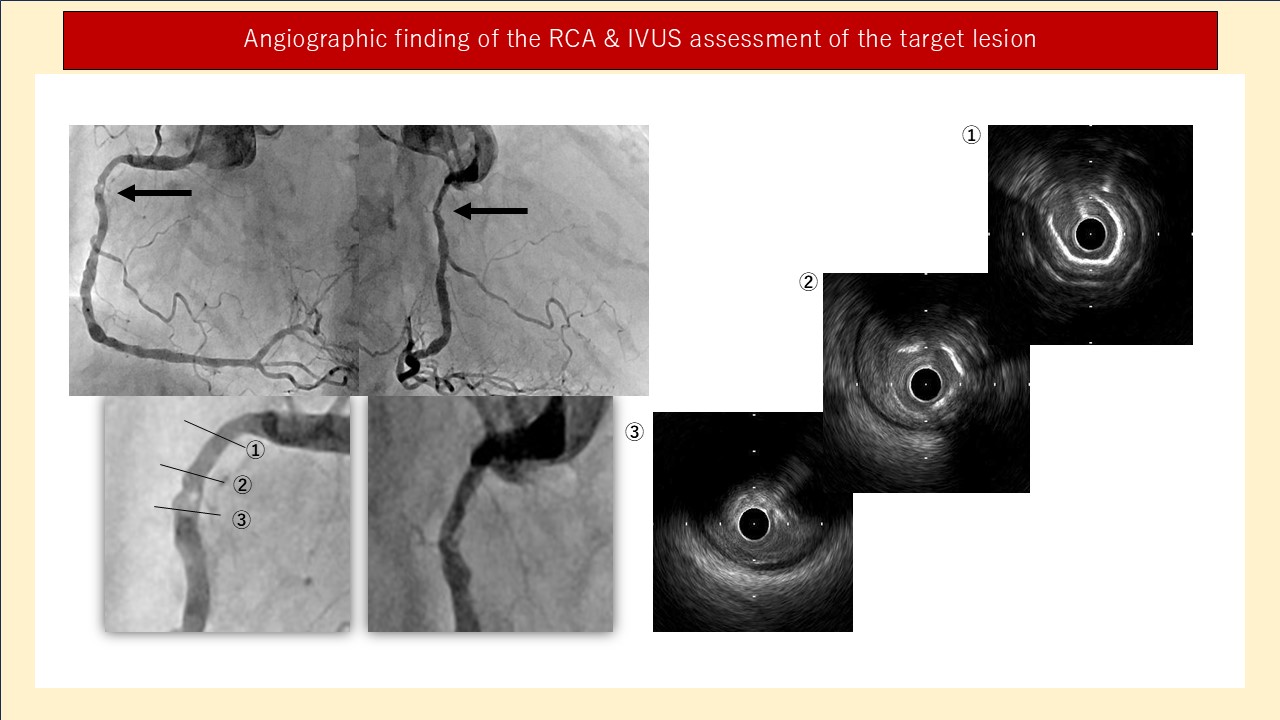
coronary angiography was performed, which revealed 75% stenosis in segment #1, 90% stenosis in segment #2, maintained patency of the previously implanted stent in segment #7, and 90% stenosis in both segments #13 and #15. Revascularisation of the right coronary artery (RCA), particularly at segment #2, was planned as the culprit lesion.
Interventional Management
Procedural Step
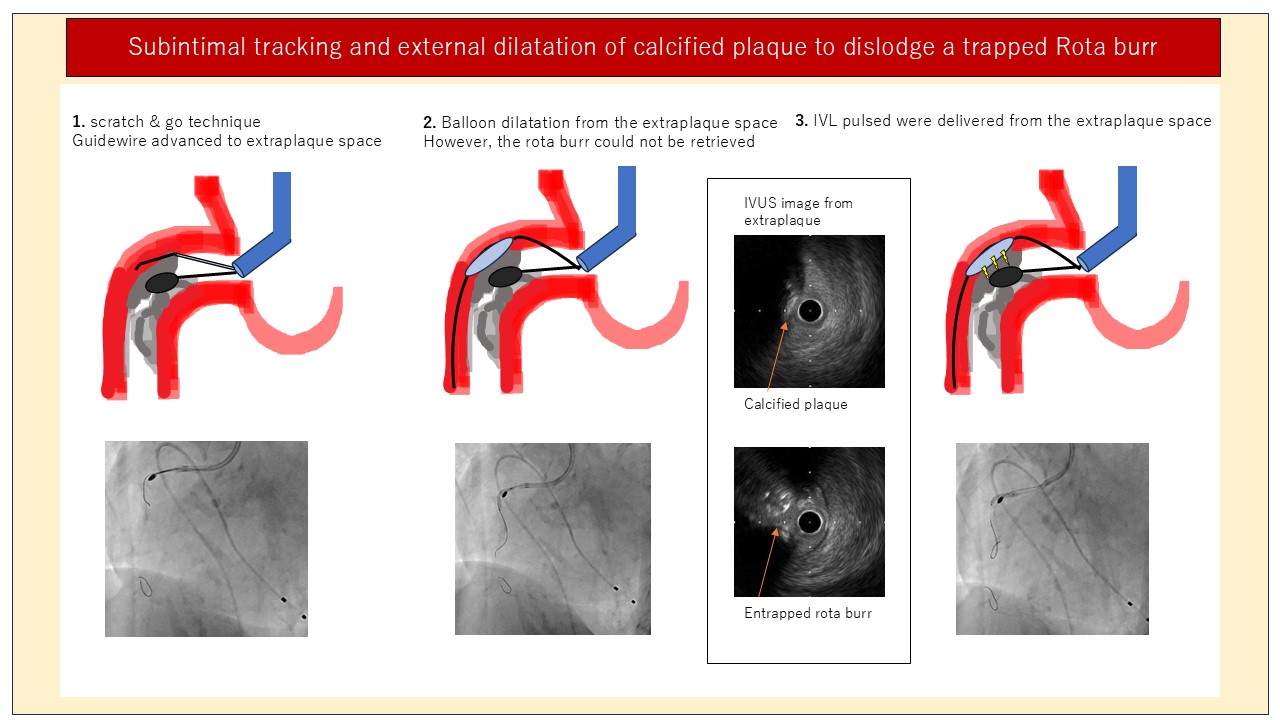
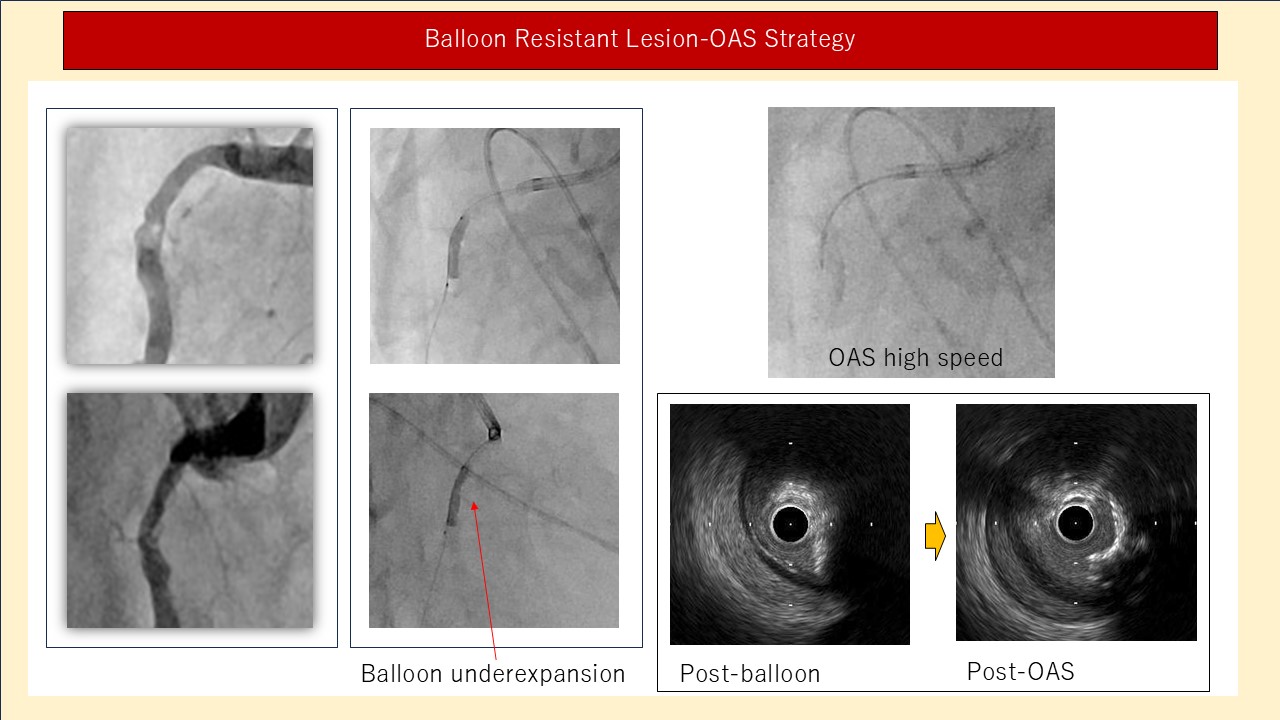
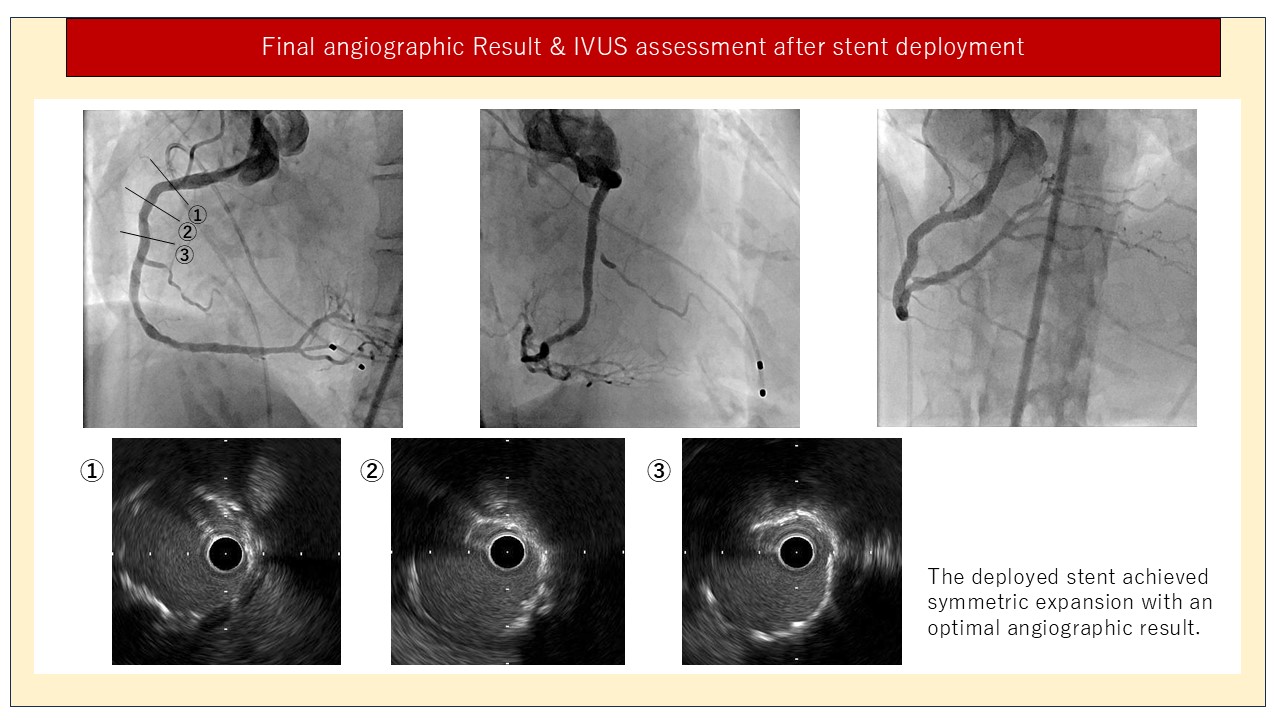
PCI was performed via a 7 Fr femoral approach using an AL 1.5 guiding catheter. A Sion guidewire crossed the lesion, and IVUS confirmed concentric calcification. RA was initiated with a 2.0 mm burr under Dynaglide mode. During advancement across segment #1, the burr became immobile within dense calcification. Repeated traction failed to free it. Parallel wiring using multiple wires was unsuccessful. A high-tip-load polymer-jacketed guidewire, designed for peripheral intervention, was advanced distally and entered the false lumen. Contrast injection via a guide extension confirmed its subintimal course adjacent to the burr. Balloon dilatation (2.0 mm at 6 atm) from the false lumen failed to release the burr. IVUS imaging revealed the burr tightly compressed between circumferential calcium. IVL was performed from the false lumen using a 2.5 × 12 mm Shockwave balloon, delivering 80 pulses. After lithotripsy, gentle traction allowed the burr to be retrieved safely without perforation. IVUS confirmed re-entry into the true lumen. Further plaque modification was achieved using orbital atherectomy (Diamondback 360®, Cardiovascular Systems, MN, USA) and a 3.0 × 10 mm Wolverine cutting balloon, followed by implantation of a 3.5 × 48 mm Synergy XD drug-eluting stent (Boston Scientific). Final angiography showed optimal expansion and TIMI 3 flow. The patient remained stable and was discharged without complications.
Case Summary
False lumen–delivered IVL may represent a safe and effective bailout technique for retrieving an entrapped RA burr in heavily calcified coronary lesions, expanding the therapeutic options for complex RA complications.