Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251105_008
A Bendy Road to Success: Complex TAVI in Bicuspid Aortic Stenosis
By Muhammad Hanis Muhmad Hamidi, Stephen O'Connor, Mark Hensey
Presenter
Muhammad Hanis Muhmad Hamidi
Authors
Muhammad Hanis Muhmad Hamidi1, Stephen O'Connor2, Mark Hensey2
Affiliation
Hospital UiTM, Malaysia1, St James's Hospital, Ireland2
View Study Report
CASE20251105_008
Structural - Aortic Valve Intervention - Bicuspid AV
A Bendy Road to Success: Complex TAVI in Bicuspid Aortic Stenosis
Muhammad Hanis Muhmad Hamidi1, Stephen O'Connor2, Mark Hensey2
Hospital UiTM, Malaysia1, St James's Hospital, Ireland2
Clinical Information
Relevant Clinical History and Physical Exam
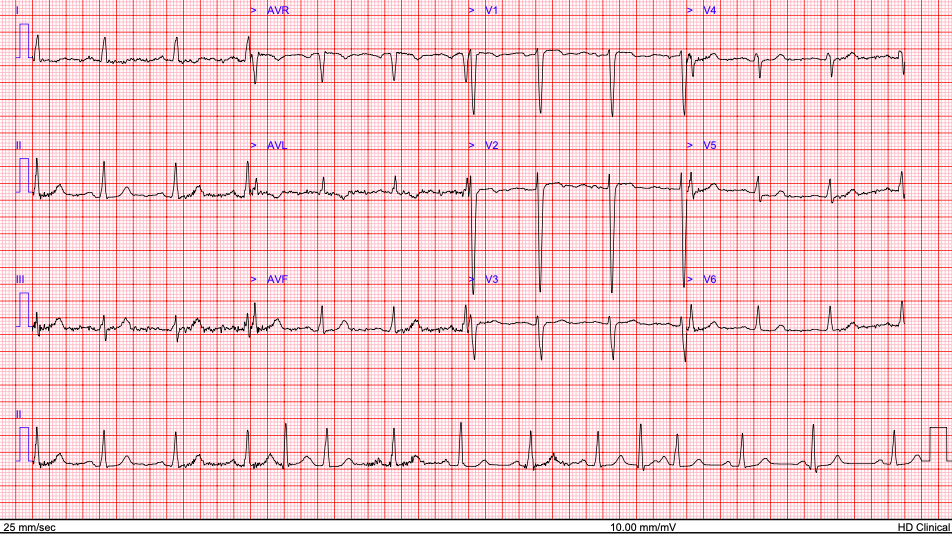
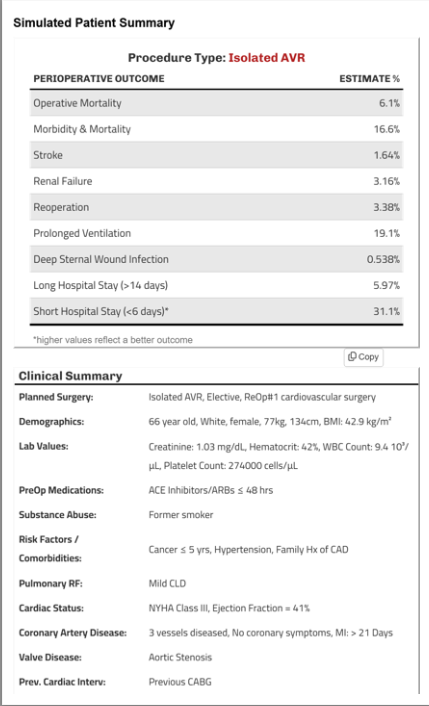
A 66y.o lady complains of progressive exertional dyspnea NYHA III for a year. She has no chest pain or syncope. She has multiple comorbids; history of CABG in 2010 for NSTEMI with LM disease (LIMA-LAD, left radial-diagonal), breast cancer in 2022 and done chemotherapy and mastectomy, severe kyphoscoliosis and chronic back pain. She is obese with short stature with BMI 43 and height 134cm. She is an exsmoker with COPD and OSA. On examination there is systolic murmur at aortic area.
Relevant Test Results Prior to Catheterization
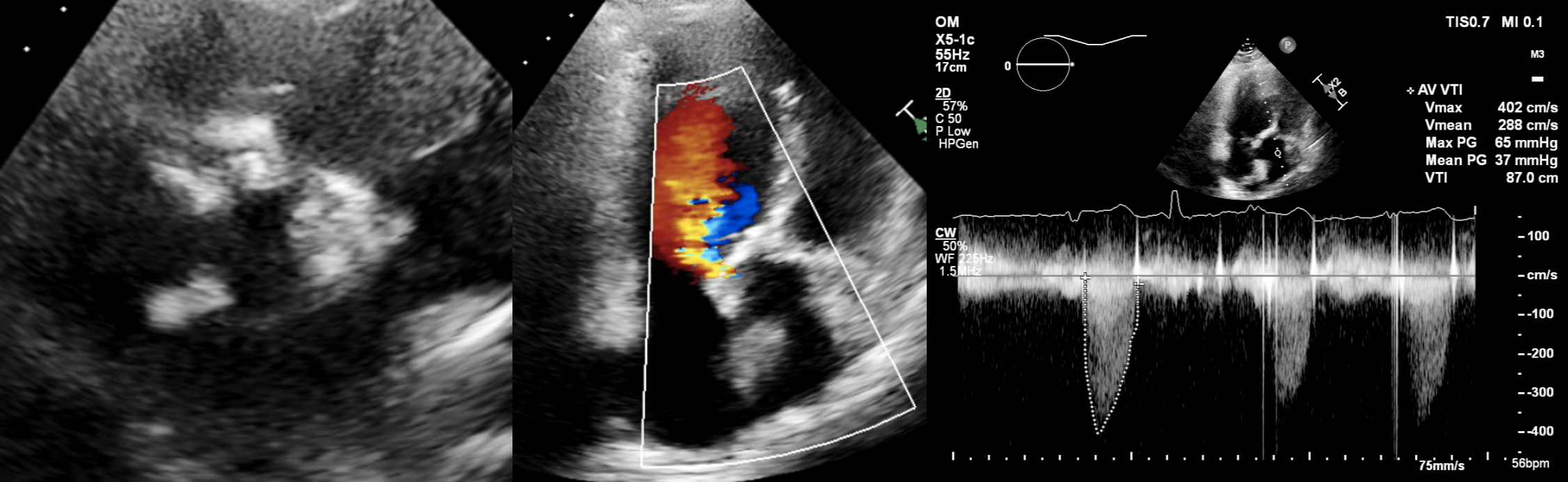
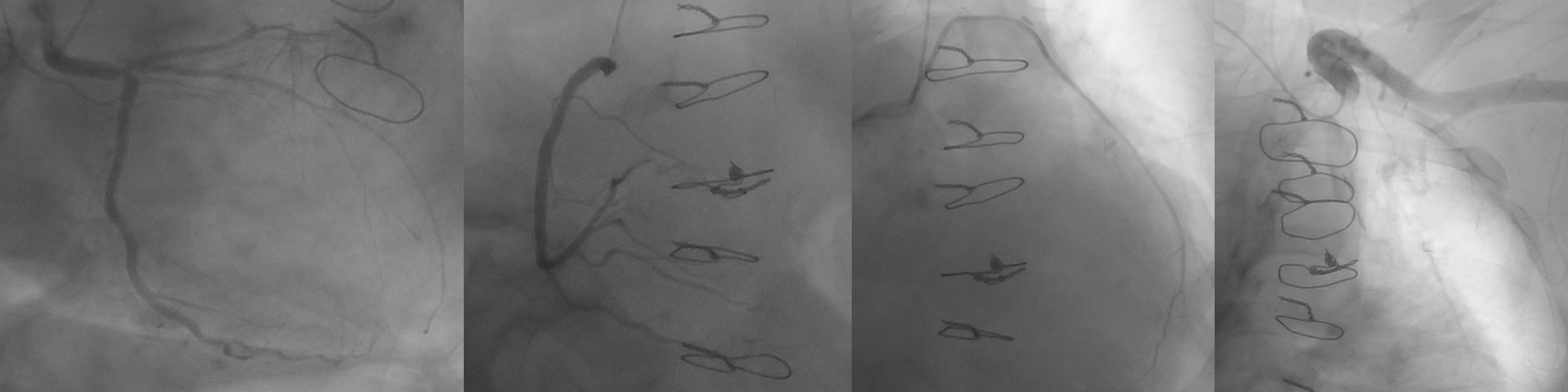
Her echo showed LVEF 41%, severe bicuspid aortic stenosis with fusion RCC/NCC, Mean/Max 37/65mmHg, Vmax4.02m/s, AVA 0.8cm2 with mild to moderate aortic regurgitation. Her coronary angiogram and graft study showed patent LIMA-LAD, radial-diagonal grafts, eccentric distal LM disease extending into ostial LAD and non obstructive LCx and RCA disease.
 TTE short axis 2.mp4
TTE short axis 2.mp4
TTE A5C.mp4
Relevant Catheterization Findings
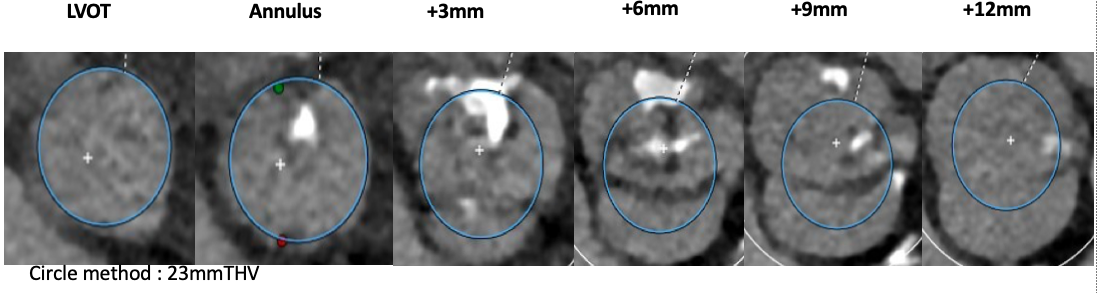
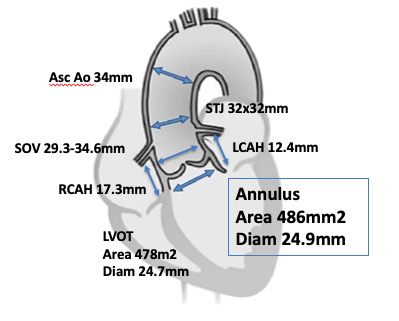
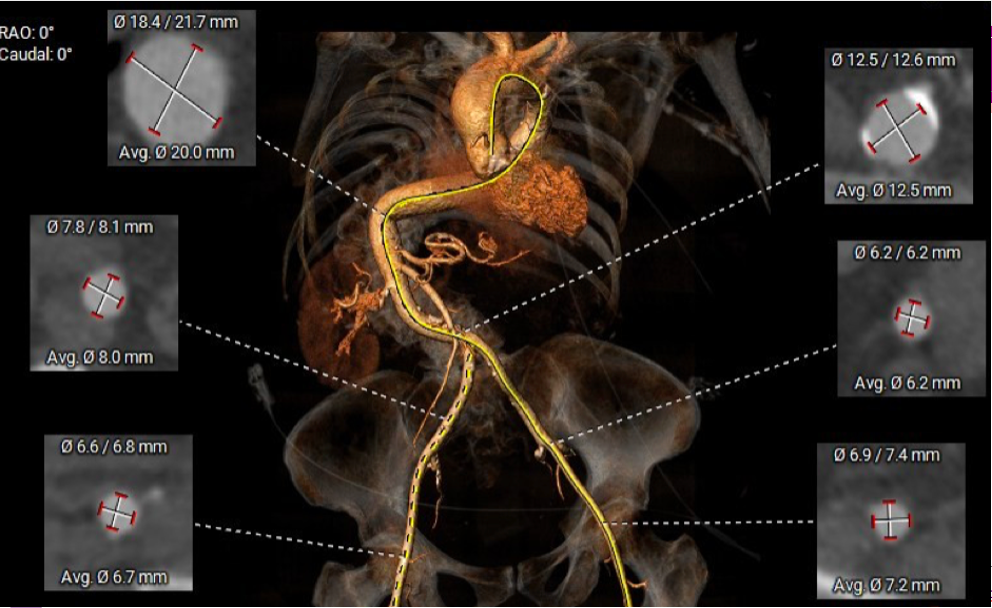
CT-TAVI confirmed Type 1B (RCC-NCC fusion) bicuspid aortic stenosis with severe raphe calcification. Aortic annulus area 486mm2, Area derived diameter 24.9mm. Other CT parameters are as attached. Both iliofemoral arteries diameter and morphology is satisfactory for transfemoral access. However, there is extreme tortuosity of her descending aorta with almost complete S shape but no significant disease or calcification throughout.
HH batch annulus edit.mp4
Aorta.mp4
Interventional Management
Procedural Step
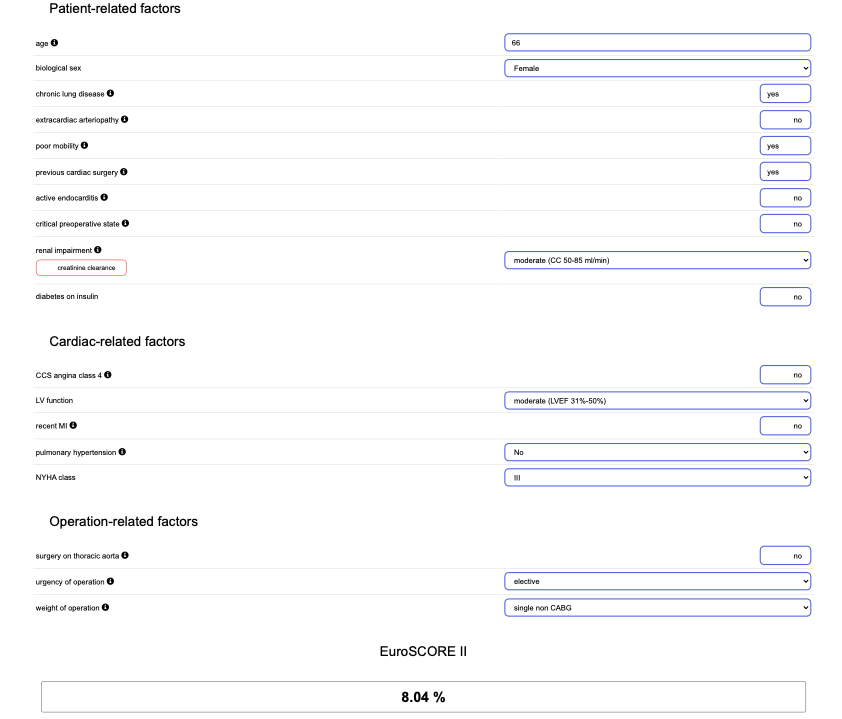
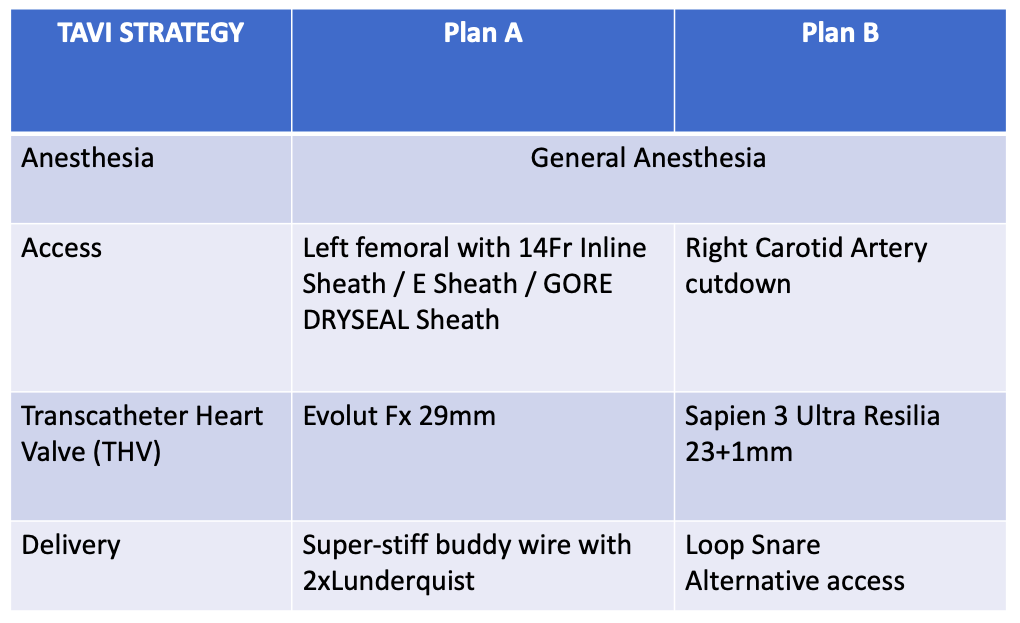
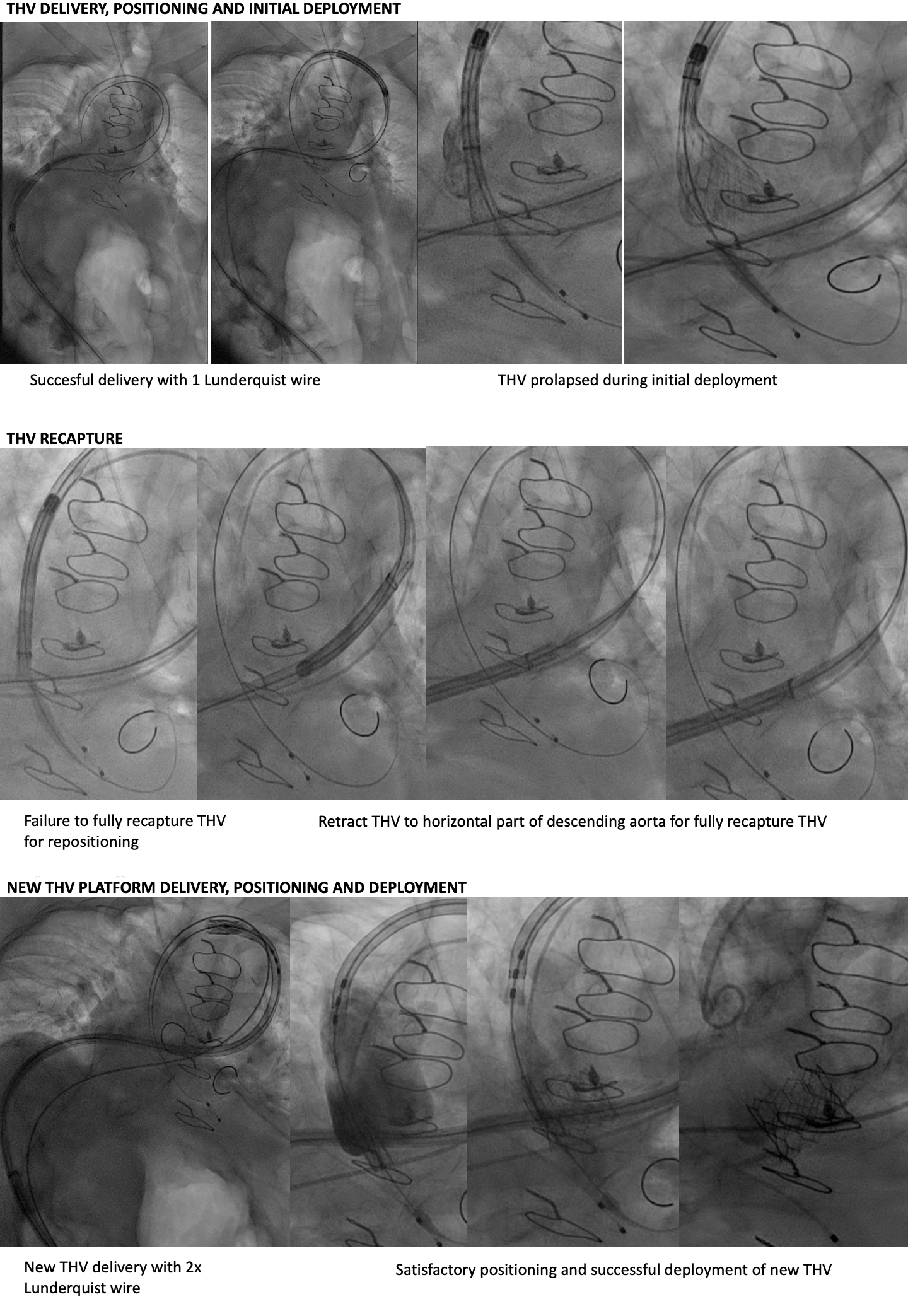
She was turned down for surgical AVR (STS 6.2%, EuroScoreII 8.0%, resternotomy, high BMI, short stature, kyphoscoliosis, COPD and breast cancer history) during Heart Team discussion. For TAVI risk, she is a young lady with almost type 0 bicuspid aortic stenosis and severely calcified raphe, tortuous aorta and left subclavian artery. We had discussed multiple strategy and decided for left transfemoral TAVI using Evolut FX 29mm. After 18mm balloon valve predilation, we successfully delivered THV to aortic root with 1 Lunderquist wire on first attempt. After satisfactory positioning, the THV had prolapsed during initial deployment. We were unable to recapture the THV nose cone tip for repositioning despite multiple maneuvers. We managed to realign the nose cone tip and fully recapture the THV by retracting to straighter part of descending aorta.This time, we had to use 2 Lunderquist wire to redeliver THV across the aortic arch. This maneuver was repeated 3 times as the THV would not remain in place due to the complex calcified nature of bicuspid valve and severe aorta tortuosity. We decided to switch to plan B using a new THV platform - Sapien 3 Ultra Resilia 23mm+1. We exchanged to E-Sheath 14Fr and successfully deliver new THV around the curves using 2 Lunderquist buddy wire. After satisfactory positioning, we successfully deployed the new THV under rapid pacing with excellent angiographic and echocardiographic results. The patient was well and discharged at day 3 post TAVI.
9-Delivery-Evolut.mp4
30 Delivery of ES3.mp4
33 FInal Aortogram.mp4
Case Summary
Super-stiff buddy wire technique is very useful in tackling aortic tortuosity. Extensive complex calcified bicuspid aortic valve with severe aortic tortuosity can significantly impact on certain THV positioning, deployment and recapturability. There is a crucial strategic need to have plan B when pursuing TAVI procedure in patient with complex anatomy.