Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251105_006
My Horrible Nightmare: Dealing With the Latrogenic Coronary Extravasation and Ostium Spiral Dissection
By Zhen Cheng Hwang, Hao-Yun Lo, Chen Lun Su
Presenter
Chen Lun Su
Authors
Zhen Cheng Hwang1, Hao-Yun Lo1, Chen Lun Su1
Affiliation
Division of Cardiology, Department of Internal Medicine, Shin Kong Wu Ho-Su Memorial Hospital, Taipe, Taiwan1
View Study Report
CASE20251105_006
Coronary - Complication Management
My Horrible Nightmare: Dealing With the Latrogenic Coronary Extravasation and Ostium Spiral Dissection
Zhen Cheng Hwang1, Hao-Yun Lo1, Chen Lun Su1
Division of Cardiology, Department of Internal Medicine, Shin Kong Wu Ho-Su Memorial Hospital, Taipe, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
This is a 60-year-old woman referred from Palau to Taiwan’s hospital because of chest pain for months despite several medical treatment. She was a heavy smoker, smoking 0.5 pack per day for almost 40years. Past history of hypertension, hyperlipidemia and obesity with BMI 29. Her family had abundant CAD disease included father & brother with CABG history, sister with PCI history. Due to the unstable angina, she was sent to Shin Kong hospital for PCI.
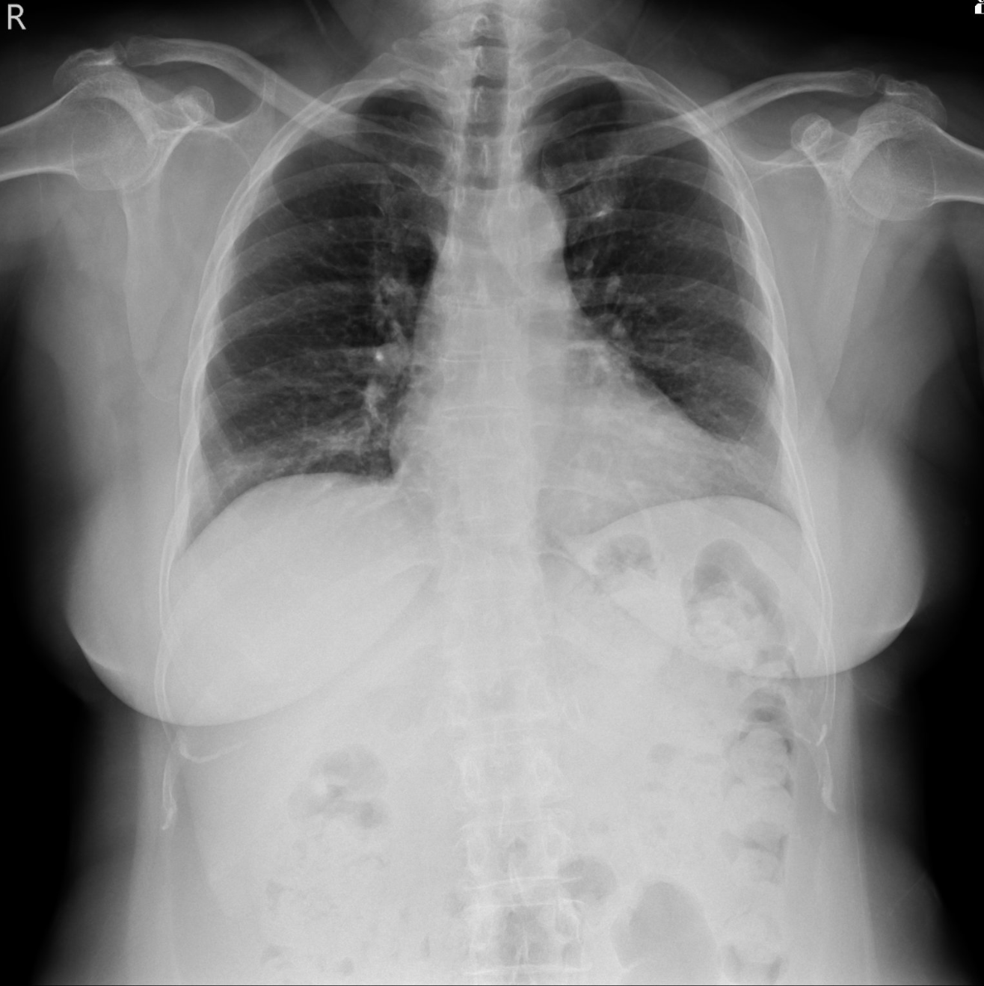
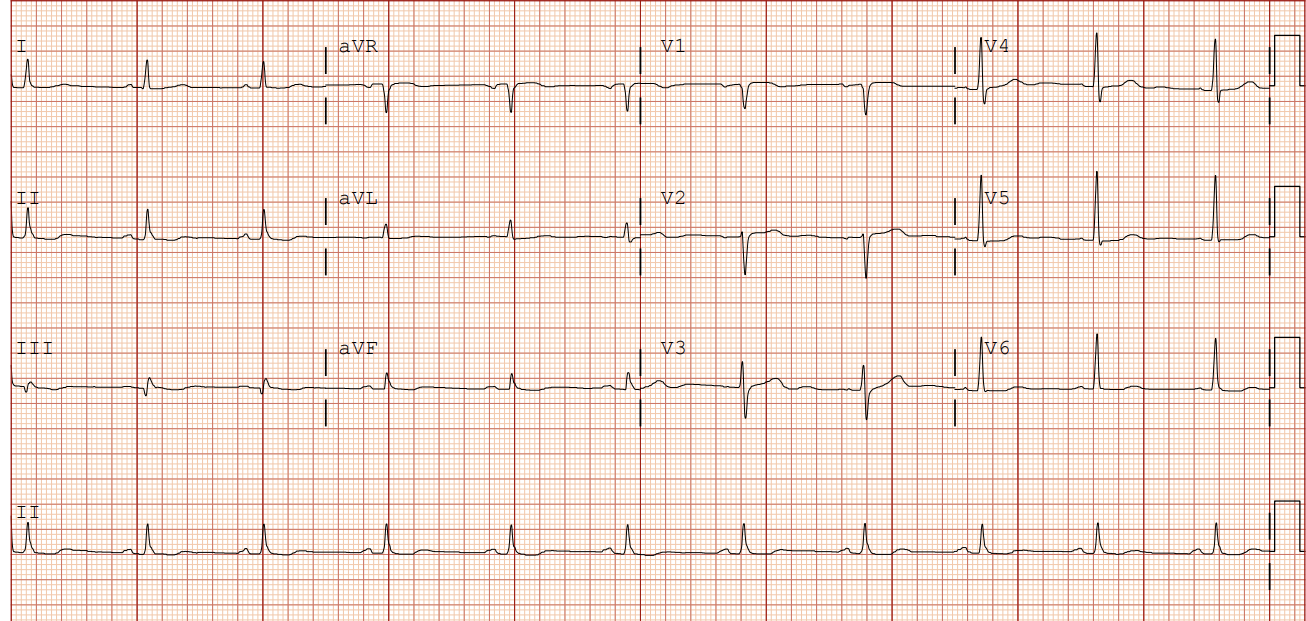
Relevant Test Results Prior to Catheterization
Normal CXR.Normal sinus rhythm, without ST-T changes in EKG
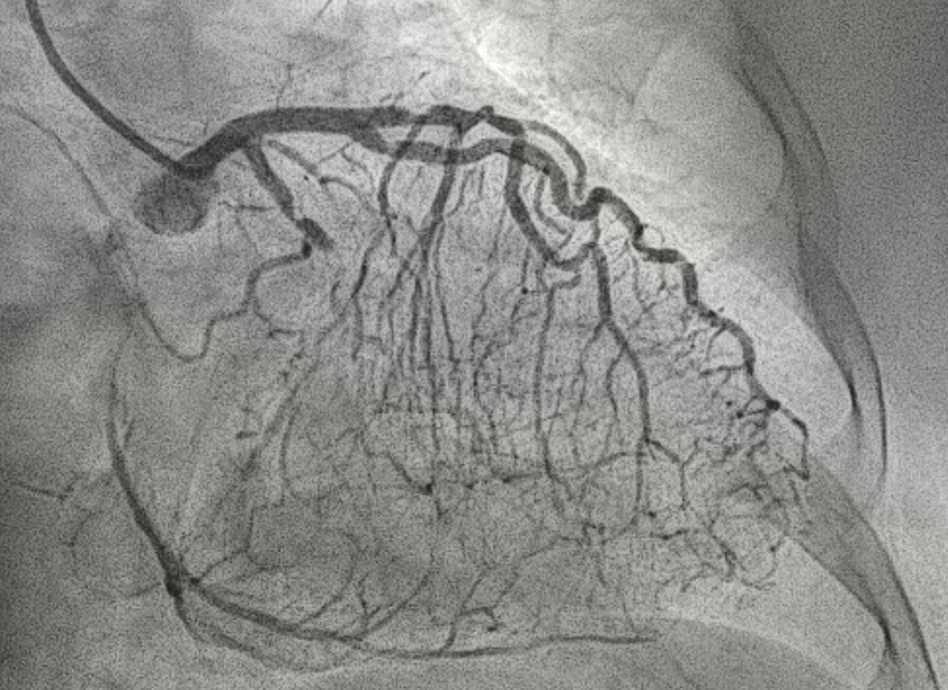
Relevant Catheterization Findings
LM : patent
LAD: middle part 80% stenosis, sending collateral vessels to PDA and LCX
LCX: proximal part 90% stenosis, distal nearly total occlusion
RCA: proximal part 70% stenosis, middle nearly total occlusion
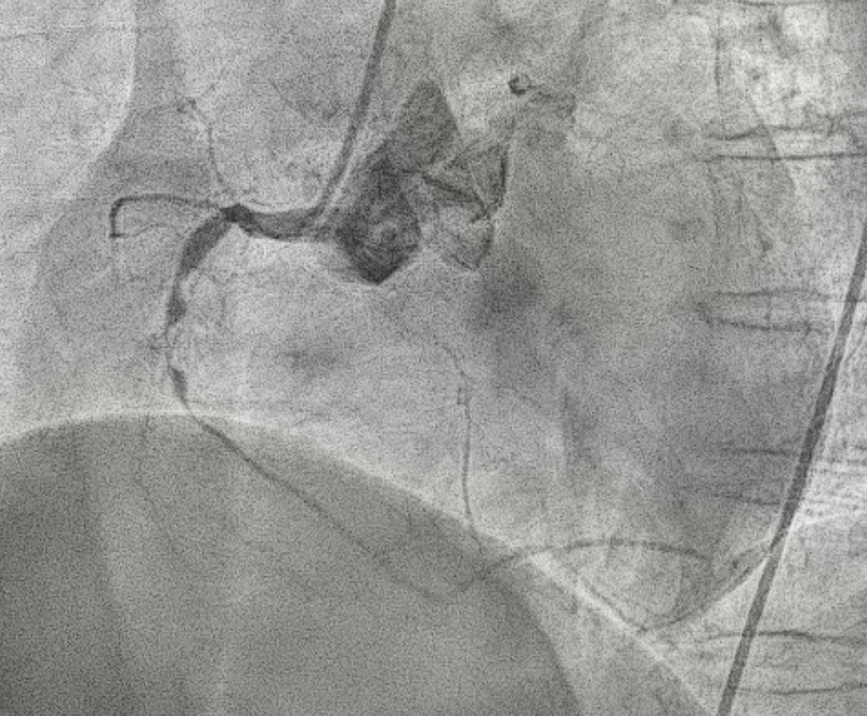

Interventional Management
Procedural Step
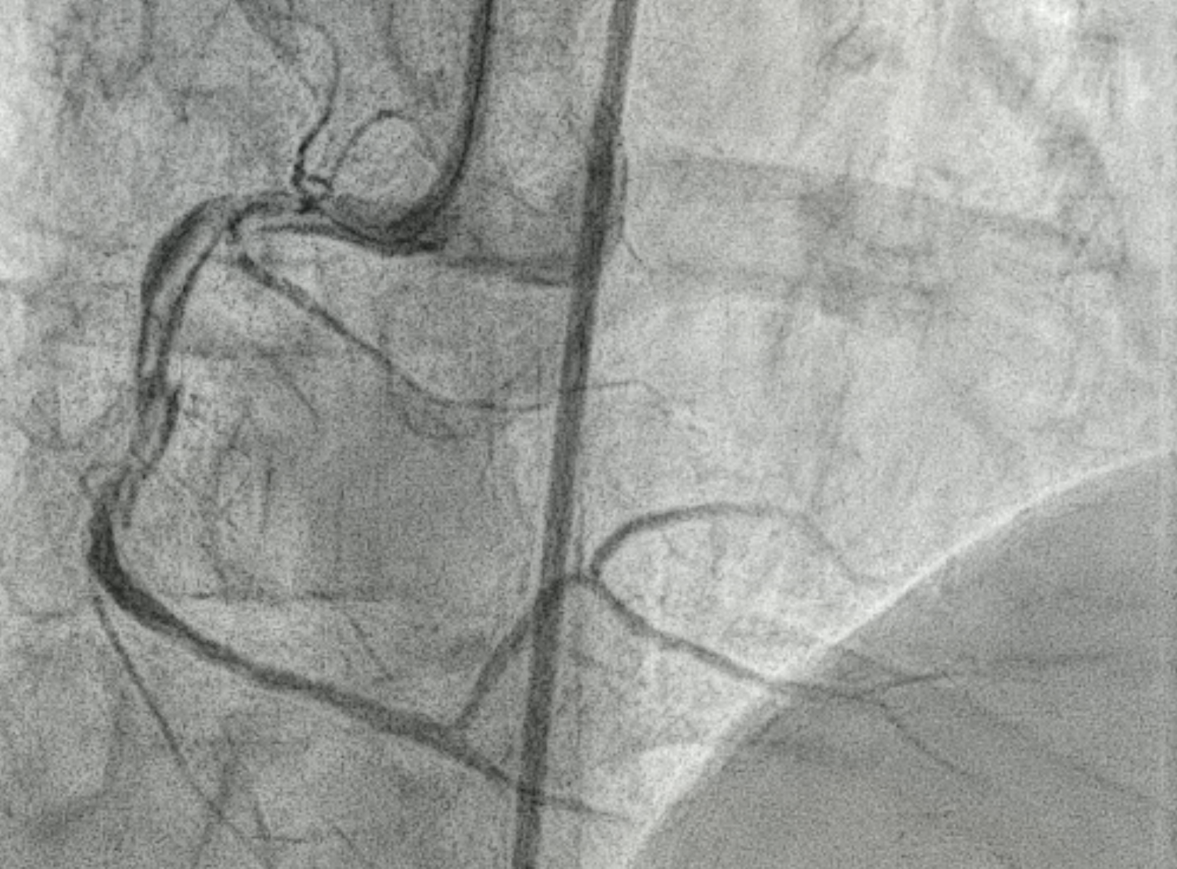
After explaining to the patient, she refused CABG and decided for PCI. 6F SAL1 as guiding catheter, starting intervention from RCA. Pressure damping was noted after engagement. While wiring Fielder FC to RCA, extravasation occurred followed by hypotension, bradycardia and nausea.IV saline challenge, inotropics agent were prescribed to stablelize the patient. Echogram showed no tamponade.
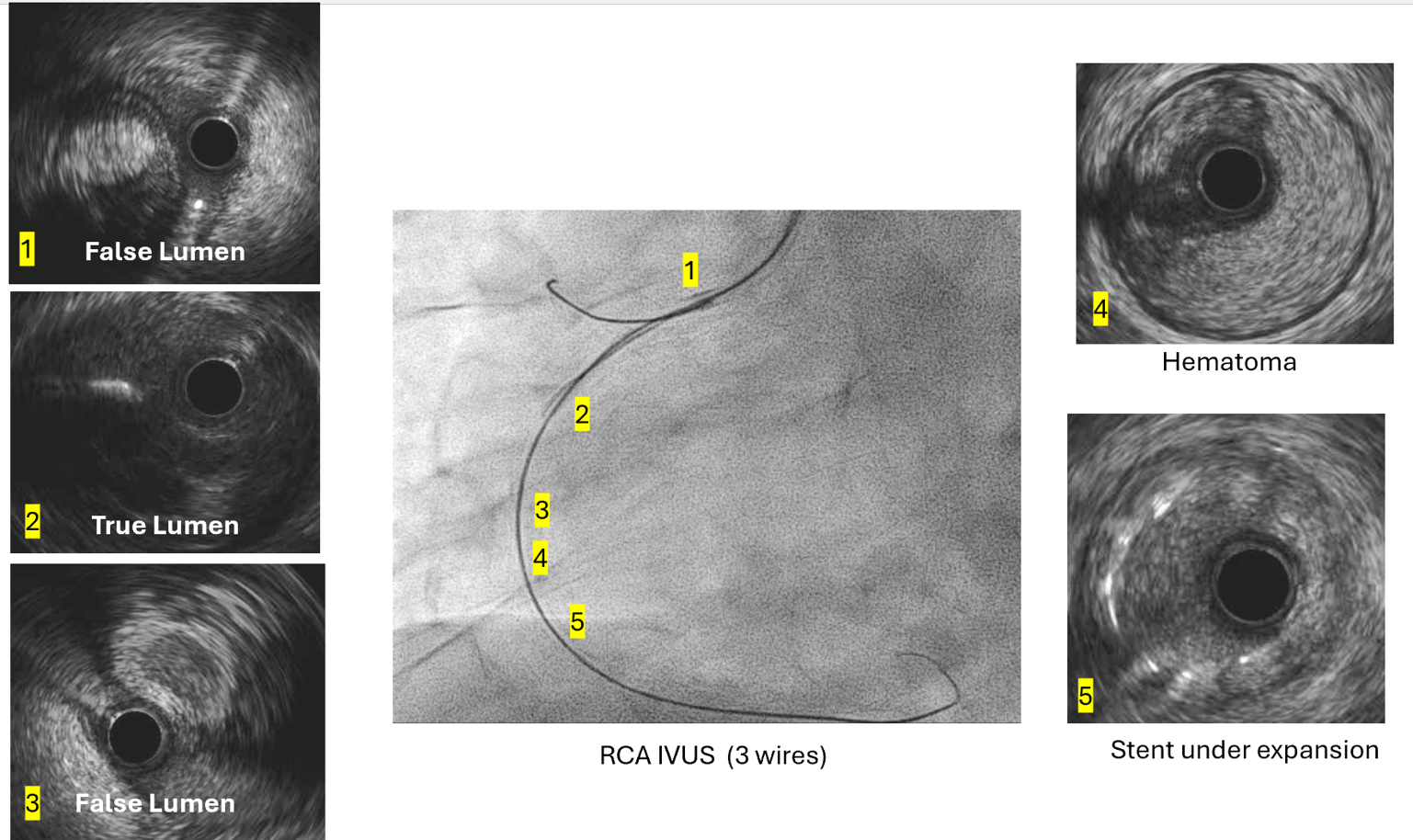
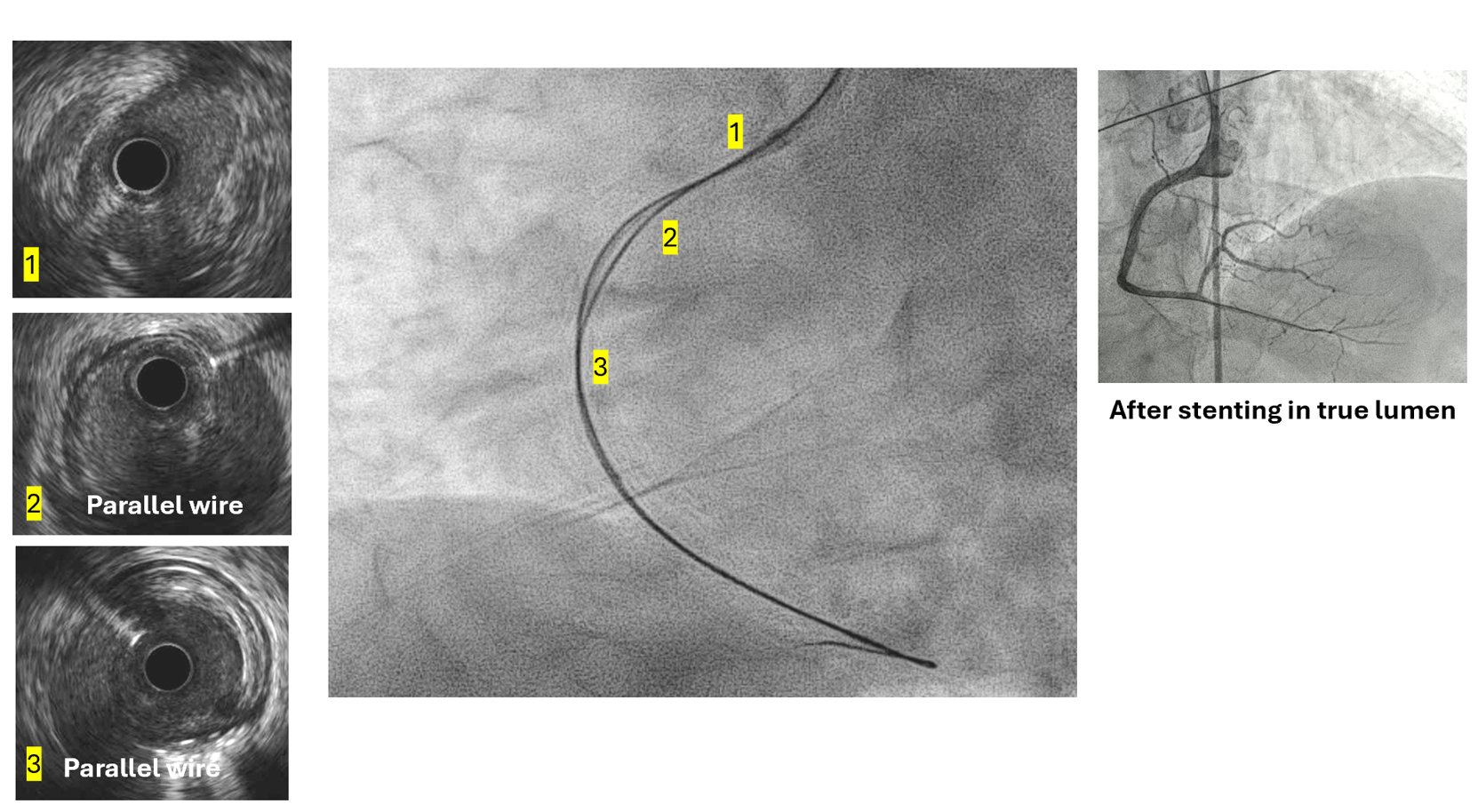
The SAL1 guiding catheter was unstable, jumping in and out the ostium. We deployed PK Papyrus 2.5 x 20 mm stent graft to dRCA quickly and planned to deployed another DES to p-dRCA. However, the patient agitated and the whole system was removed, leaving severe spiral dissection, starting from the ostium to middle RCA.We tried to wire FC, XTA and sion balck to true lumen but fail. Switched to 6F JR guiding but still fail.We wired FC to distal RCA with parallel wire technique and checked IVUS. The distal wire was over true lumen, but false lumen wiring was noted since proximal RCA.We wired XTA to true lumen under IVUS image. Then true lumen wiring was completed.We dilated with 1.5 balloon. Followed by Ryurei 2.50 x 15 mm to mRCA.We deployed Ultimaster Tansei 3.00 x 38 mm and Ultimaster Tansei 4.00 x 18 mm to p-dRCA.Post-dilated with 3.0, 3.5, and 4.0 NC balloon to RCA.The final IVUS showed well stent expansion.The final flow is good. We closed the procedure smoothly.
 24218894_007 fielderFC wiring but extravasation.AVI
24218894_007 fielderFC wiring but extravasation.AVI
24218894_116 pRCA stenting position.AVI
24218894_134 floating wire.AVI
The SAL1 guiding catheter was unstable, jumping in and out the ostium. We deployed PK Papyrus 2.5 x 20 mm stent graft to dRCA quickly and planned to deployed another DES to p-dRCA. However, the patient agitated and the whole system was removed, leaving severe spiral dissection, starting from the ostium to middle RCA.We tried to wire FC, XTA and sion balck to true lumen but fail. Switched to 6F JR guiding but still fail.We wired FC to distal RCA with parallel wire technique and checked IVUS. The distal wire was over true lumen, but false lumen wiring was noted since proximal RCA.We wired XTA to true lumen under IVUS image. Then true lumen wiring was completed.We dilated with 1.5 balloon. Followed by Ryurei 2.50 x 15 mm to mRCA.We deployed Ultimaster Tansei 3.00 x 38 mm and Ultimaster Tansei 4.00 x 18 mm to p-dRCA.Post-dilated with 3.0, 3.5, and 4.0 NC balloon to RCA.The final IVUS showed well stent expansion.The final flow is good. We closed the procedure smoothly.
Case Summary
This is a PCI case with iatrogenic coronary extravasation and dissection. The nightmare started at the beginning of the intervention with poorly preparation and uncooperative patient. We tried several attempts including parallel wire technique and IVUS guided wiring to ensure the wire was located in the true lumen. We shared this case to inform that fully preparation, planning & discussion should not be neglected including catheter option, wire selection, PCI strategies/CABG risk & benefit and the necessary of mechanical support before the intervention. Thanks!