Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251105_005
Challenges in Retrograde CTO PCI: Addressing Left Ventricular Billowing and Device Entanglement
By Ricky Wang Hei Leung, Frankie Chor-cheung Tam
Presenter
Ricky Wang Hei Leung
Authors
Ricky Wang Hei Leung1, Frankie Chor-cheung Tam1
Affiliation
Queen Mary Hospital, Hong Kong, China1
View Study Report
CASE20251105_005
Coronary - Complex PCI - CTO
Challenges in Retrograde CTO PCI: Addressing Left Ventricular Billowing and Device Entanglement
Ricky Wang Hei Leung1, Frankie Chor-cheung Tam1
Queen Mary Hospital, Hong Kong, China1
Clinical Information
Relevant Clinical History and Physical Exam
A 71-year-old male smoker with a history of ACS underwent PCI to the LAD and LCX nearly 20 years ago. He presented with recurrent chest discomfort. CTCA revealed an occluded proximal RCA, in-stent restenosis (ISR) in the LAD, and a patent LCX stent. Coronary angiography confirmed LAD Type 4 ISR and ostial RCA CTO with collateral supply. PCI to the LAD ISR was successfully performed, and staged PCI to the RCA CTO was planned. Physical examination was unremarkable.
 MOVIE-0073.mp4
MOVIE-0073.mp4
MOVIE-0005.mp4
MOVIE-0011.mp4
Relevant Test Results Prior to Catheterization
Review of the index procedure angiogram was essential before the staged RCA CTO PCI, which is described at section below.
Relevant Catheterization Findings
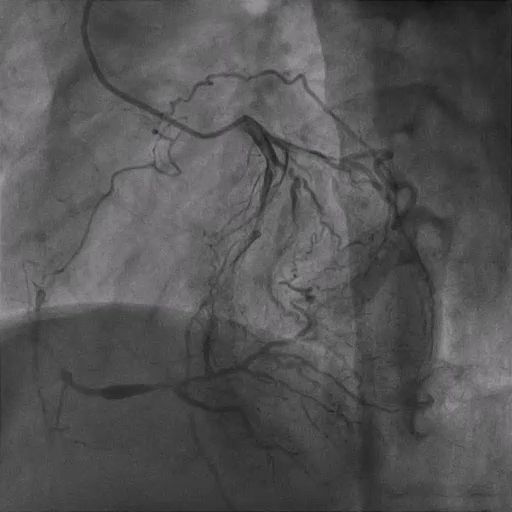
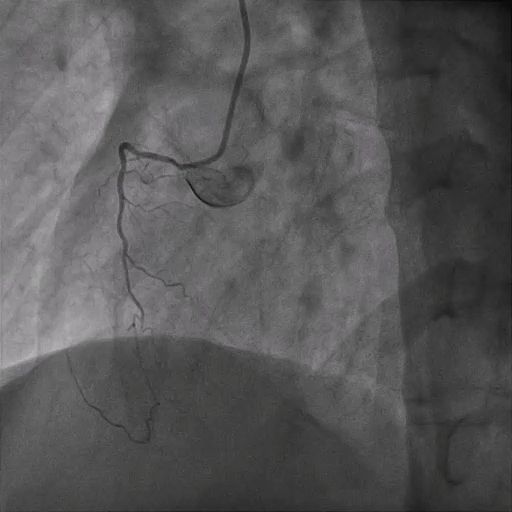
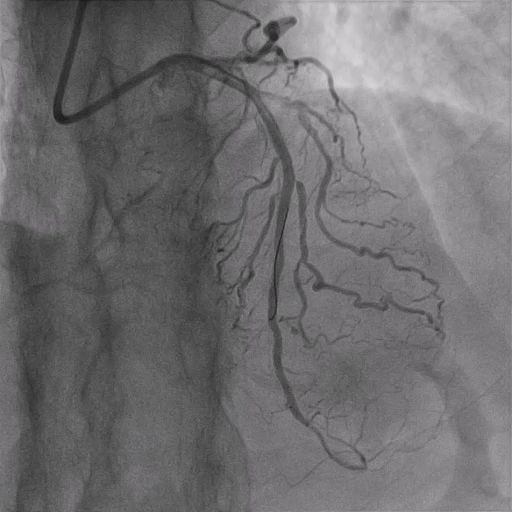
The RCA CTO had an ambiguous proximal course with a non-tapered stump and an estimated occlusion length of ≈50 mm. Distal vessel quality was good, with collateral filling mainly from the LCX, providing critical information for procedural planning and strategy selection.

MOVIE-0006.mp4
MOVIE-0009.mp4
Interventional Management
Procedural Step
Bilateral 6Fr femoral access was obtained for staged PCI to the RCA CTO. The antegrade approach using a Gaia Next 2 wire entered the mid-RCA, but ADR with a Recross microcatheter and CP12 wire failed. A retrograde approach via the PL branch was then attempted using a SUOH3 wire, with reverse CART performed using a 2.5-mm balloon and CP12 wire. The Caravel microcatheter could not cross the CTO due to lesion rigidity, and the antegrade system was lost. The retrograde system was re-established with a Turnpike 150 microcatheter, which successfully traversed the lesion and was externalized using an RG3 wire snared into the antegrade JR4 guide. During retrograde microcatheter withdrawal, the patient developed severe chest pain and hypotension (due to stretching of LV i.e., billowing), requiring stabilization with intravenous adrenaline and dopamine. After the antegrade microcatheter crossed the lesion, the retrograde system was withdrawn. The RCA was predilated with 2.0- and 2.5-mm balloons, then stented with overlapping 3.0/44-mm and 3.5/44-mm stents, followed by postdilation with NC 3.5- and 4.0-mm balloons. During the final IVUS run, the IVUS catheter became trapped at the proximal RCA stent; it was retrieved by cutting the catheter, inserting a V18 wire into its lumen, and withdrawing it through a 6Fr guide extension. Final angiography demonstrated well-expanded stents with TIMI 3 flow in the RCA.
MOVIE-0090.mp4
MOVIE-0093.mp4
Case Summary
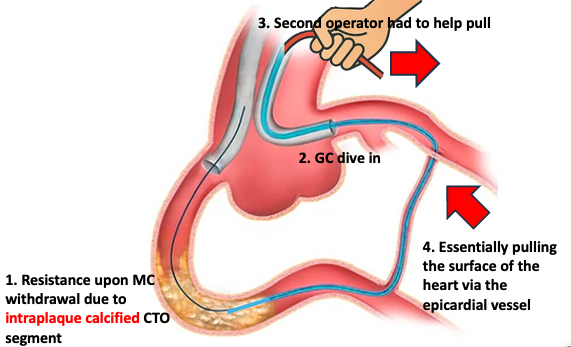
Retrograde PCI to CTO carries risks specific to retrograde approach. LV "billowing" can occur on withdrawal of retrograde MC, especially in this case, due to intra-plaque calcified CTO path and pulling force to antegrade GC by second operator, resulting in a lifting force via the epicardial collaterals. This highlights the importance of understanding risk factor specific to each case and communication between operators. Moreover, trapped IVUS is unusual but important to know how to tackle in a 6F system.