Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251105_001
An NSTEMI Case: RCA With Spontaneous Dissection
By Chan-Hsu Wu, Yen-Lien Chou
Presenter
Chan-Hsu Wu
Authors
Chan-Hsu Wu1, Yen-Lien Chou1
Affiliation
Division of Cardiology, Department of Internal Medicine, Tri-Service General Hospital, National Defe, Taiwan1
View Study Report
CASE20251105_001
Coronary - ACS/AMI
An NSTEMI Case: RCA With Spontaneous Dissection
Chan-Hsu Wu1, Yen-Lien Chou1
Division of Cardiology, Department of Internal Medicine, Tri-Service General Hospital, National Defe, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
A 57-year-old male with a history of hypertension and type 2 diabetes mellitus presented with exertional chest tightness for two days. There was no history of previous myocardial infarction, revascularization, or chest trauma. On arrival, he appeared mildly diaphoretic but alert and oriented. His blood pressure was 105/66 mmHg, heart rate 82 beats per minute, and oxygen saturation 97% under room air. Cardiovascular examination revealed a regular rhythm without murmurs, rubs, or gallops.
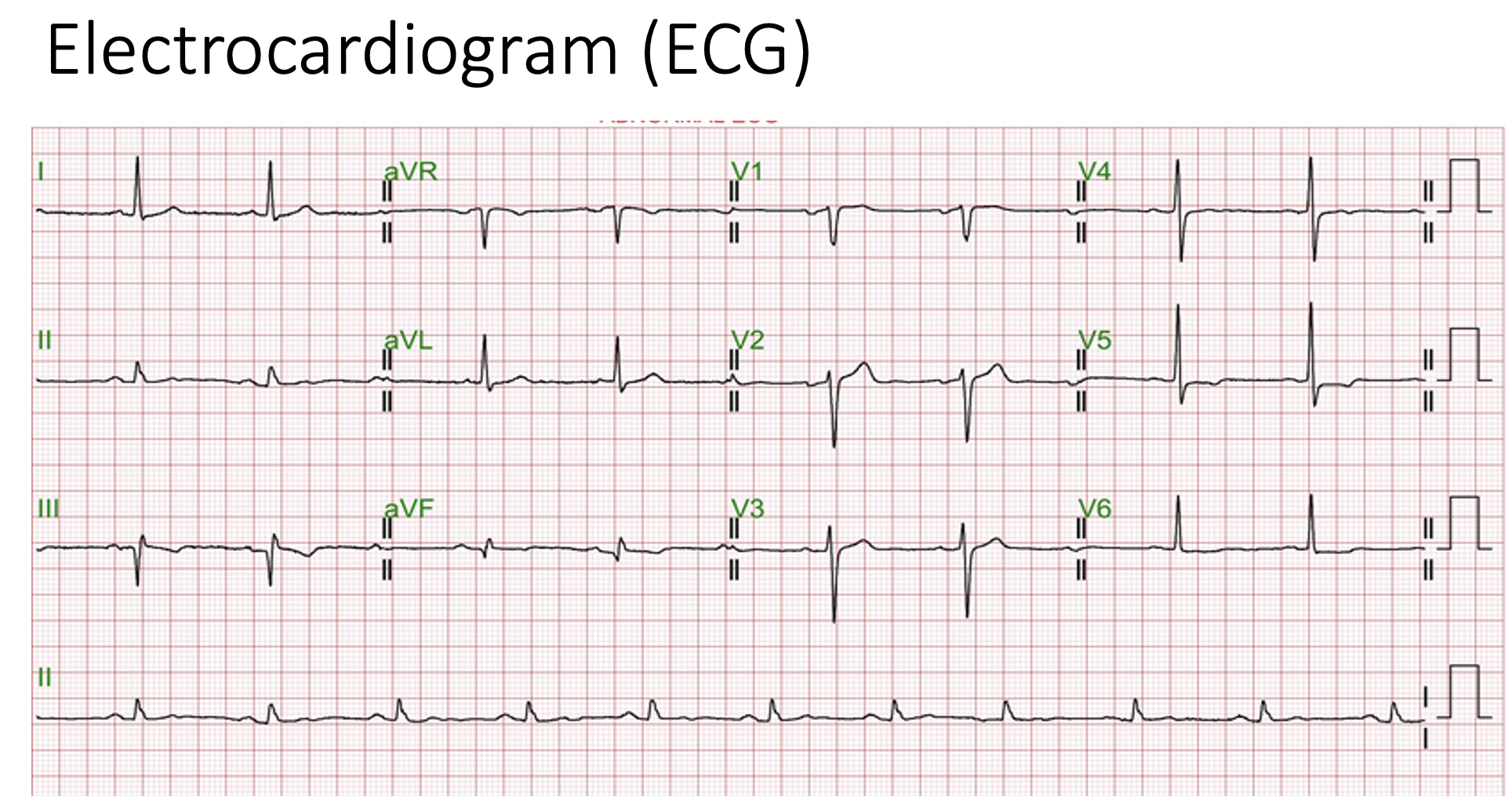
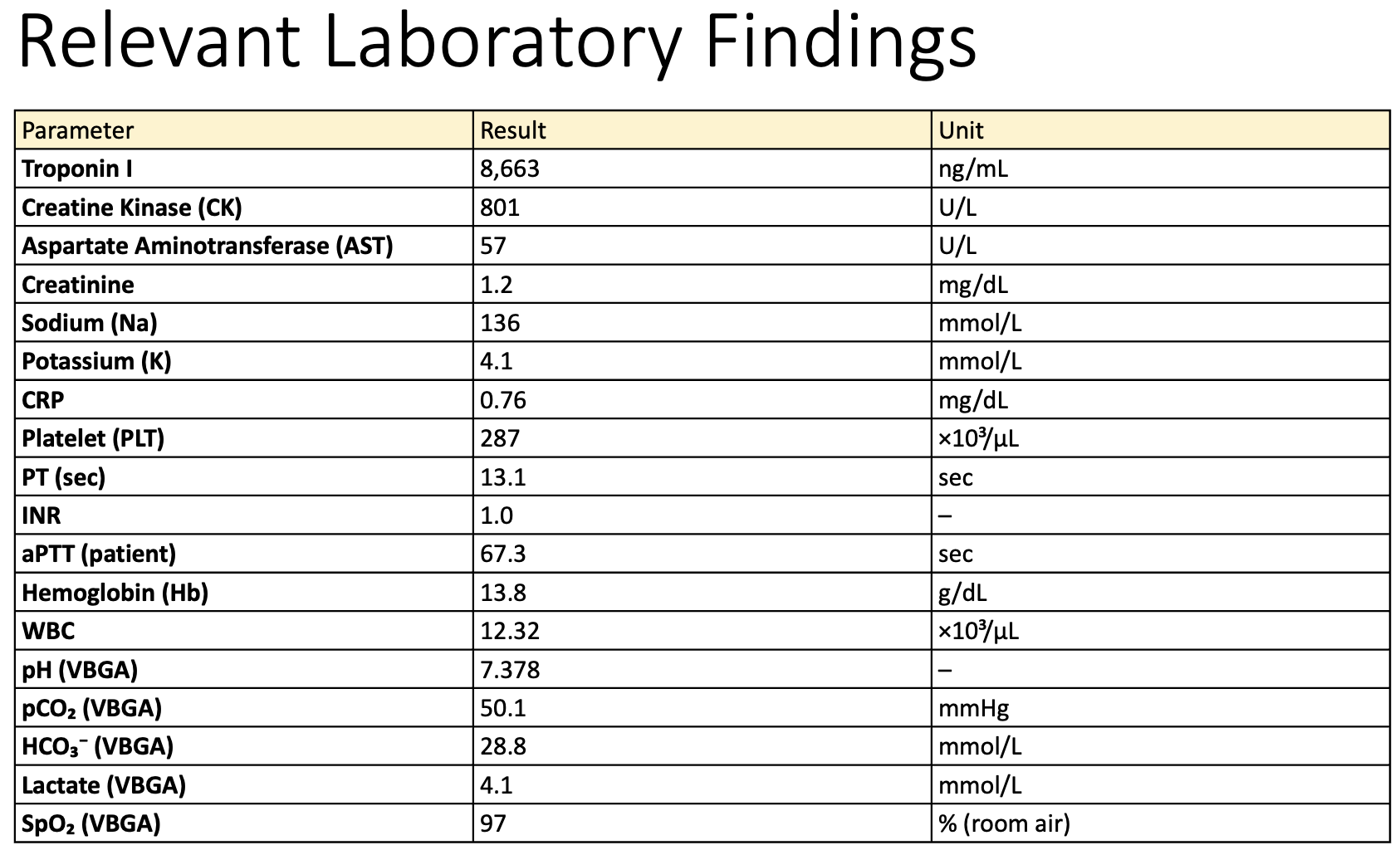
Relevant Test Results Prior to Catheterization
Laboratory testing showed markedly elevated cardiac troponin I (8,663 ng/mL), consistent with acute myocardial injury. The overall findings suggested an acute coronary syndrome, specifically non-ST-elevation myocardial infarction (NSTEMI), prompting further diagnostic evaluation with coronary angiography.
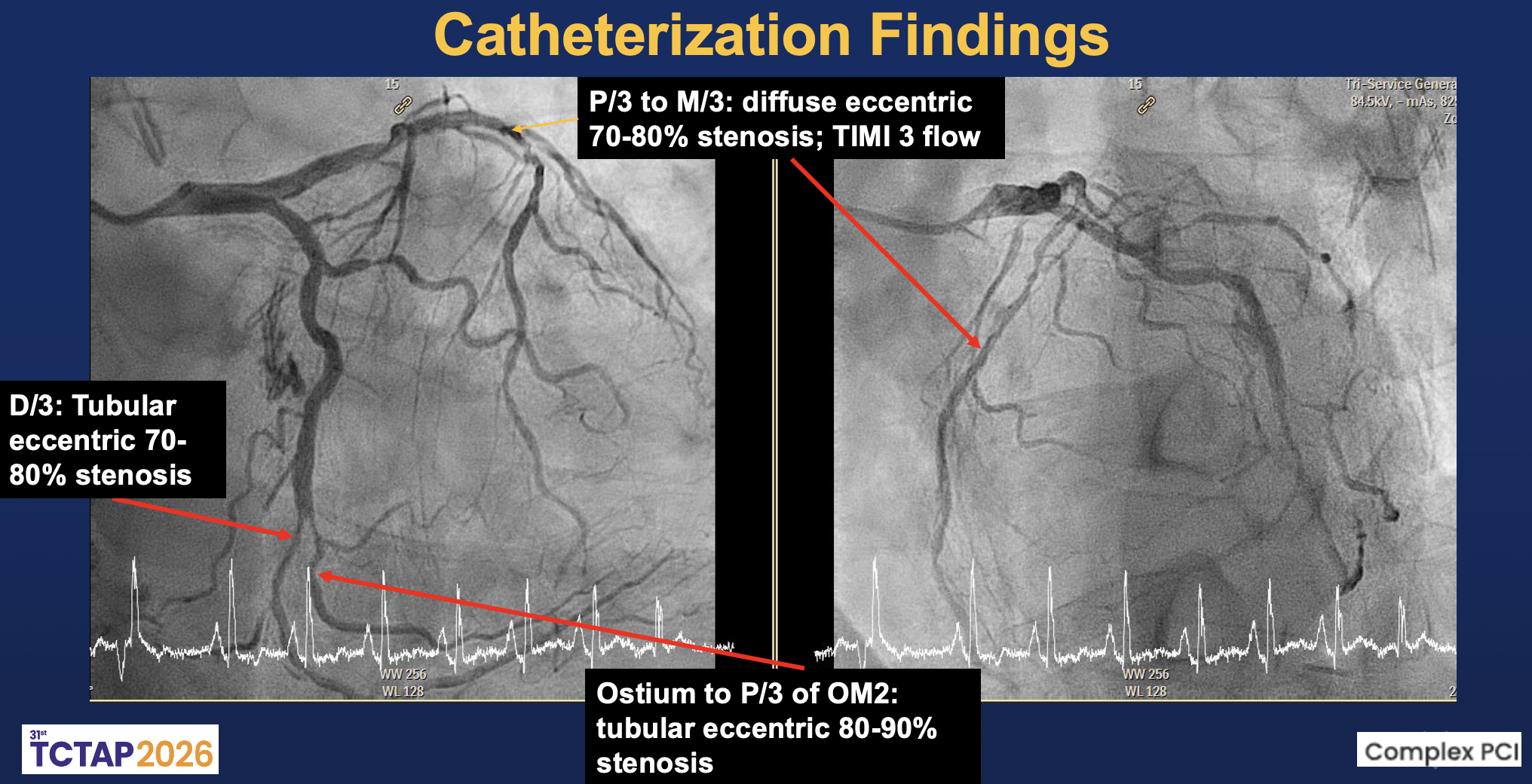
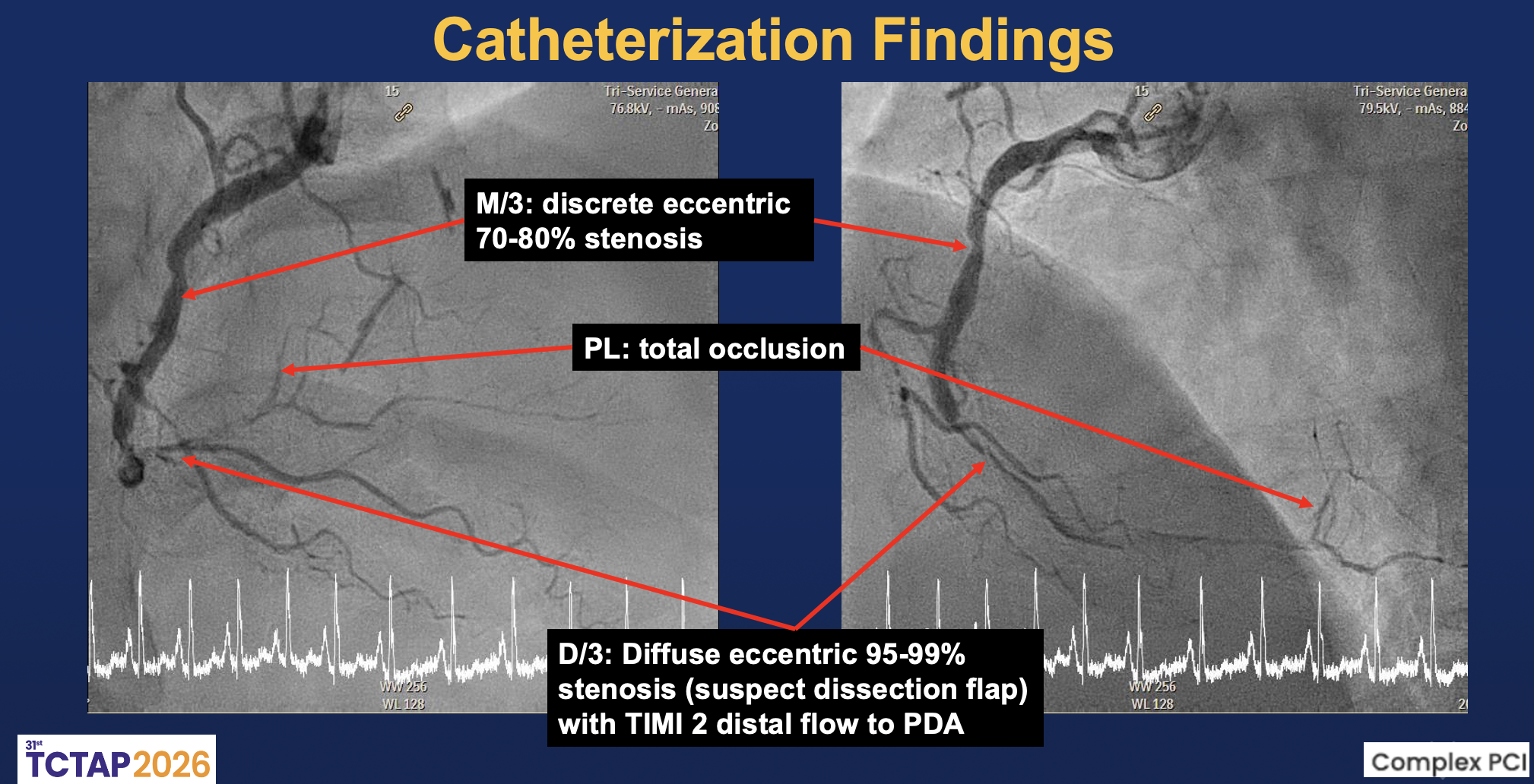
Relevant Catheterization Findings
The left main was patent. The LAD showed diffuse eccentric 70–90% stenosis from proximal to distal segments with preserved TIMI 3 flow. The LCx had distal 80–90% and OM2 ostial-proximal 70–80% stenoses with small caliber, giving collaterals to PL. The RCA was dominant with mid 70–80% stenosis and distal diffuse 95–99% stenosis, suggesting a dissection flap with TIMI II distal flow; the PL branch was totally occluded.
 RAO CAU Left.mp4
RAO CAU Left.mp4
RAO CRA Left.mp4
RCA.mp4
Interventional Management
Procedural Step
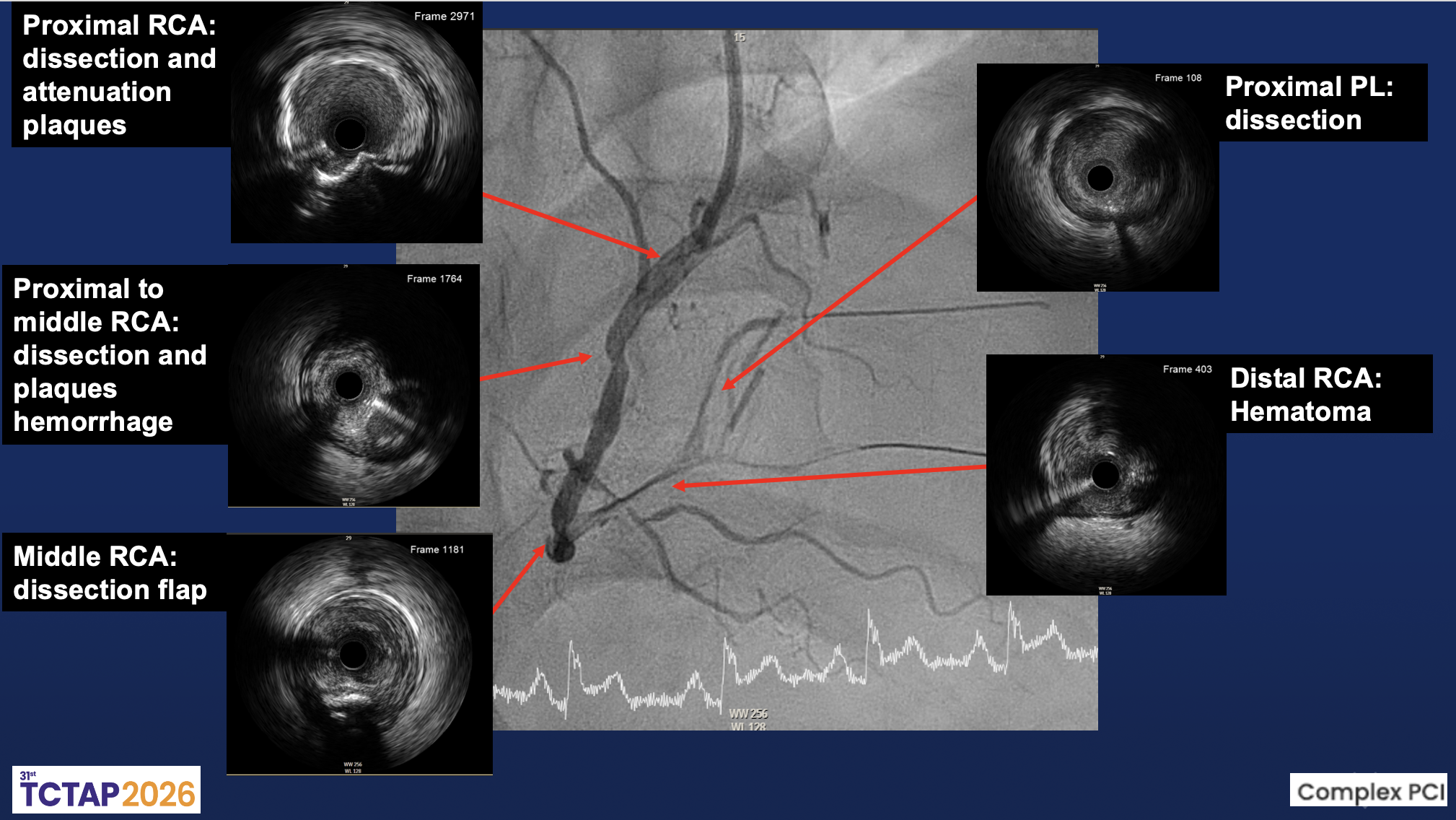
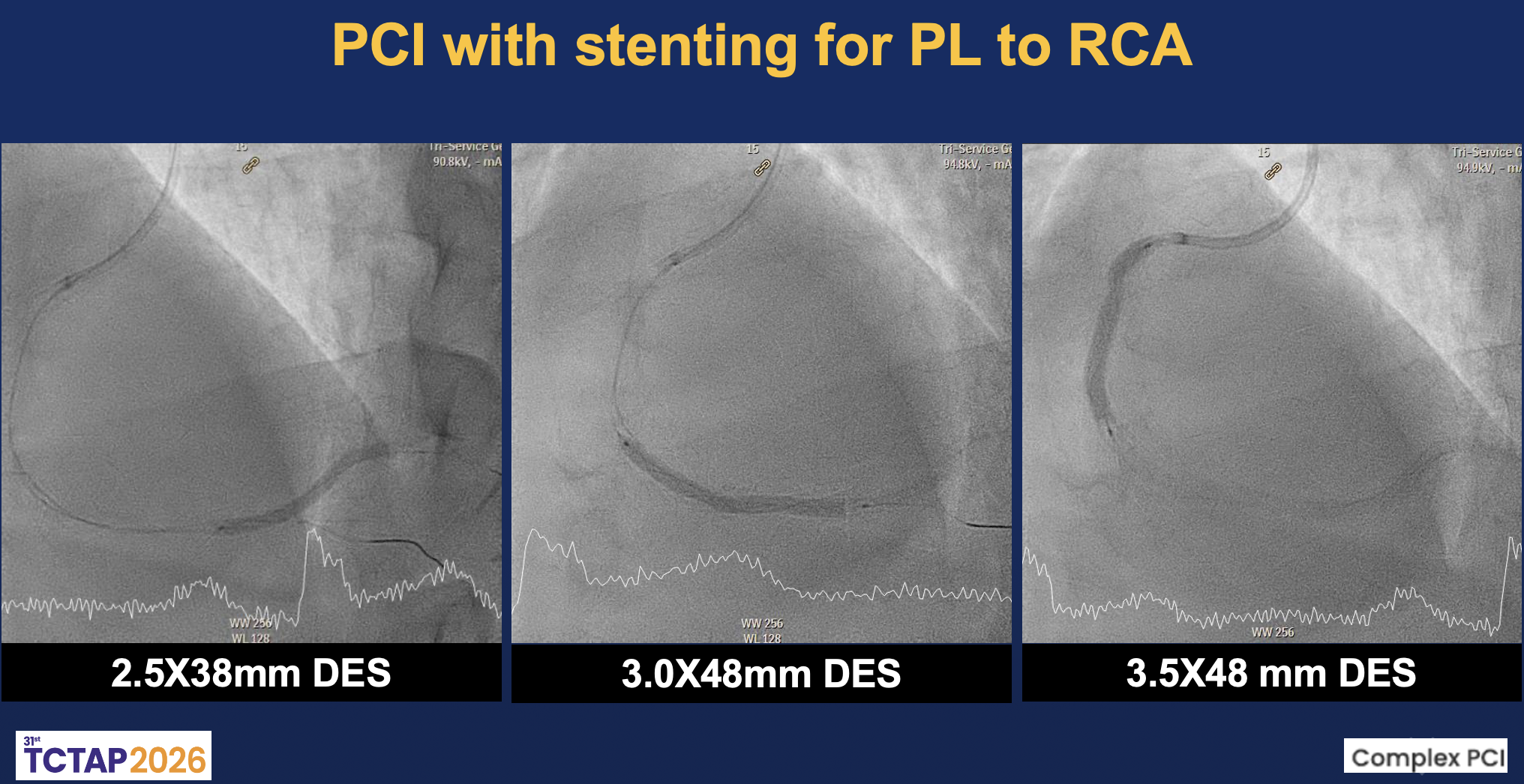
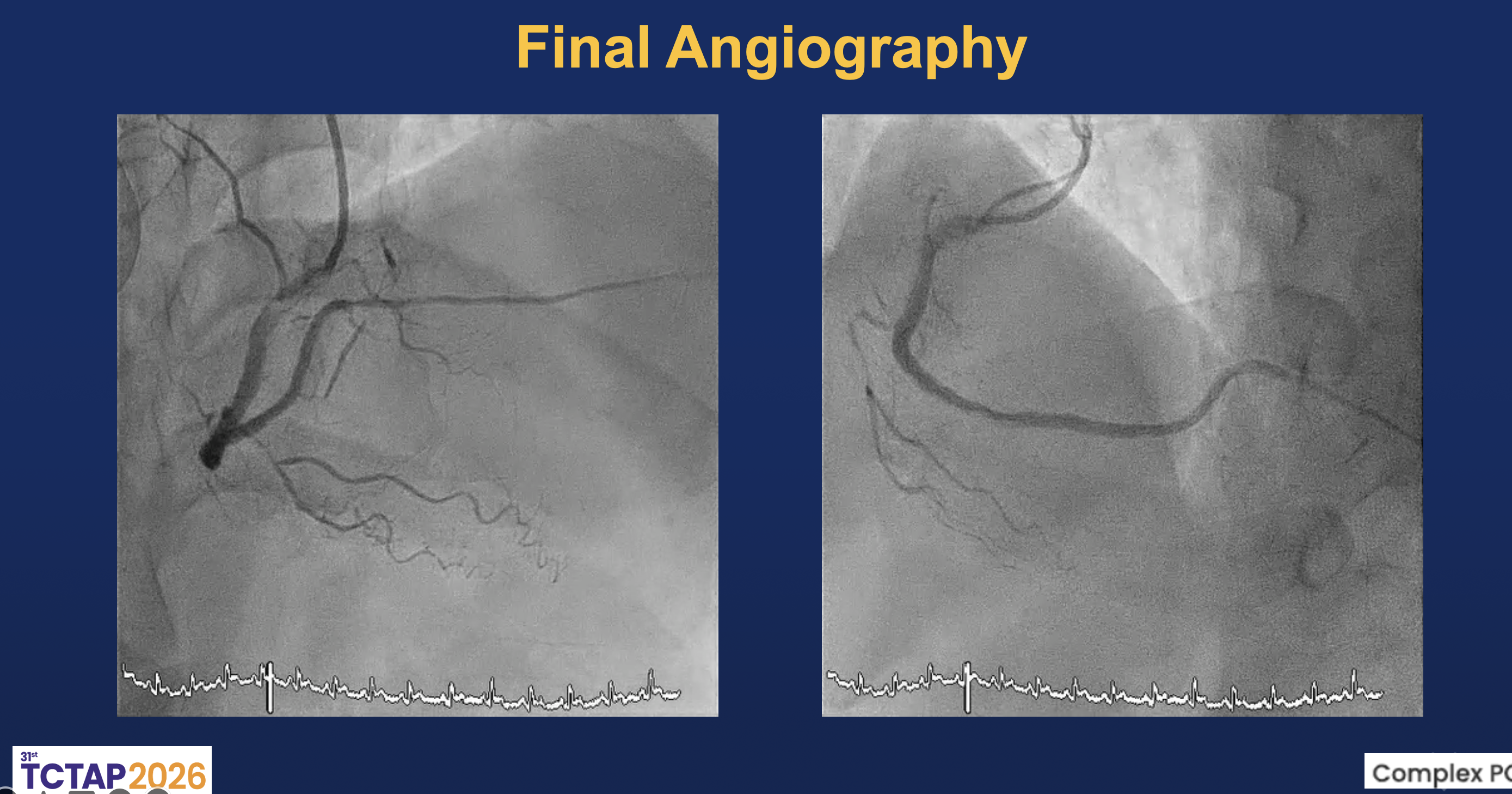
Coronary intervention was performed via the right distal radial approach using a 6F SAL 1.0 guiding catheter. The RCA was identified as the culprit vessel. A Sion Black wire successfully crossed the distal RCA lesion into the posterolateral (PL) branch, followed by predilation with a 2.0×20 mm Ryurei balloon. IVUS imaging revealed multiple intramural abnormalities, including diffuse dissection planes, intramural hematoma, and plaque hemorrhage extending from the proximal to distal RCA. The minimal lumen area (MLA) measured 2.26 mm² at the distal RCA and 3.59 mm² at the PL branch, confirming severe luminal compromise with large plaque burden.Further dilation with a 2.5×15 mm Accuforce balloon induced a type B dissection from distal to mid RCA. Sequential stent implantation was performed with a 2.5×38 mm Onyx stent from PL to distal RCA, a 3.0×48 mm Synergy stent in distal RCA, and a 3.5×48 mm X-X stent from mid to distal RCA. Post-dilatation using 3.0×20 mm and 4.0×15 mm Accuforce balloons optimized stent expansion. Repeat IVUS demonstrated good apposition with resolution of intramural hematoma and a minimal stent area (MSA) of 4.61 mm². Final angiography showed restoration of TIMI 3 flow in the RCA and TIMI I–II flow in the PDA without residual dissection.
Procedural Step1.mov
Procedural Step2.mov
Procedural Step3.mov
Case Summary
This case highlights the complexity of PCI in spontaneous coronary dissection. Technical challenges include wiring the true lumen, managing propagation of intramural hematoma, and maintaining side branch patency. IVUS imaging was crucial in identifying multiple dissection planes, hematoma extension, and plaque hemorrhage, guiding appropriate stent sizing and landing zones. Careful wire selection and controlled manipulation are essential to avoid false-lumen entry and further vessel injury. While drug-coated balloon therapy has been reported in selected cases, evidence remains limited.