Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251104_014
ISR CTO Treated With Laser Shock
By Yue Hin Tang
Presenter
Yue Hin Tang
Authors
Yue Hin Tang1
Affiliation
Princess Margaret Hospital, Hong Kong, China1
View Study Report
CASE20251104_014
Coronary - Complex PCI - CTO
ISR CTO Treated With Laser Shock
Yue Hin Tang1
Princess Margaret Hospital, Hong Kong, China1
Clinical Information
Relevant Clinical History and Physical Exam
A middle aged gentleman with cardiovascularrisk factors including diabetes, dyslipidaemia and 2 times of prior angioplastyto ostial-proximal left anterior descending (LAD) artery presented with typicalexertional chest discomfort again. Invasive coronary angiogram showed distalleft main/LAD/ramus/circumflex trifurcation disease with ostial LAD beingchronic total occluded. Angioplasty to left main/ramus/circumflex with drugcoated balloon was done first with staged angioplasty to LAD planned.
 LM trifurcation disease (2).avi
LM trifurcation disease (2).avi
LM trifurcation disease (3).avi
LM trifurcation disease.avi
Relevant Test Results Prior to Catheterization
Transthoracic echocardiogram showedimpaired left ventricular ejection fraction of 46% with hypokinetic apical andanteroseptal segments.
Echo.avi
Relevant Catheterization Findings
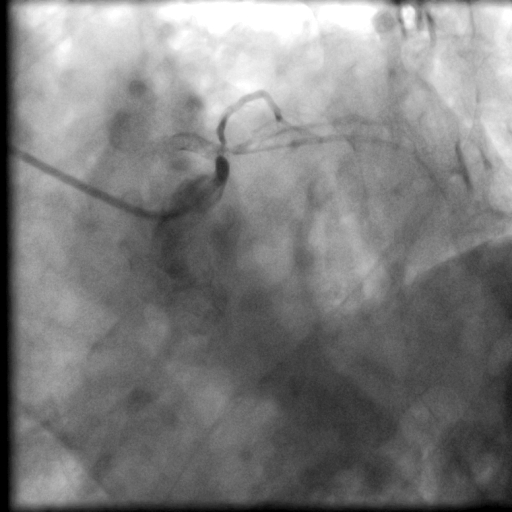
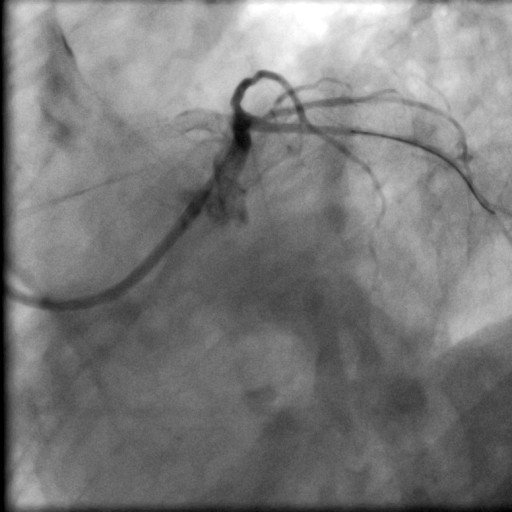
Angiogram showed satisfactory result overleft main/ramus/circumflex from prior drug coated balloon. LAD was totallyoccluded right from the ostium with an ambiguous proximal cap. Fortunately thecourse of the vessel was highlighted by the presence of calcium and stent, butthe CTO length was long. Bilateral dual injection showed faint retrograde fromright coronary artery only. J-CTO score was 3.
Bilateral injection.avi
Interventional Management
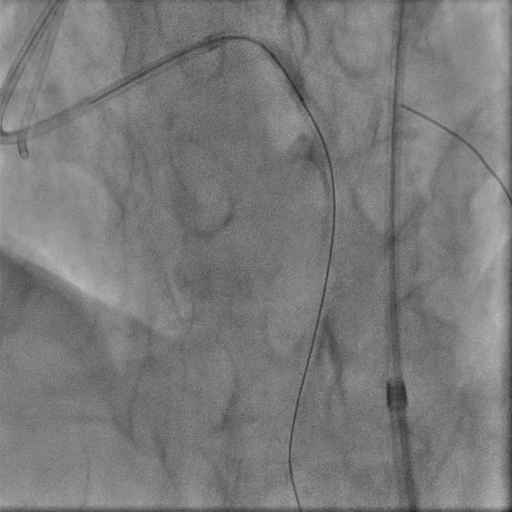
Procedural Step
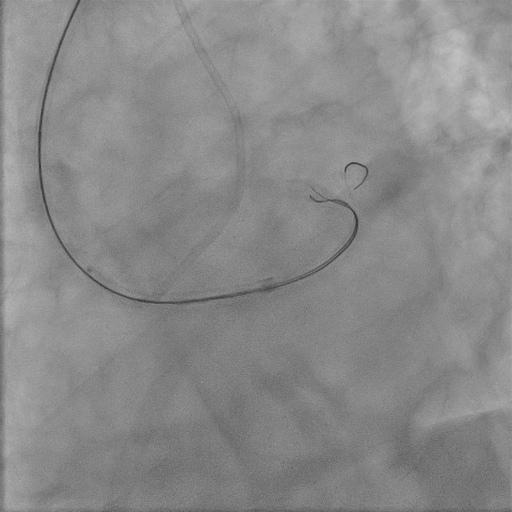
We used 7Fr EBU 3.5 guiding catheter to provide strong support, with diagnostic JR4 as contralateral injection. We started with antegrade wiring, which turned out to be difficult. There seemed to be a little bit of stump in the proximal cap but wire manipulation towards the stump was difficult, owing to the bending angle right at left main trifurcation as well as presence of calcium nodule in ostial stent. We failed proximal cap puncture despite escalating to Conquest Pro 12 loaded in single lumen microcatheter (SLC), which often backed off upon wire probing. Balloon assisted power puncture failed as well. To overcome the acute bending hindering wiring force exertion, we switched to an angulated microcatheter SuperCross120. By this manouvre we were able to advance our wire slightly into very proximal part of LAD stent, but it was deviated from central lumen and we failed to track down SLC. Hence we switched to parallel wire technique with use of a dual lumen microcatheter. The 2nd wire was able to reach the distal part of the stent only despite switching back to SLC and 1.0 balloon dilatation. Our next step was using the 0.9mm laser catheter to perform calcium modification within the ISR segment sequentially with saline, blood and contrast medium. After this manouvre, LAD was finally successfully wired with Fielder XTA, followed by balloon dilatation under IVUS guidance. Balloon expansion in ISR was suboptimal, hence it was treated with shockwave and drug coated balloon.

Laser.avi
Laser1.avi
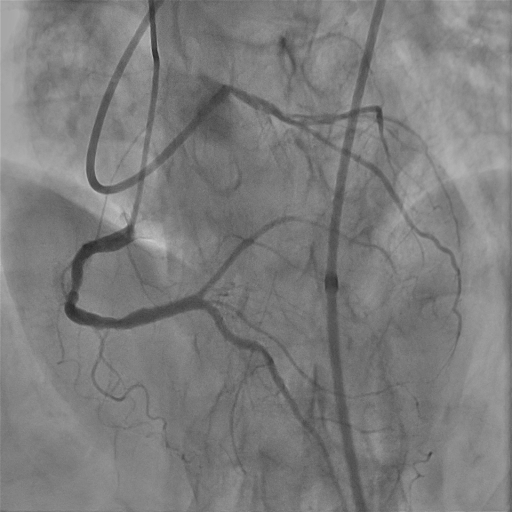
Final angiogram.avi
Case Summary
Percutaneous coronary angioplasty of chronic total occlusion (CTO) lesions requires meticulous planning with precise execution. Even the finest details matter and can affect outcome. As anatomy dictates strategy, choosing the correct weapons to attack the lesion is of paramount importance. Our case illustrated how we adapted to the anatomy and switched between different kinds of microcatheters in order to achieve an ideal attacking angle which ultimately led to procedural success. Another highlight would be the role of laser therapy in instent CTO lesions where use of other modalities of atherectomy may be limited by the presence of stents.