Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251104_012
Multimodality Approach to Calcified Lesion: A Case Study of PCI With Rotablator, Cutting Balloon and Intravascular Lithotripsy
By Khairani Ummah, Amir Aziz Alkatiri, Doni Firman, Arwin Saleh Mangkuanom, Nanda Iryuza
Presenter
Khairani Ummah
Authors
Khairani Ummah1, Amir Aziz Alkatiri1, Doni Firman1, Arwin Saleh Mangkuanom1, Nanda Iryuza1
Affiliation
National Cardiovascular Center Harapan Kita, Indonesia1
View Study Report
CASE20251104_012
Coronary - Complex PCI - Calcified Lesion
Multimodality Approach to Calcified Lesion: A Case Study of PCI With Rotablator, Cutting Balloon and Intravascular Lithotripsy
Khairani Ummah1, Amir Aziz Alkatiri1, Doni Firman1, Arwin Saleh Mangkuanom1, Nanda Iryuza1
National Cardiovascular Center Harapan Kita, Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
A 63 year old male complaining about angina on effort during his mild daily activities. Risk factor included diabetes mellitus, dyslipidemia , smoking and obesity. Physical examination was unremarkable.

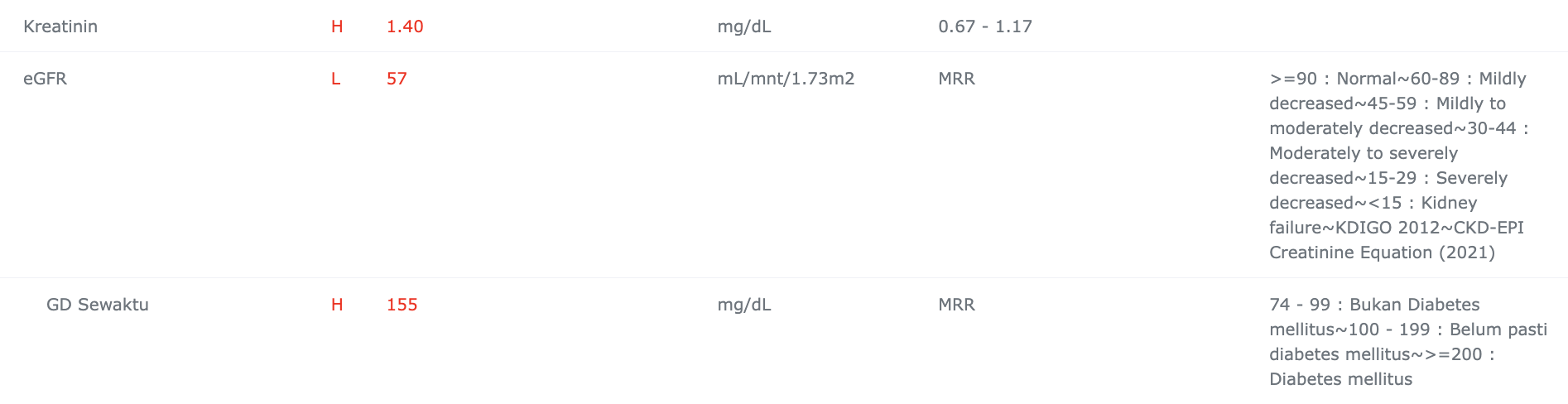
Relevant Test Results Prior to Catheterization
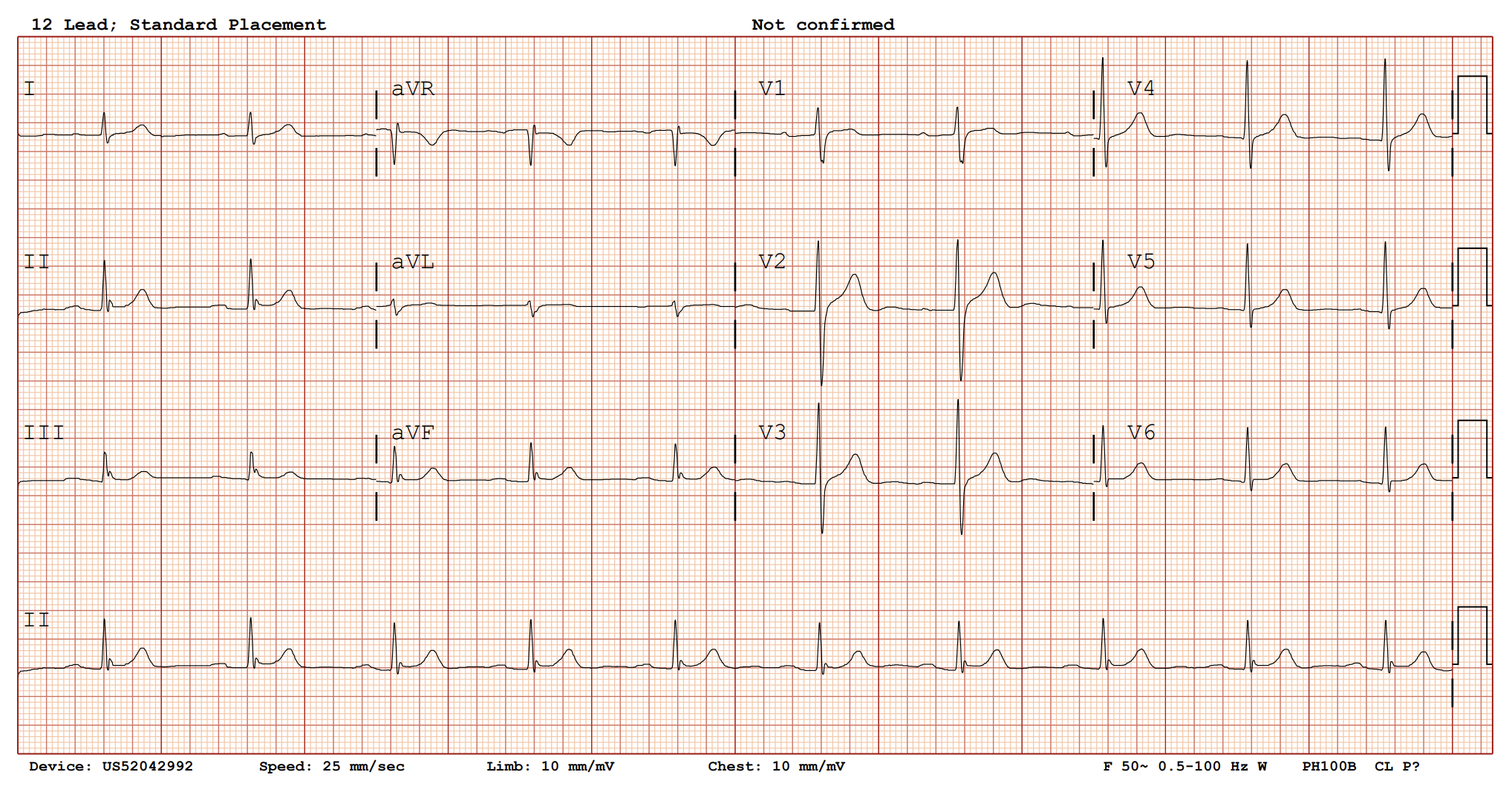
The patient presented with symptoms consistent with typical angina and a prior history of non-ST elevation myocardial infarction (NSTEMI) with unsuccessful revascularization. The resting electrocardiogram (ECG) showed no significant abnormalities.
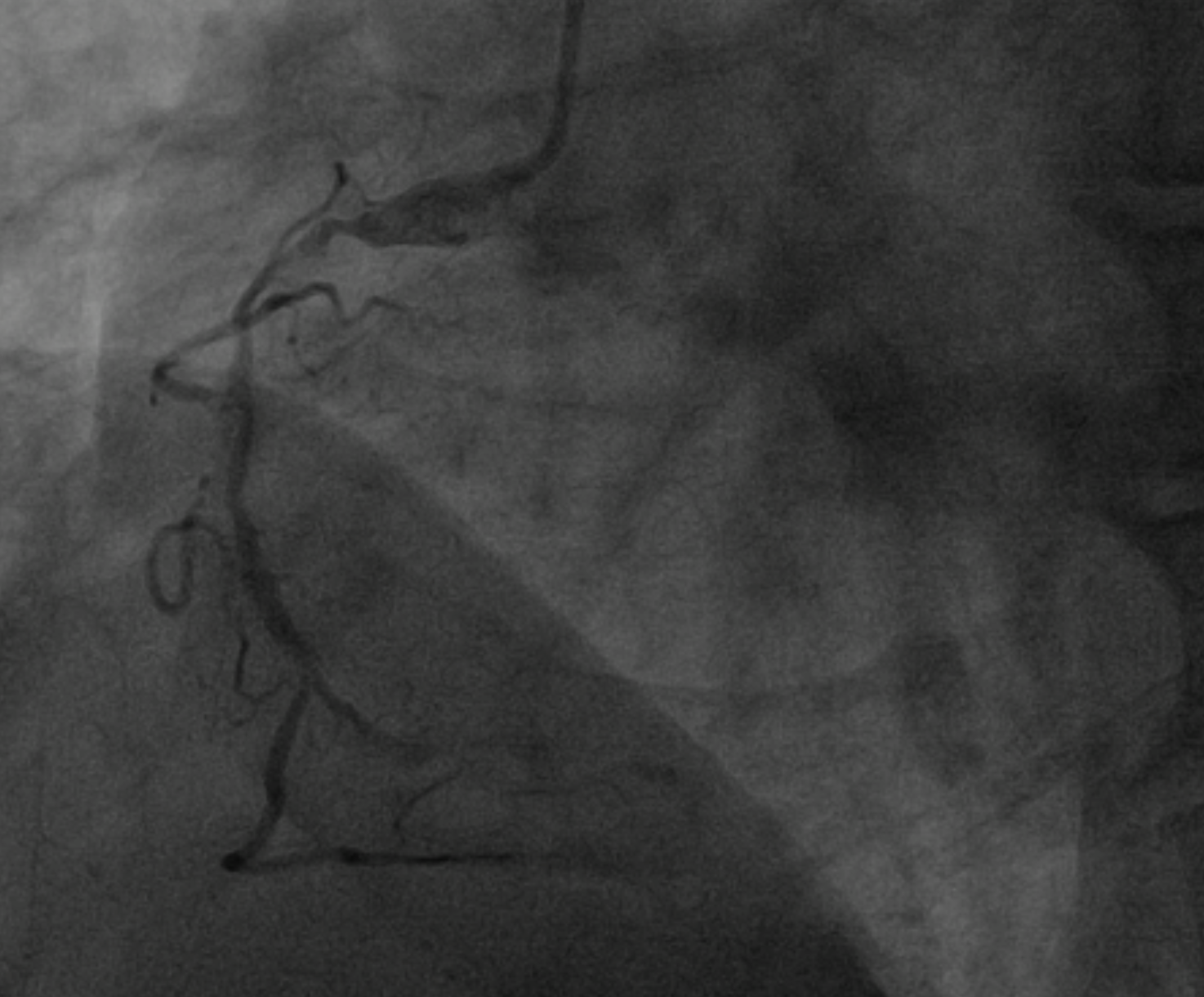
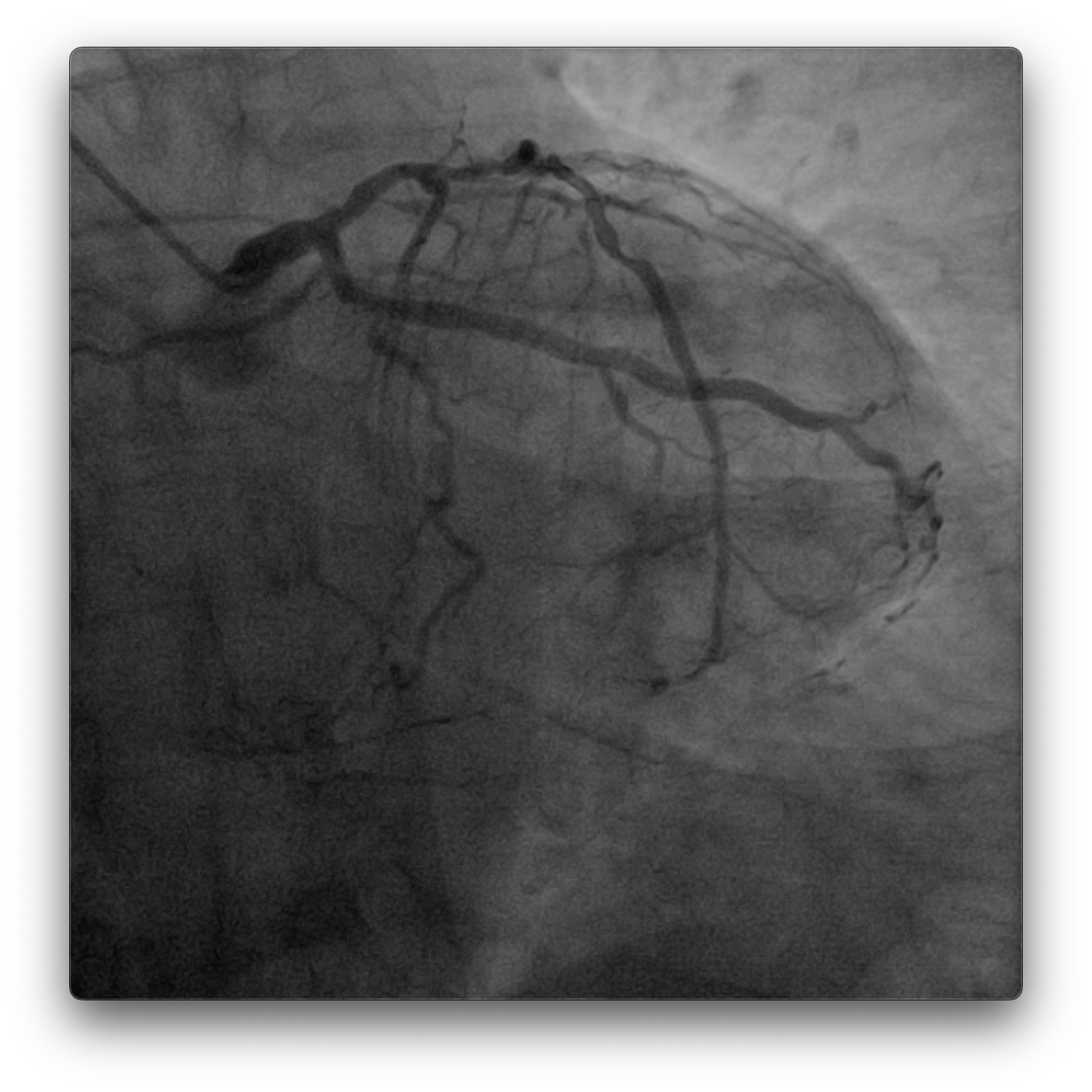
Relevant Catheterization Findings
Dominant right coronary artery (RCA) with a heavily calcified, diffusely diseased segment extending from the ostium to the distal portion. The left anterior descending (LAD) and left circumflex (LCx) arteries show irregular but non-significant stenoses

 Coronary_15_fps_1_1.mp4
Coronary_15_fps_1_1.mp4
Coronary_15_fps_4_4.mp4
Coronary_15_fps_5_5.mp4
Interventional Management
Procedural Step
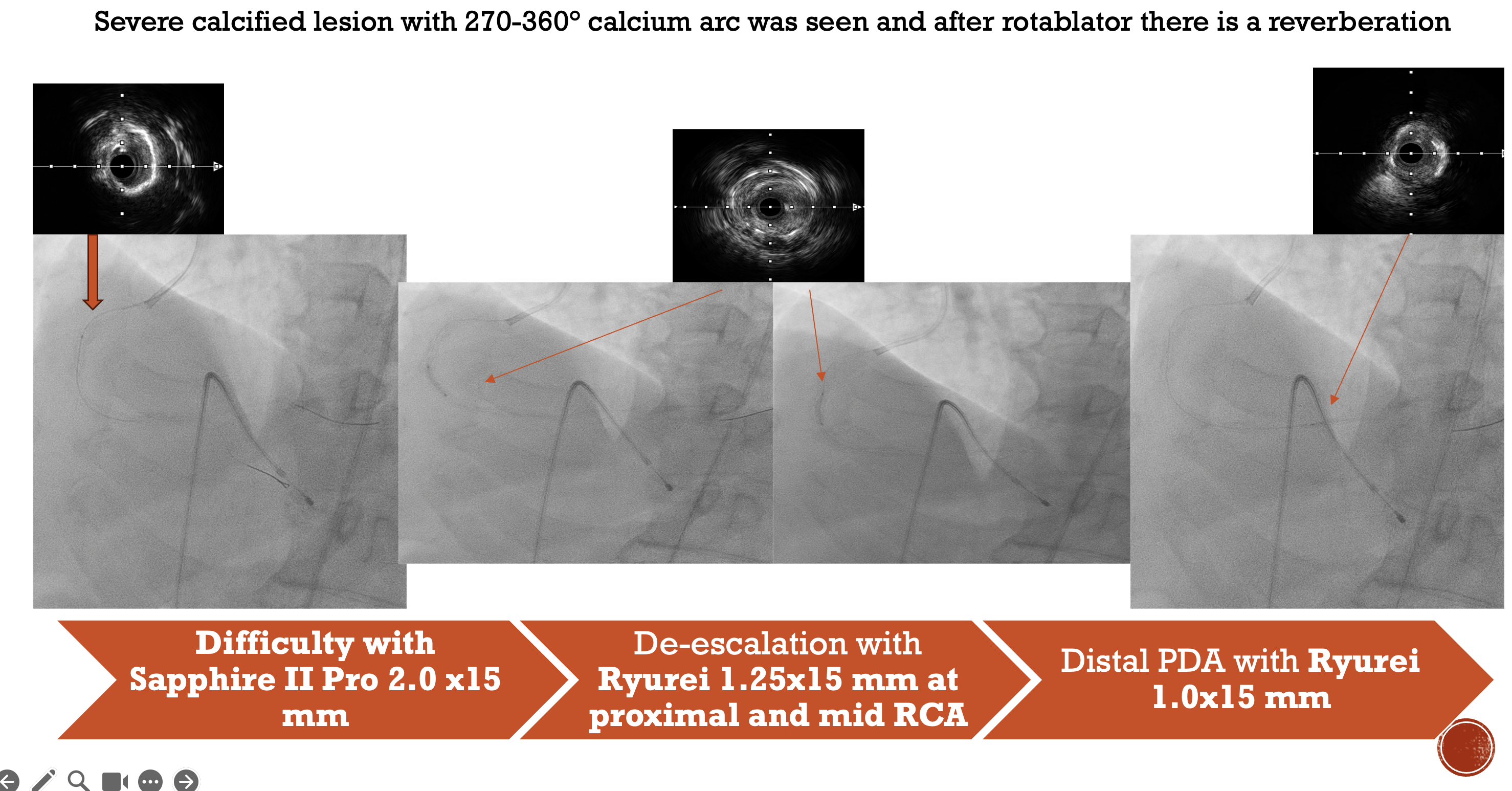
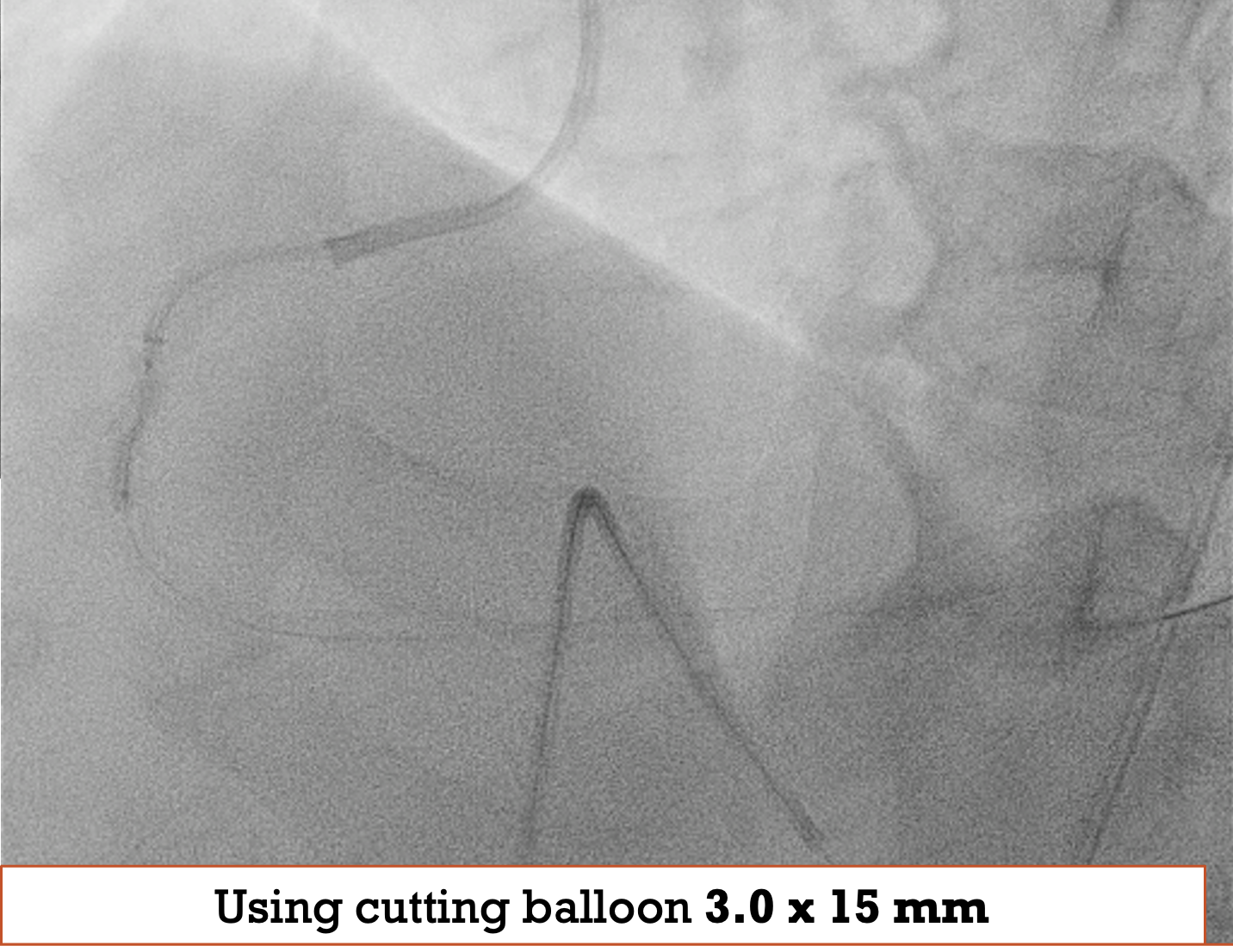
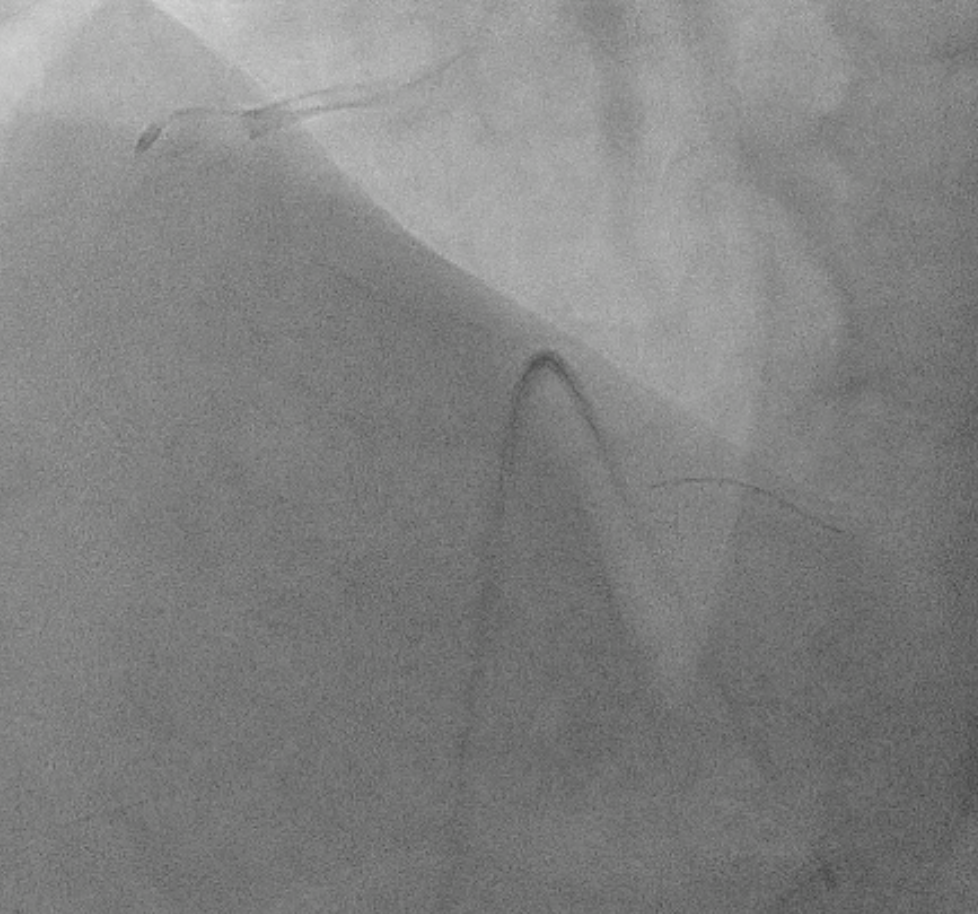
PCI to RCA : Canulation using guiding catheter AL 0.75/7Fr, heparin was administered. Workhorse wire to distal PL. Initial attempt with a 1.5 × 15 mm balloon failed to cross the distal lesion and subsequently ruptured. Rotational atherectomy was performed using a 1.5 mm burr at 160–180k rpm with three runs and one polishing pass. A 2.0 × 15 mm semi-compliant balloon was then advanced from distal to proximal segments with the assistance of a guide extension catheter.IVUS evaluation demonstrated a 360° circumferential calcium arc and multiple calcium nodules extending from proximal to distal RCA. Lesion preparation was continued using sequential scoring balloon 2.0 mm and NC 2.5 mm, and cutting balloon 3.0 mm at high pressure. A “dogbone” appearance was noted with the cutting balloon at the proximal RCA. An intravascular lithotripsy (IVL) balloon 3.0 mm was then applied to both distal and proximal RCA, delivering a total of 120 pulses (up to 8 atm).Repeat IVUS confirmed adequate calcium modification and optimal lesion preparation. Three overlapping drug-eluting stents (DES) were deployed: 3.0 × 38 mm (distal–mid RCA), 3.5 × 32 mm (mid RCA), and 4.0 × 22 mm (ostial–proximal RCA), followed by sequential post-dilatation up to 4.0 mm. Final IVUS confirmed good stent apposition and expansion, with a minimal stent area of 6.36 mm² at the distal RCA. TIMI 3 flow was achieved. Total contrast volume: 160 mL, Fluoroscopy time: 01:09:34 minutes, DAP: 232 Gy·cm²
IVUS Run post Rota and IVL.mp4
Coronary_15_fps_Low_88_94.mp4
Fluoroscopy__stored_22_25.mp4
Case Summary
A stepwise multimodality approach combining rotational atherectomy, specialty balloons, and IVL achieved optimal stent expansion in a severely calcified RCA. Intravascular imaging guidance was essential for safe and successful procedural outcome. All target vessels reached optimal stent expansion and TIMI 3 flow without complications.