Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251104_010
A Successful CHIP Intervention for Cardiopulmonary Arrest Due to Myocardial Infarction Combined With Abdominal Aortic Aneurysm Impending Rupture
By Makio Muraishi, Kotaro Obunai
Presenter
Makio Muraishi
Authors
Makio Muraishi1, Kotaro Obunai1
Affiliation
Tokyo Bay Urayasu Ichikawa Medical Center, Japan1
View Study Report
CASE20251104_010
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
A Successful CHIP Intervention for Cardiopulmonary Arrest Due to Myocardial Infarction Combined With Abdominal Aortic Aneurysm Impending Rupture
Makio Muraishi1, Kotaro Obunai1
Tokyo Bay Urayasu Ichikawa Medical Center, Japan1
Clinical Information
Relevant Clinical History and Physical Exam
A 64-year-old man with a previous history of percutaneous coronary intervention (PCI) to the right coronary artery presented with dyspnea on exertion for 2 weeks. He was transferred to our hospital due to newly developed chest and abdominal pain on the day of admission. On presentation, vital signs indicated a pre-shock status: heart rate 97 bpm, blood pressure 106/86 mmHg, respiratory rate 24/min, and SpO₂ 97% on room air. He was diaphoretic and complained of coldness in his extremities.
Relevant Test Results Prior to Catheterization
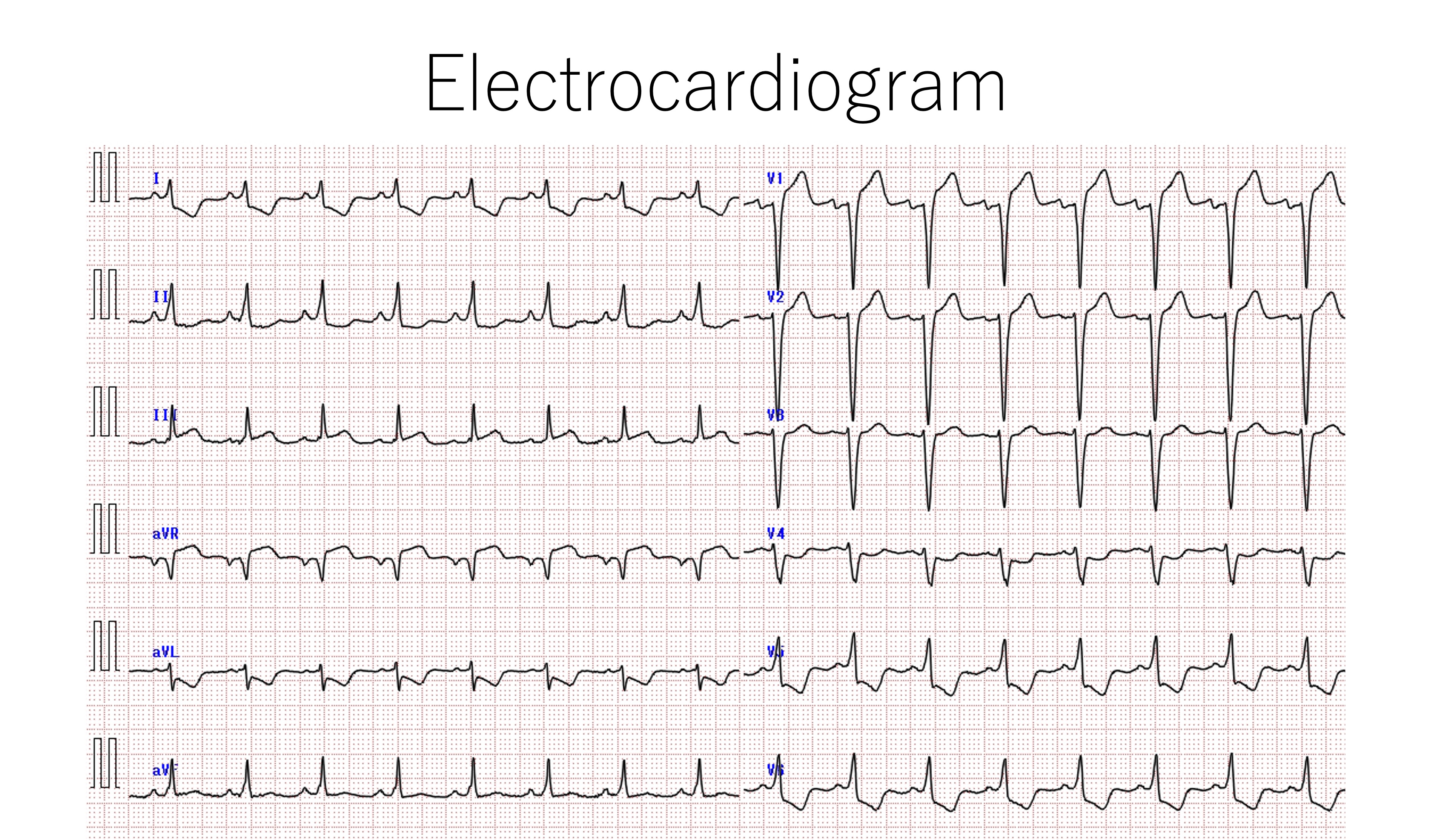
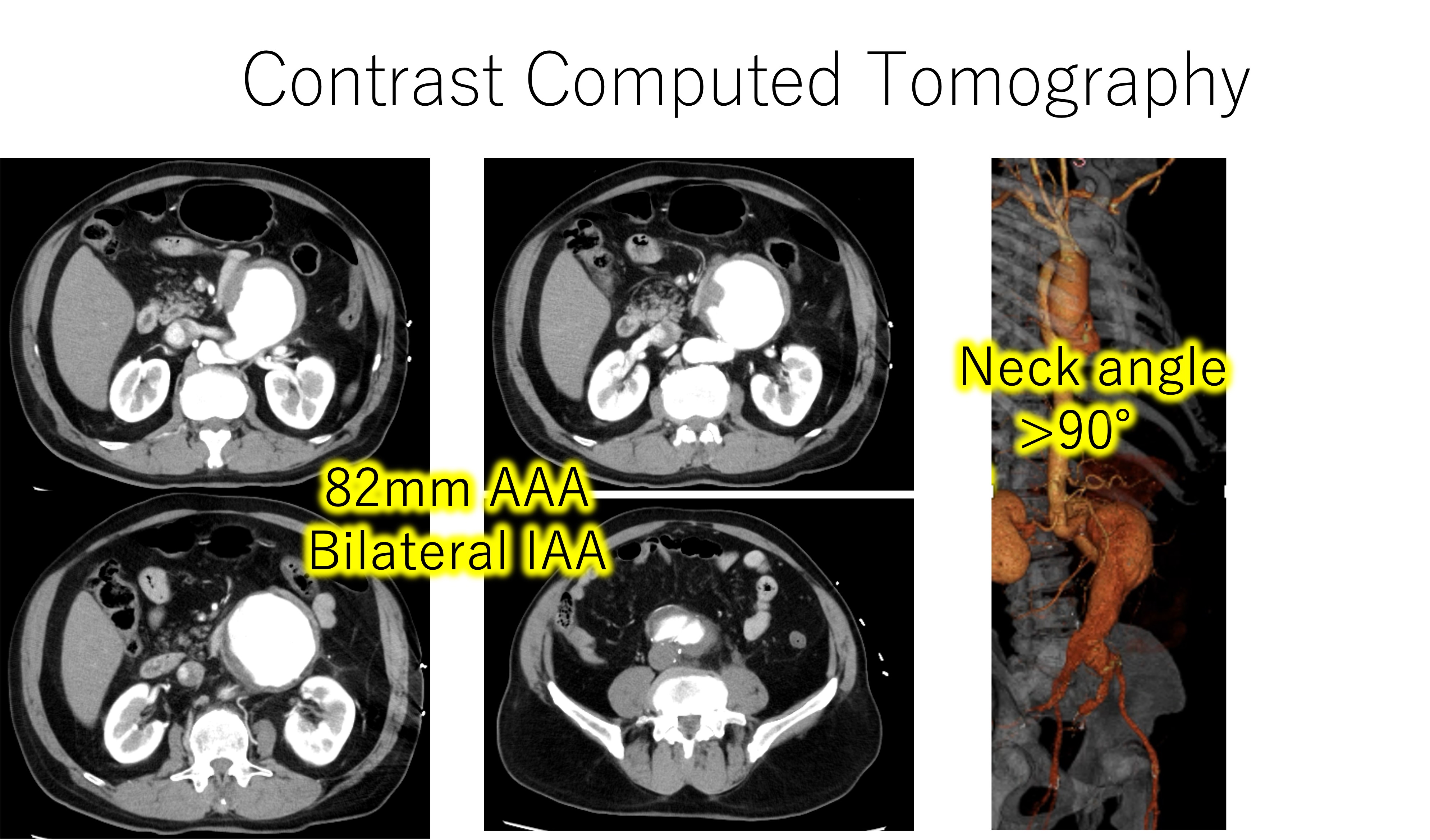
electrocardiogram revealed ST elevation in lead aVR and ST depression in leadⅠ,Ⅱ, aVL, V4-6, consisted with acute coronary syndrome (ACS), while transthoracic echocardiography showed severe left ventricular dysfunction (ejection fraction: approximately 20%). Contrast computed tomography revealed 82mm infra-renal abdominal aortic aneurysm (AAA) with a sign of impending rupture. laboratory blood test showed elevated troponin I level (3.48 ng/ml).
Relevant Catheterization Findings
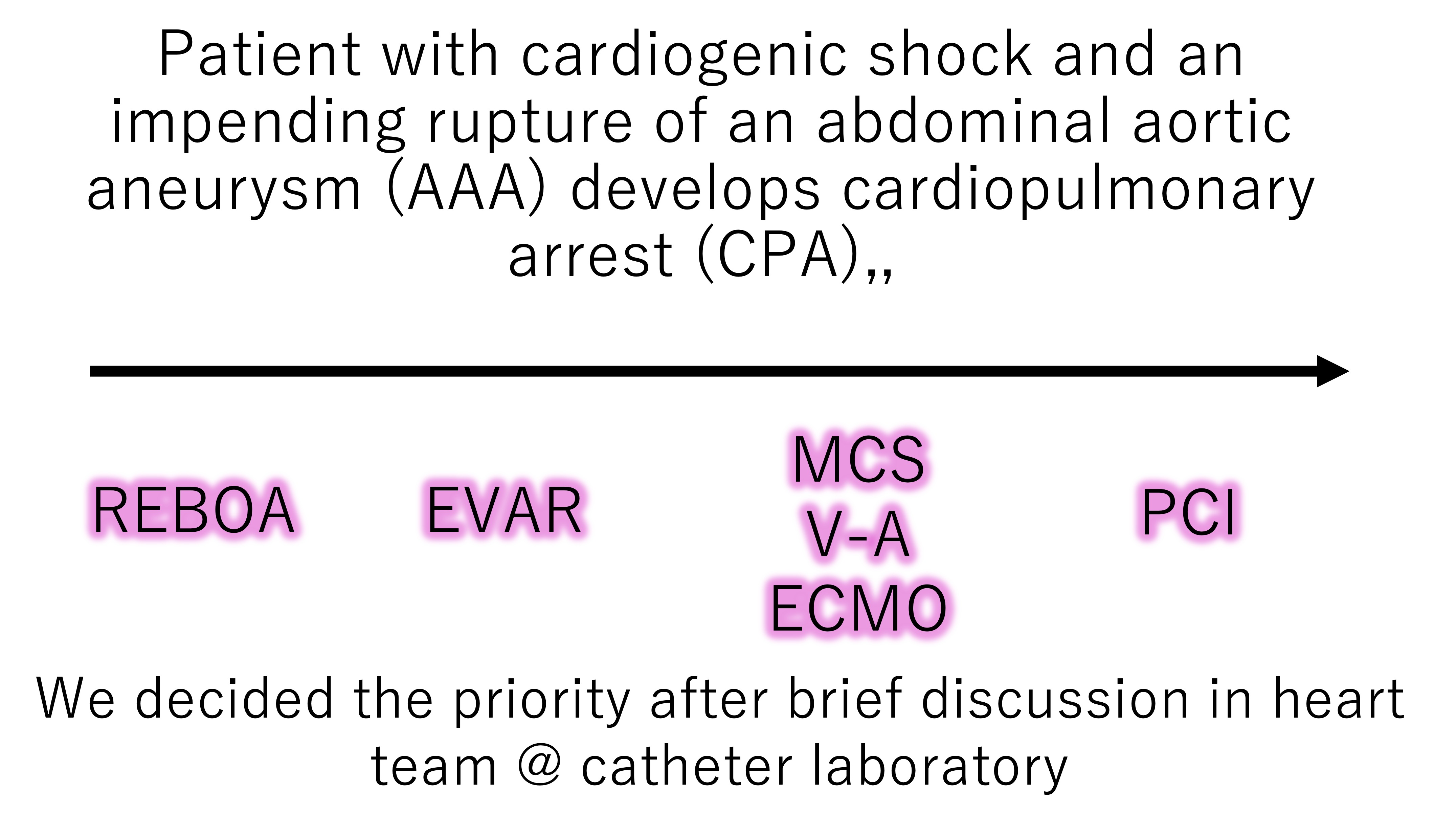
Unfortunately, the patient became cardiopulmonary arrest (CPA) on the way to catheterization laboratory. Emergent coronary angiography and PCI should have been performed, but after brief heart team discussion, decision was made to perform endovascular aortic repair (EVAR) first, to secure the AAA prior to introducing mechanical circulatory support.
Interventional Management
Procedural Step
EVAR was performed during resuscitation followed by introducing Veno-Artrial Extracorporeal Membrane Oxygenation (V-A ECMO). Then, CAG revealed severe multivessel disease (chronic total occlusion at proximal RCA, 99% stenosis at LAD ostium and LCX ostium) and PCI was performed to LMT-LAD with the ECMO support. Finally, Impella 5.5 was surgically introduced via the right subclavian artery. These procedures, performed by the heart team (including interventionists, cardiac surgeons, and intensivists), resulted in rescue of the patient.
Case Summary
We experienced a case of cardiogenic shock and cardiopulmonary arrest (CPA) caused by the coexistence of acute coronary syndrome (ACS) and an impending rupture of an abdominal aortic aneurysm (AAA).
In cases of cardiogenic shock or CPA due to complex underlying conditions, determining the priority of interventions and rapidly sharing information within the heart team are essential for successful resuscitation.
In cases of cardiogenic shock or CPA due to complex underlying conditions, determining the priority of interventions and rapidly sharing information within the heart team are essential for successful resuscitation.