Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251104_008
Kissing Stent Technique for SVC Syndrome in an ESRD Patient on Hemodialysis: Dual Venous Outflow Restoration
By Chi-Chen Yang, Chon-Seng Hong
Presenter
Chi-Chen Yang
Authors
Chi-Chen Yang1, Chon-Seng Hong1
Affiliation
Chi-Mei Medical Center, Taiwan1
View Study Report
CASE20251104_008
Endovascular - Venous Disease Intervention
Kissing Stent Technique for SVC Syndrome in an ESRD Patient on Hemodialysis: Dual Venous Outflow Restoration
Chi-Chen Yang1, Chon-Seng Hong1
Chi-Mei Medical Center, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
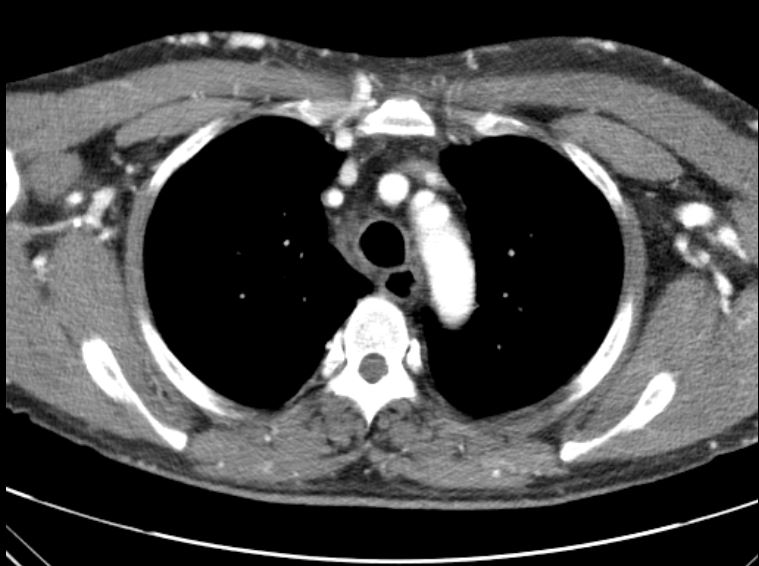
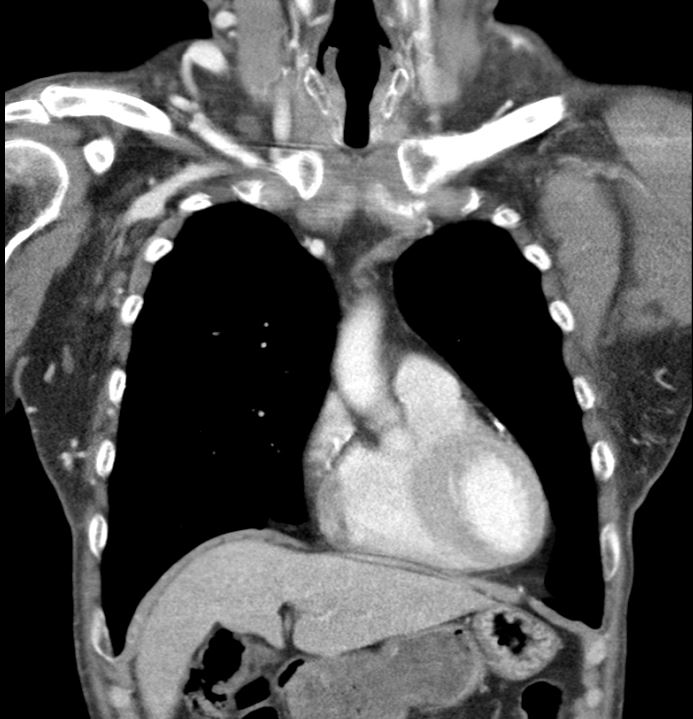
A 53-year-old man with type 2 diabetes, hypertension, COPD, and end-stage renal disease on hemodialysis presented with progressive facial swelling for one month. Vital signs were stable. Examination revealed a high-pitched voice, facial and bilateral upper limb swelling, and prominent chest wall venous engorgement. Chest CT showed bilateral brachiocephalic vein obstruction with multiple collaterals, consistent with superior vena cava (SVC) syndrome.
Relevant Test Results Prior to Catheterization
Chest CT revealed chronic thrombosis of the left brachiocephalic vein and a diminutive right brachiocephalic vein with multiple collateral channels, findings consistent with superior vena cava (SVC) syndrome secondary to chronic central venous obstruction.
Relevant Catheterization Findings
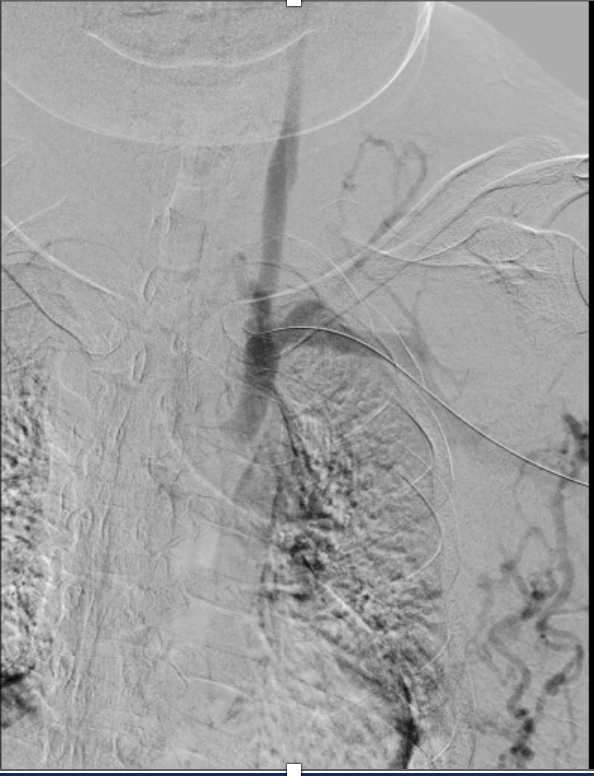
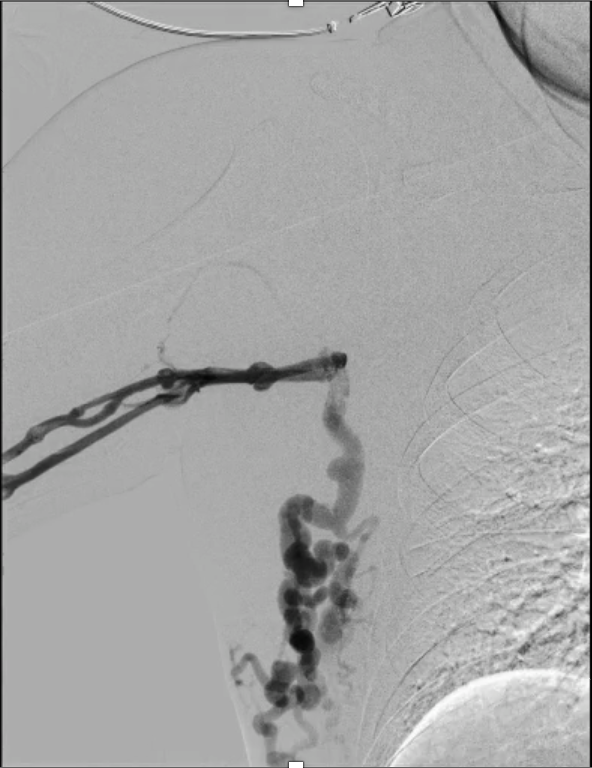
Bilateral venography demonstrated complete occlusion of both brachiocephalic veins with extensive collateral formation.
Interventional Management
Procedural Step
Real-time echo-guided puncture of both basilic veins was performed, and 6 Fr sheaths were inserted bilaterally.

 17731865(6).mp4
17731865(6).mp4
17731865(8).mp4
17731865(60).mp4
Case Summary
Successful endovascular revascularization was achieved in a patient with superior vena cava syndrome secondary to chronic bilateral brachiocephalic vein occlusion. High-pressure balloon angioplasty followed by bilateral stent deployment restored venous patency and relieved symptoms. This case highlights the feasibility and effectiveness of endovascular therapy in dialysis-related chronic central venous obstruction.