Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251104_007
Taming the Curve: Snare-Assisted Self-Expandable Valve Delivery in Type I BAV With Steep LV–Aorta Angle
By Harilalith Kovvuri, Akshay Prashanth Giri, Ramesh Sankaran, Nagendra Boopathy Senguttuvan
Presenter
Harilalith Kovvuri
Authors
Harilalith Kovvuri1, Akshay Prashanth Giri1, Ramesh Sankaran1, Nagendra Boopathy Senguttuvan1
Affiliation
Sri Ramachandra Institute of Higher Education and Research, India1
View Study Report
CASE20251104_007
Structural - Aortic Valve Intervention - Bicuspid AV
Taming the Curve: Snare-Assisted Self-Expandable Valve Delivery in Type I BAV With Steep LV–Aorta Angle
Harilalith Kovvuri1, Akshay Prashanth Giri1, Ramesh Sankaran1, Nagendra Boopathy Senguttuvan1
Sri Ramachandra Institute of Higher Education and Research, India1
Clinical Information
Relevant Clinical History and Physical Exam
An 80-year-old male with diabetes, hypertension, and chronic bronchiectasis presented with worsening dyspnea, progressing from NYHA II to IV heart failure with recurrent decompensation despite optimal therapy. Examination showed mild pedal edema, bilateral coarse crepitations, and a grade 3/6 ejection systolic murmur radiating to carotids, suggestive of severe aortic stenosis. He was evaluated with ECG, echocardiography, and CT TAVI protocol.
Relevant Test Results Prior to Catheterization
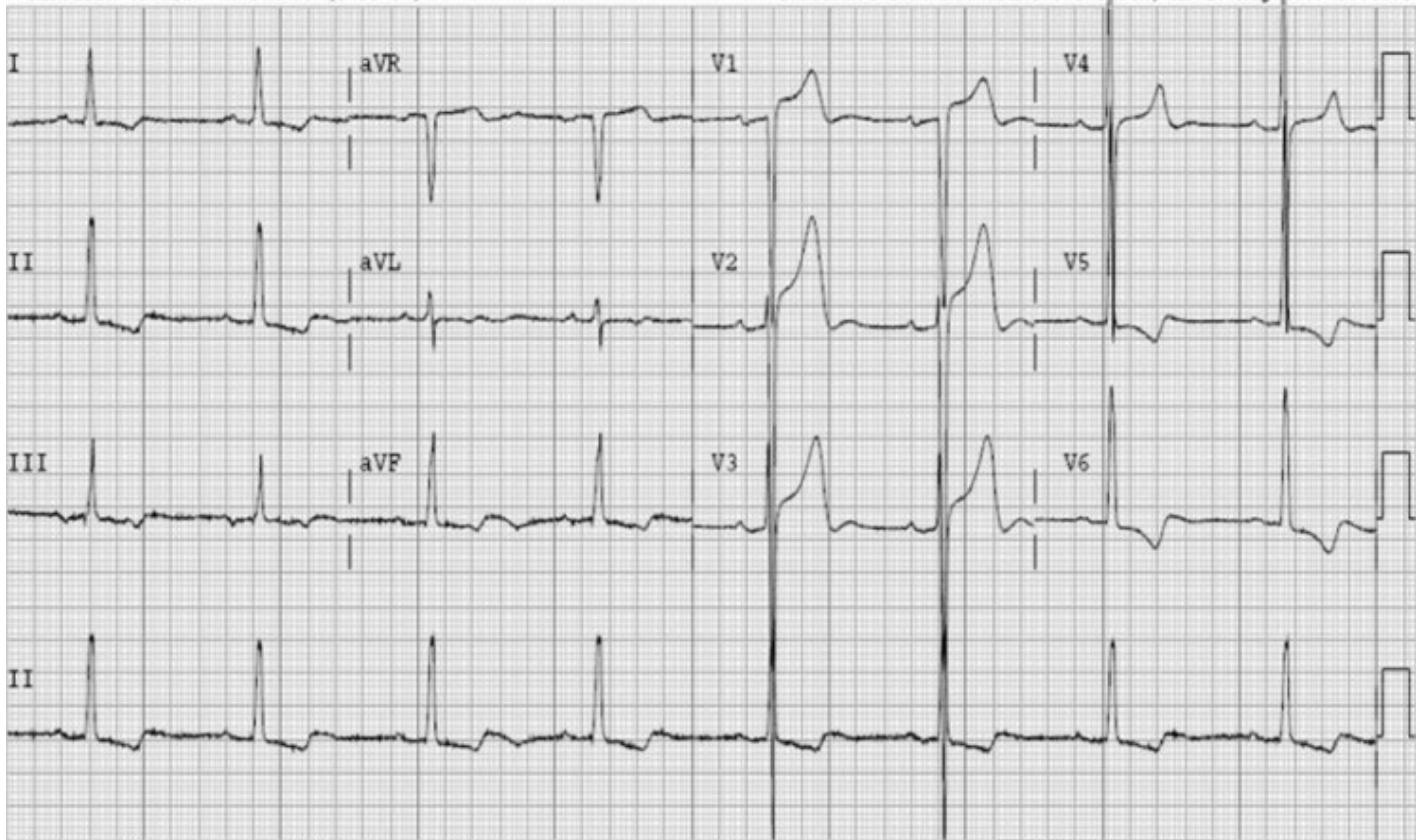
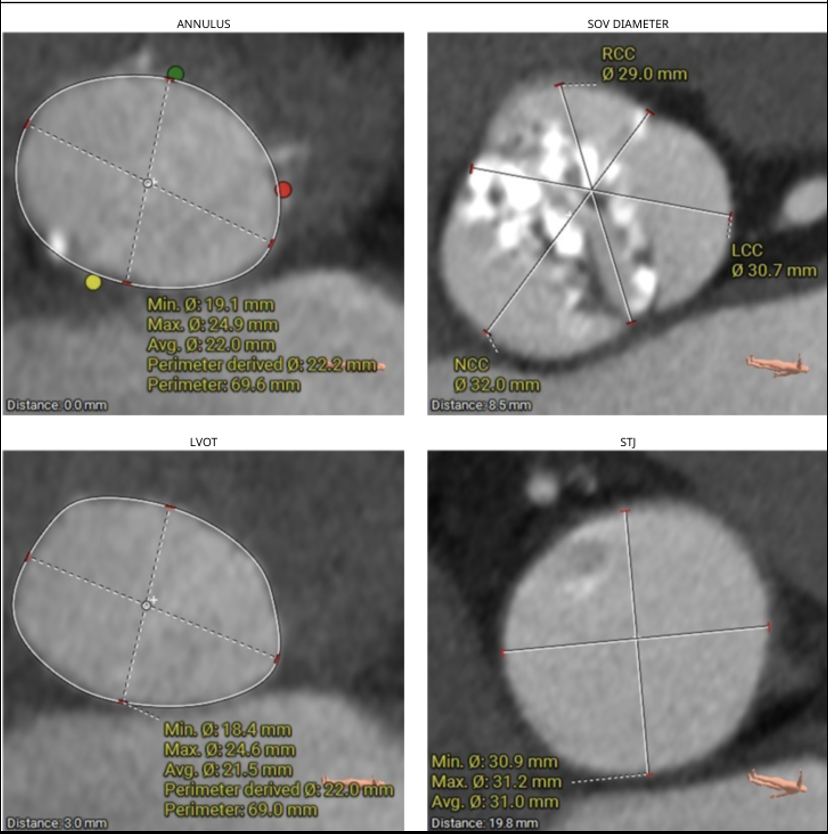
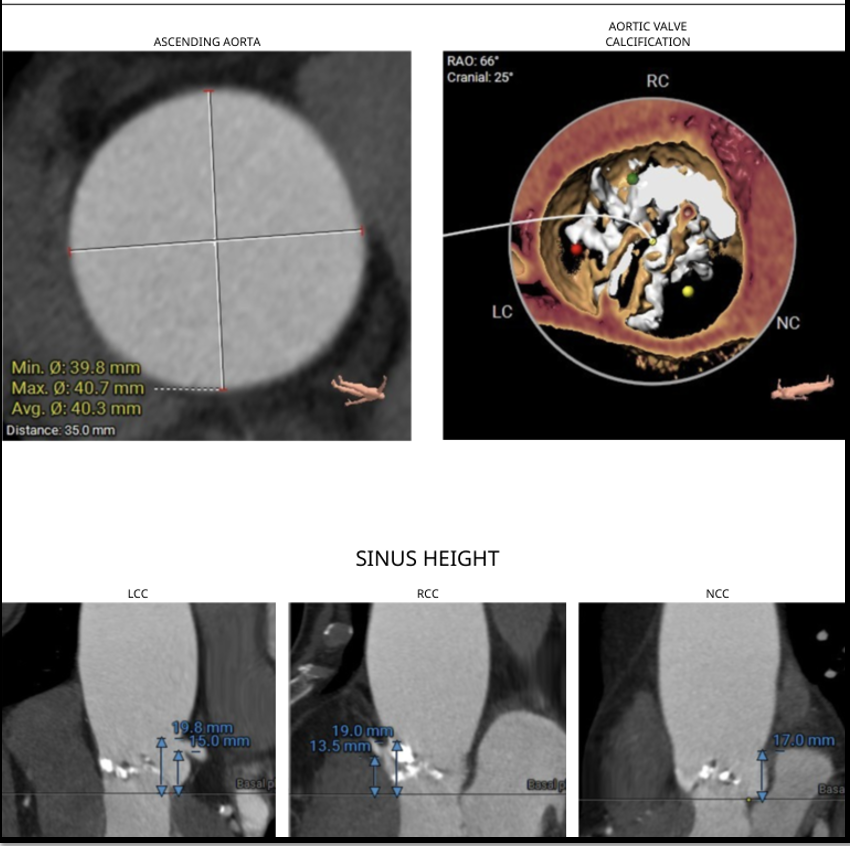
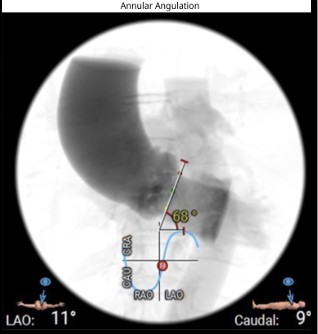
ECG revealed features of left ventricular hypertrophy. 2D echocardiography showed preserved left ventricular ejection fraction with severe calcific aortic stenosis, CT-TAVI protocol revealed Type 1 bicuspid aortic valve (R-L fusion), dilated ascending aorta, a perimeter-derived annulus of 22.2 mm (average 22 mm), sinus of Valsalva diameters RCC 29 mm, LCC 30.7 mm, NCC 32 mm, LVOT perimeter 22 mm, significant valve calcification, steep LVOT angle (68°), and well-sized, non-tortuous femoral access
Relevant Catheterization Findings
The preprocedural risk assessment revealed a EuroSCORE II of 12.6% and an STS score of 16.1%, confirming prohibitive surgical risk. Advised for transfemoral TAVI, snare assisted delivery of self-expanding valve.
Interventional Management
Procedural Step
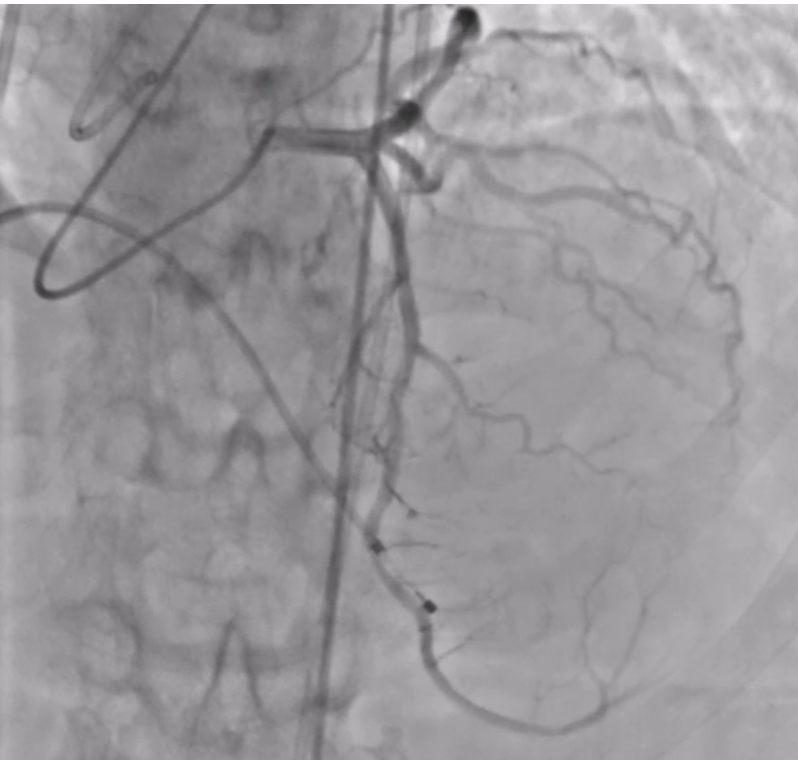
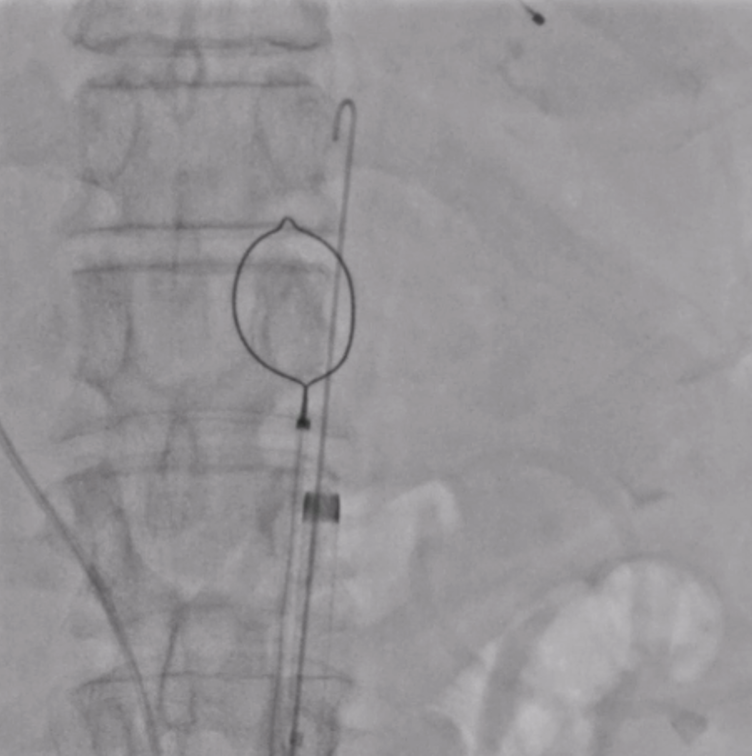
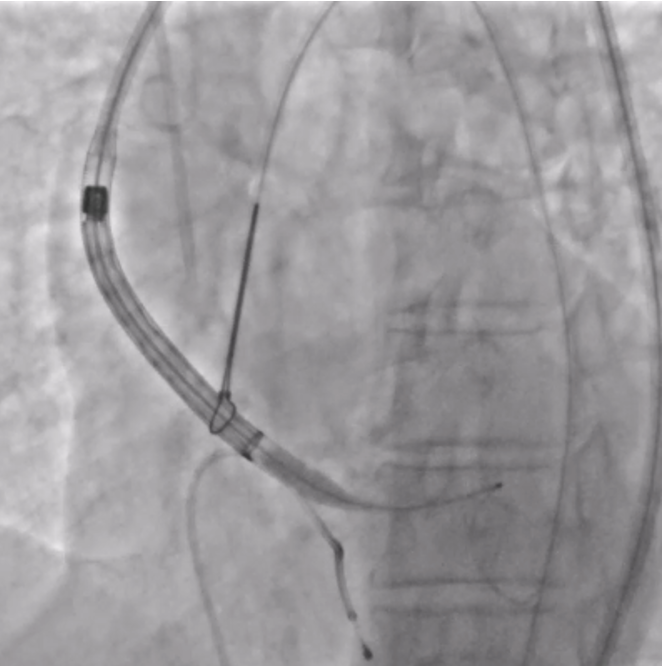
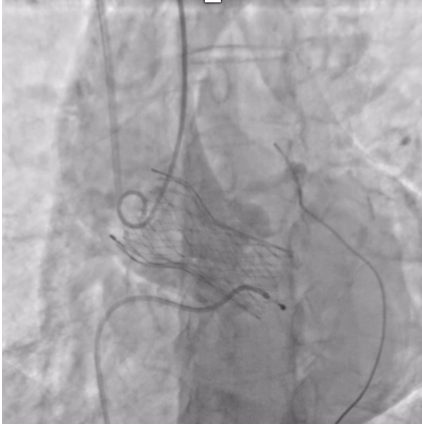
The patient was planned for transfemoral TAVI. Both left and right femoral arteries were punctured under ultrasound guidance. A temporary pacemaker (TPA) was placed in the right ventricle via the left femoral artery, and the right femoral artery sheath was upgraded to the 14Fr sheath. Selective left coronary angiography revealed normal coronaries. Through the right femoral artery, a snare was deployed in the abdominal aorta. The native bicuspid aortic valve was crossed with an Lunderquist wire, which was advanced into the left ventricle. Using pigtain, angiographic gradient was measured, showing severe aortic stenosis. Predilatation was performed using a 20 mm Z-MED balloon with satisfactory results. The TAVI valve, a self-expanding valve, was advanced across the native valve with the aid of the snare and positioned accurately in the cusp-overlap view. Under rapid pacing, the valve was deployed up to 80%, and after confirming satisfactory depth, full deployment was completed in the coplanar view. Final angiographic assessment showed no paravalvular leak (PVL) or aortic regurgitation (AR), with valve depth of 4–5 mm at the NCC and 6–7 mm at the LCC. Femoral closure was performed successfully without vascular complications.
 PRE DIL.mp4
PRE DIL.mp4
Snare.mp4
Final.mp4
Case Summary
In patients with severe calcific aortic stenosis and Type 1 bicuspid anatomy with a steep LV–aortic angle, transfemoral TAVI using a snare-assisted technique facilitates safe and controlled valve delivery. This approach ensures optimal coaxial alignment, minimizes resistance during advancement of the self-expanding valve, and prevents aortic sinus or annular injury, resulting in precise deployment and excellent procedural outcome without complications.