Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251104_005
When Perfection Is a Luxury - A Primary PCI Case Report in Rural Areas
By Alvin Tonang
Presenter
Alvin Tonang
Authors
Alvin Tonang1
Affiliation
Dr. Adhyatma (Tugurejo) General Hospital, Semarang, Indonesia1
View Study Report
CASE20251104_005
Coronary - ACS/AMI
When Perfection Is a Luxury - A Primary PCI Case Report in Rural Areas
Alvin Tonang1
Dr. Adhyatma (Tugurejo) General Hospital, Semarang, Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
Our patient is a 42-year-old gentleman with crushing chest pain in the middle of the night. At presentation, it was 1 hour onset. He was an active heavy smoker, fully alert with sweating. His body mass index was 26 kg/m2. His blood pressure was 147/95 mmHg, heart rate 72 bpm, with respiratory rate 24 per minutes, with good oxygen saturation (100% with nasal cannulae 3 lpm). Physical examination was done with unremarkable results. There were no signs of heart failure nor cardiogenic shock.
Relevant Test Results Prior to Catheterization
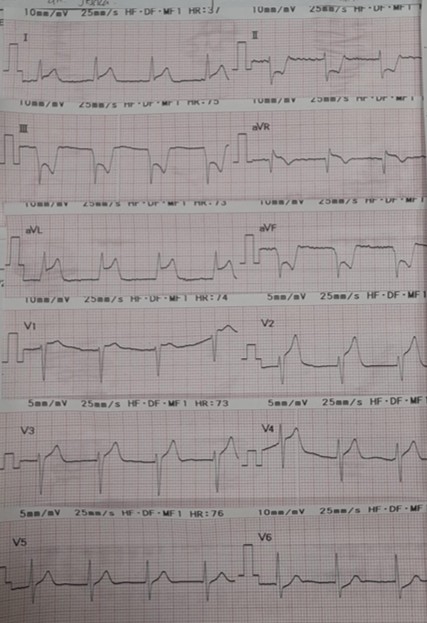
The emergency department immediately did the ECG, and revealed an anterior extensive ST-segment elevation, with slight aVR lead-elevation and a reciprocal ST-segment depression in inferior lead. Laboratory test result came back with negative troponin (0.01 ng/mL), with good renal function BUN 15 mg/dL, creatinine 0.98 mg/dL, and with eGFR 99 mL/min/1.73 m2.
Relevant Catheterization Findings
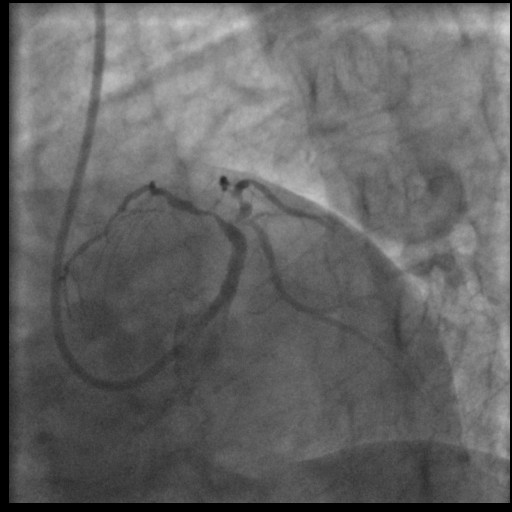
We immediately activated the Cath-lab and did the Primary PCI. We used radial access and 6F sheath, and the using Tig-5F catheter, we cannulated RCA and LCA. The culprit lesion was in the left main artery and a TIMI flow 0. RCA had a good TIMI flow, with borderline lesion in proximal to mid part.
 LCA1.avi
LCA1.avi
LCA2.avi
RCA.avi
Interventional Management
Procedural Step
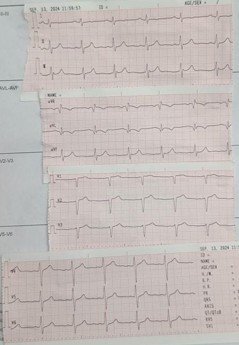
PPCI was done with GC XB 3,5/6F, followed by wiring the LAD using GW RNS hypercoat and double wired LCX using GW Sion Blue. Thrombosuction couldn’t pass the tight lesion in LM, so we removed the Sion Blue, and continued the thombosuction from the LM to distal LAD. We successfully retrieved some thrombus, and we appreciate significant stenosis in the LM, with TIMI flow II. We did the balloon predilatation using SC balloon 2,5x15 mm (up to 14 atm), but the patient became unstable and VT. CPR and defib 200 J was done. After stabilisation, we evaluate that the flow was greatly reduced, back to TIMI flow 0. Thus we decided that we have to restored the flow as soon as possible, we did stenting with DES 3,5x16 mm (up to 14 atm). TIMI flow III was achieved, despite there is still lesion in LAD and the LCX. Due to limited resources and patient was stabilized with good hemodynamic, we decided to stop the procedure. Patient stayed 2 days in ICU, and no further VT/VF episodes. Echocardiogram was done, EF was 43% (biplane), and we still appreciated the wall motion abnormality in anterior segment. He was discharged in 5th days. Without chest pain and stable with good hemodynamic. ECG showed complete ST-segment resolution without Q-wave. He was then referred to a bigger hospital with better resources to achieved a complete revascularization.

after thrombosuction.avi
TIMI Flow reduced again.avi
post PPCI.avi
Case Summary
Despite the limited resources in the rural area, we tried to save as much myocardium as possible, even though complete revascularisation was recommended by the guideline. Thus the goal of PPCI was to restored the epicardial infarct-related artery patency as soon as possible. We also aware that the lesion preparation was not perfect and the stent most likely is undersized. Still we believed that achieving microvascular reperfusion is important in every primary PCI cases. Thus this is the case where perfection maybe is a luxury, but as and interventionist we still try to give the best that we can do in the rural area.