Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251104_004
Direct Stenting in Primary PCI of Acute ST-Elevation Myocardial Infarction May Prevent Distal Embolization
By Md Mohasin Uddin, Mahbubor Rahman, Mohammad abul Khayer, Shiblee Sadik Pathan, Md Asifudduza Asif, Rashiduz Zaman, Md Monoarul Islam
Presenter
Md Mohasin Uddin
Authors
Md Mohasin Uddin1, Mahbubor Rahman1, Mohammad abul Khayer1, Shiblee Sadik Pathan1, Md Asifudduza Asif1, Rashiduz Zaman1, Md Monoarul Islam1
Affiliation
Labaid Cardiac Hospital, Bangladesh1
View Study Report
CASE20251104_004
Coronary - ACS/AMI
Direct Stenting in Primary PCI of Acute ST-Elevation Myocardial Infarction May Prevent Distal Embolization
Md Mohasin Uddin1, Mahbubor Rahman1, Mohammad abul Khayer1, Shiblee Sadik Pathan1, Md Asifudduza Asif1, Rashiduz Zaman1, Md Monoarul Islam1
Labaid Cardiac Hospital, Bangladesh1
Clinical Information
Relevant Clinical History and Physical Exam
A 52 years old gentlemen presented with complaints of sudden onset of severe chest pain for 6 hour. Risk factor are smoking , diabetes mellitus , dyslipidemiaOn admission BP 110/70mmhg, Pulse 58 / min, SpO2 98%Cardiovascular examination : NAD . lungs base are clear .
Relevant Test Results Prior to Catheterization
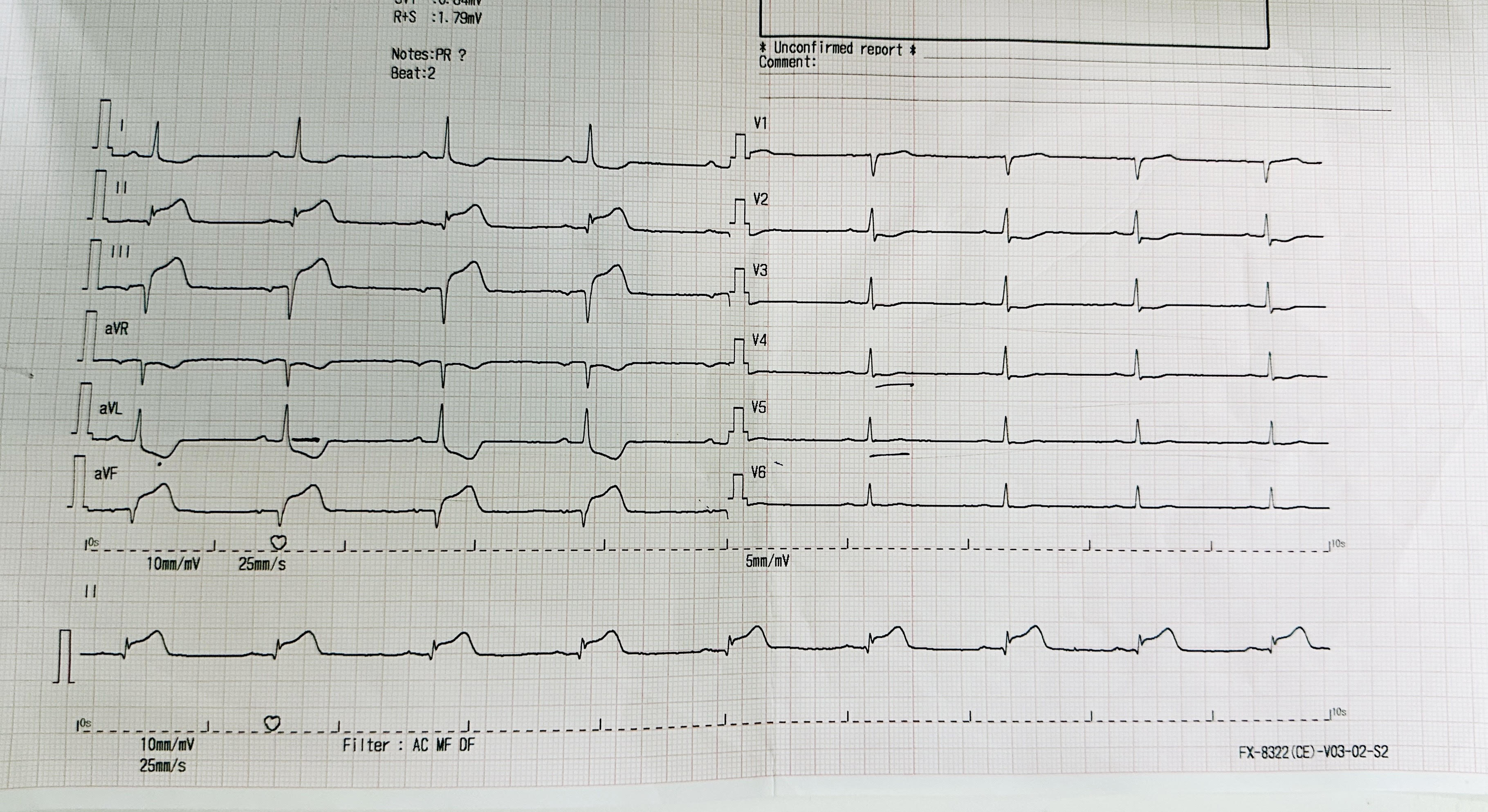
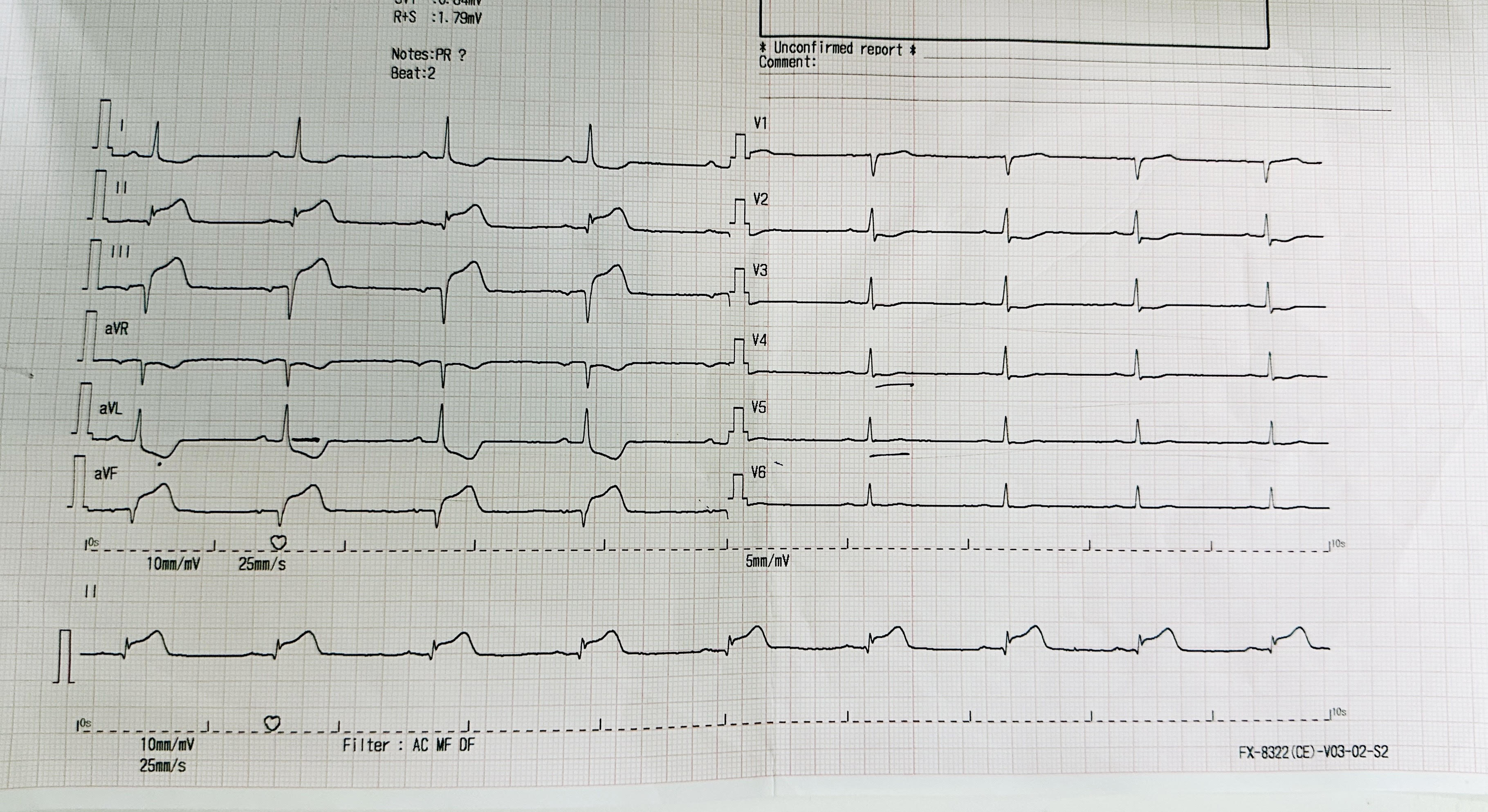
ECG showed Sinus Rhythm heart rate 58 bpm, ST elevation at lead II, III, aVF and Q wave in lead III, aVF and ST depression at lead I, aVL. Diagnosis of Acute ST Elevated Myocardial Infarction Inferior.Echocardiography (TTE) : Mid Inferior wall and Mid Posterior wall are severe Hypokinesia. No pericardial effusion. Primary PCI activated. Chest X ray normal.
Relevant Catheterization Findings
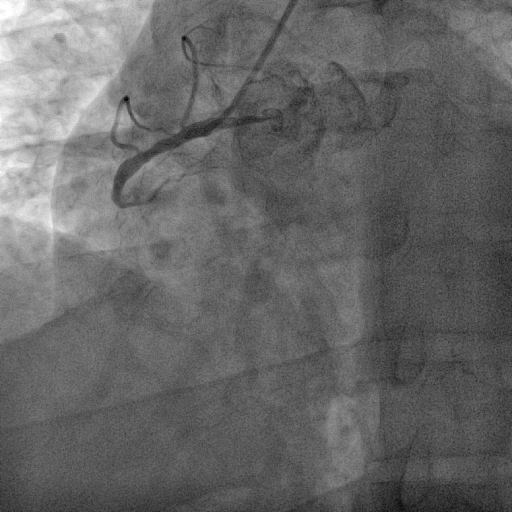
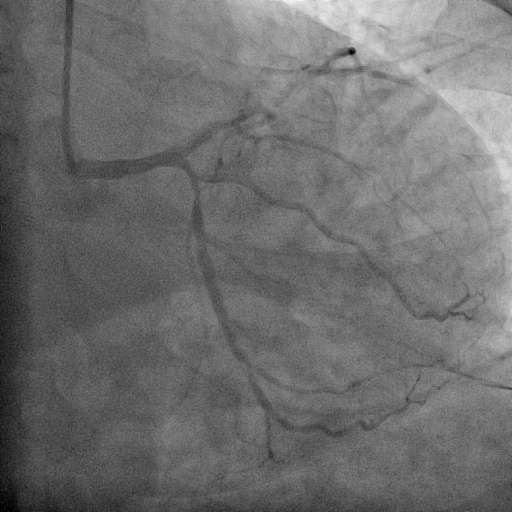
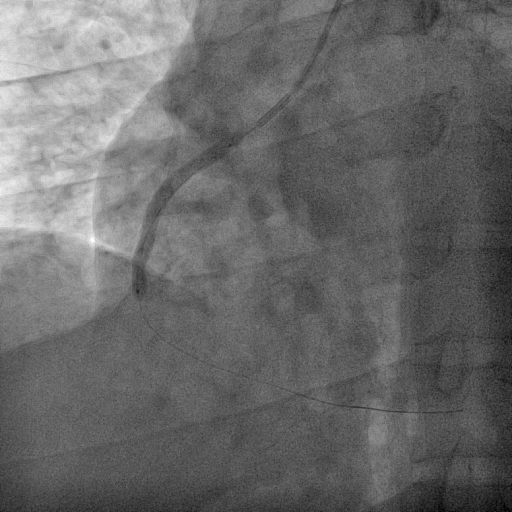
Coronary angiography was performed via right radial access with terumo radial TIG 5Fr catheter . Coronary artery angiogram revealed right dominance coronary artery system with RCA mid 100% with retrograde from LAD and LCx proximal 70%, distal 80% and LAD proximal 99% .
 SHAHIDUL ISLAM_(S7_F1-50).avi
SHAHIDUL ISLAM_(S7_F1-50).avi
SHAHIDUL ISLAM_(S2_F1-57).avi
SHAHIDUL ISLAM_(S6_F1-102).avi
Interventional Management
Procedural Step
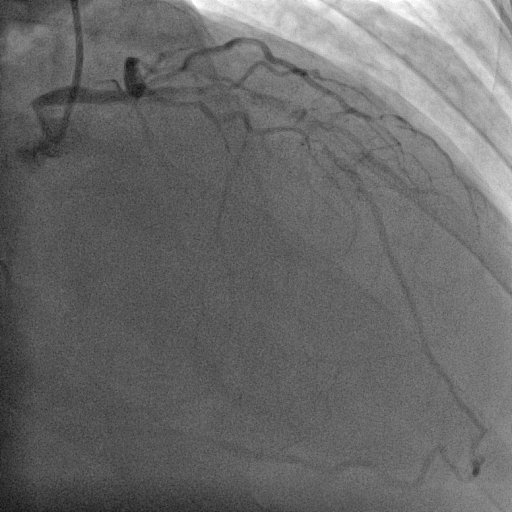
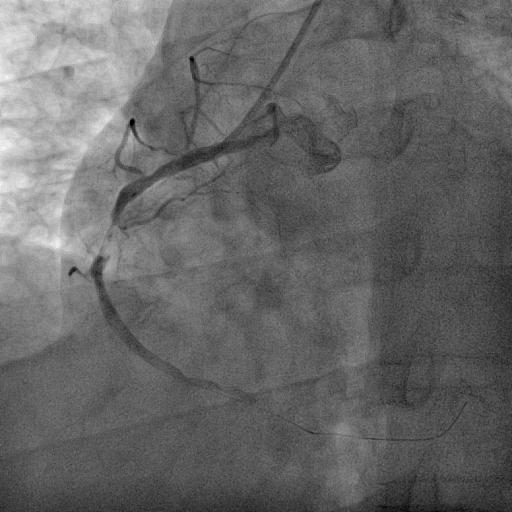
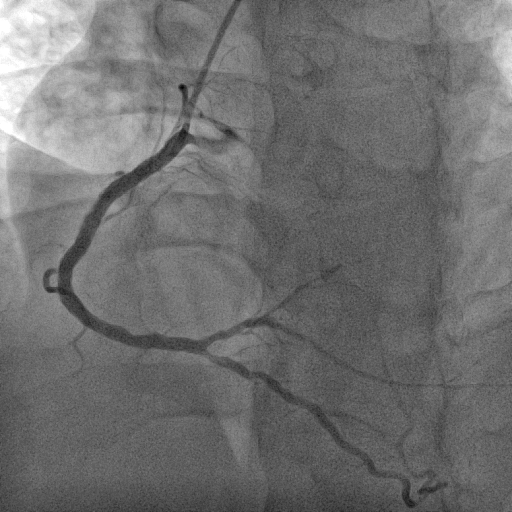
We decided to proceed with the primary percutaneous coronary angioplasty via right radial access by using the 5F JR 3.5 guiding catheter . We used Run through NS floppy wire for crossing culprit lesion to distal RCA but TIMI flow 0. We used micross 1.0 balloon for just cross the lesion and tracking balloon over the lesion . Then distal segment properly seen. Pre dilatation not done due to acute lesion and high chance of thrombus dislodgement and distal embolization . Direct stent 3.50 x 42 mm was implanted in proximal RCA to Mid RCA at 14 atmosphere pressure. Stent was well apposed and final result angiography was excellent and TIMI III flow without residual lesion and no distal embolization. the procedure done without any complications. Total Inj. heparin 10000 unit given and ACT was 298 sec.
SHAHIDUL ISLAM_(S8_F1-57).avi
SHAHIDUL ISLAM_(S12_F1-23).avi
SHAHIDUL ISLAM_(S14_F1-46).avi
Case Summary
Directing stenting may prevent distal embolization and TIMI Slow flow during primary Percutaneous coronary angioplasty specially thrombus containing culprit lesion in acute STEMI. This case reinforces the role of direct stenting in reducing distal embolization, promoting early vessel healing, achieving favorable long term outcomes. Results reflects the importance of meticulous procdural execution with use of appropriate stent .