Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251103_015
Save the Stent!
By Chun Lin Raymond Cheung
Presenter
Chun Lin Raymond Cheung
Authors
Chun Lin Raymond Cheung1
Affiliation
Tuen Mun Hospital, Hong Kong, China1
View Study Report
CASE20251103_015
Coronary - Complication Management
Save the Stent!
Chun Lin Raymond Cheung1
Tuen Mun Hospital, Hong Kong, China1
Clinical Information
Relevant Clinical History and Physical Exam
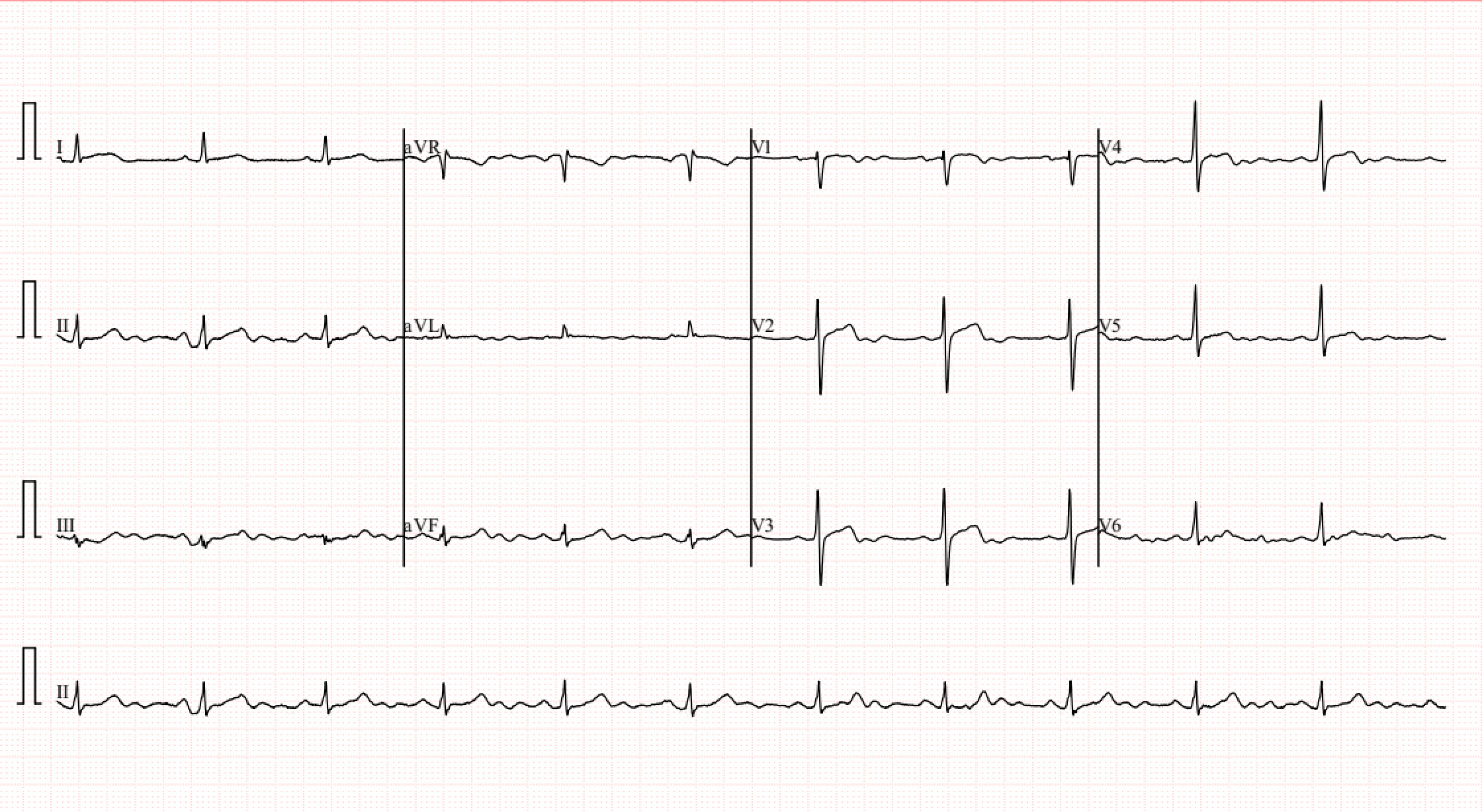
Mr Wai is a 66 year old man with history of ischemic heart disease. He presented to us for on and off non exertional chest discomfort.CT Coronary aniogram showed severe disease at proximal LAD.ECG showed sinus rhythmn with no acute ST changes.He was planned for elective coro/PCI.
Relevant Test Results Prior to Catheterization
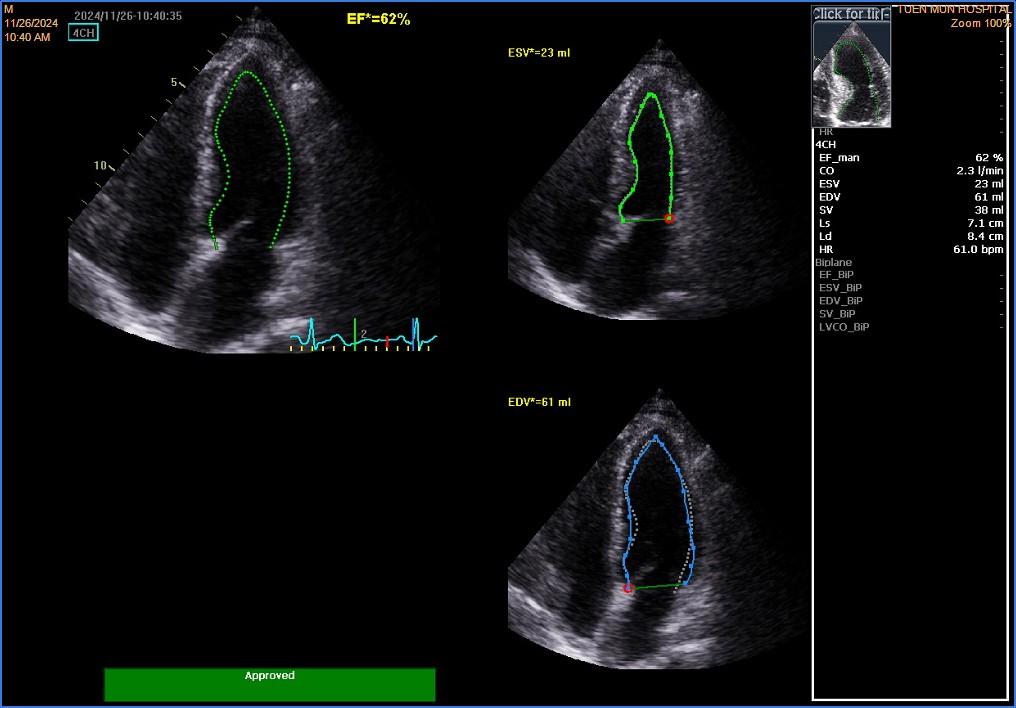
Blood tests were unremarkable. LDLc was 1.7mmol.L.A1c was 6.0. Echo showed normal LV systolic function, with LVEF 65%.Mild hypokinetic mid to apical anterior wall was noted.There was no pericardial effusion.
 4ch.avi
4ch.avi
sax.avi
lax1.avi
Relevant Catheterization Findings
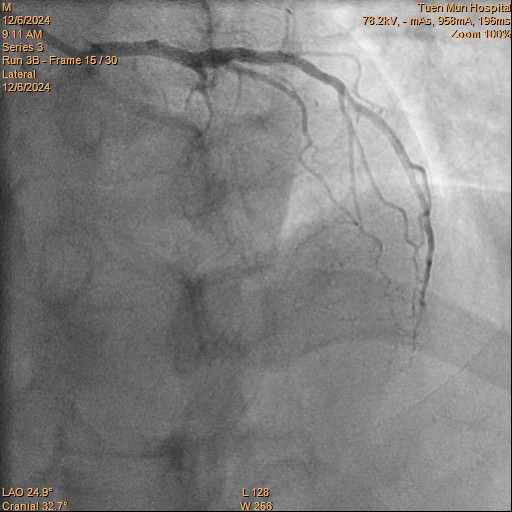
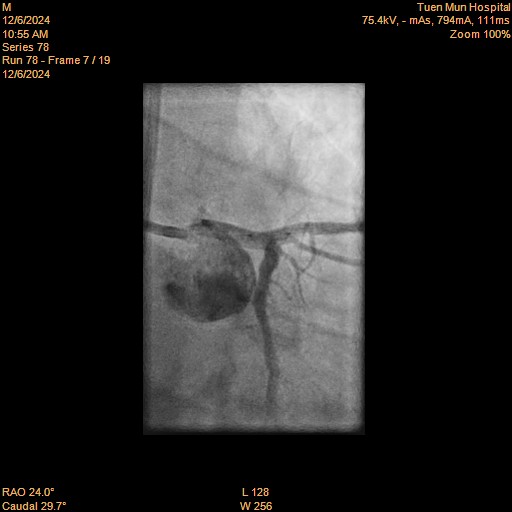
LMS: Normal LAD: Occluded from proximal segment onwards, receiving collaterals from right system LCX: Moderate disease distally RCA: Dominant. Minor disease
cranial.avi
caudal.avi
rca.avi
Interventional Management
Procedural Step
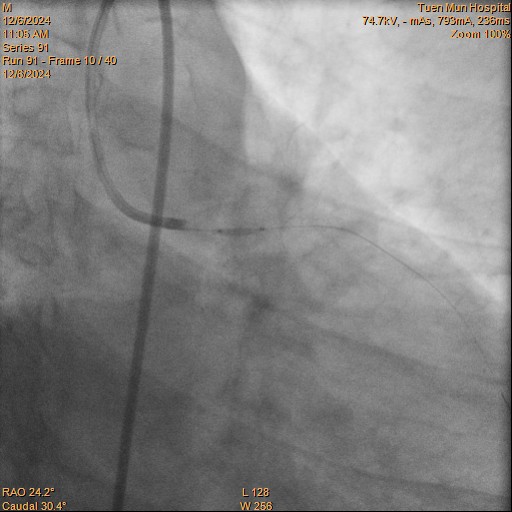
RFA approach.LMS engaged with EBU 3.5 7F.RCA engaged with with JR4 for contralateral injection via RRA.
pLAD wired with Gaia Next II with cosair Pro. Tried wiring mLAD but wire into subintimal space. Gaia Next III used for parallel wiring with crusade.
LAD dilated with 1.5 balloon.IVUS confirmed wire in true lumen.o-pLAD stented with Xience 2.5/26.IVUS showed stent protruded into LMS, decided for stenting to LMS.
Plan for Xience 3.5/8 into LM, but stent not long enough. So plan to switch for longer stent 3.5/12.But stent dislodged while being retrieved out.
So the 3.5/8 stent was serially dilated with 1.5, 2.25 & 3.0 NC with stent boost guidance. POT done at LMS with NC 4.0/6 at 22atm. oLAD dilated with stent balloon 3.5/8 at 14atm.
Final IVUS showed satisfactory landing zone, good apposition/ expansion and no significant stent edge.Final angiography showed satisfactory result and TIMI 3 flow.
final.avi
pLAD stent.avi
ladcrossed.avi
pLAD wired with Gaia Next II with cosair Pro. Tried wiring mLAD but wire into subintimal space. Gaia Next III used for parallel wiring with crusade.
LAD dilated with 1.5 balloon.IVUS confirmed wire in true lumen.o-pLAD stented with Xience 2.5/26.IVUS showed stent protruded into LMS, decided for stenting to LMS.
Plan for Xience 3.5/8 into LM, but stent not long enough. So plan to switch for longer stent 3.5/12.But stent dislodged while being retrieved out.
So the 3.5/8 stent was serially dilated with 1.5, 2.25 & 3.0 NC with stent boost guidance. POT done at LMS with NC 4.0/6 at 22atm. oLAD dilated with stent balloon 3.5/8 at 14atm.
Final IVUS showed satisfactory landing zone, good apposition/ expansion and no significant stent edge.Final angiography showed satisfactory result and TIMI 3 flow.
Case Summary
In summary, this is a challenging LAD CTO case, which required parallel wiring from subintimal space. True lumen was confirmed with contralateral injection and IVUS.
While planned for LMS stenting, the stent used was too short. While the stent was retrieved for a longer stent, the stent was dislodged.The stent balloon was removed and the stent stayed at the same place inside LMS. So the stent was kept and serially dilated with from 1.5 up to 4.0 NC balloon. Final IVUS and angioraphic result were satisfactory out of our expectation despite we planned to use a longer stent.
While planned for LMS stenting, the stent used was too short. While the stent was retrieved for a longer stent, the stent was dislodged.The stent balloon was removed and the stent stayed at the same place inside LMS. So the stent was kept and serially dilated with from 1.5 up to 4.0 NC balloon. Final IVUS and angioraphic result were satisfactory out of our expectation despite we planned to use a longer stent.