Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251103_013
A Guiding Catheter Thrombectomy: A Salvage Technique for Massive Thrombus Burden in STEMI
By Ruth Grace Aurora, Arwin Saleh Mangkuanom, Nanda Iryuza, Amir Aziz Alkatiri, Doni Firman
Presenter
Ruth Grace Aurora
Authors
Ruth Grace Aurora1, Arwin Saleh Mangkuanom1, Nanda Iryuza1, Amir Aziz Alkatiri1, Doni Firman1
Affiliation
Department of Cardiology and Vascular Medicine, Faculty of Medicine Universitas Indonesia - National, Indonesia1
View Study Report
CASE20251103_013
Coronary - ACS/AMI
A Guiding Catheter Thrombectomy: A Salvage Technique for Massive Thrombus Burden in STEMI
Ruth Grace Aurora1, Arwin Saleh Mangkuanom1, Nanda Iryuza1, Amir Aziz Alkatiri1, Doni Firman1
Department of Cardiology and Vascular Medicine, Faculty of Medicine Universitas Indonesia - National, Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
An 81-year-old woman with a history of CTEPH (stable, on therapy) presented with 7 hours of shortness of breath and diaphoresis. On arrival, her hemodynamic profile was consistent with cardiogenic shock, requiring emergent endotracheal intubation and mechanical ventilation.
Relevant Test Results Prior to Catheterization
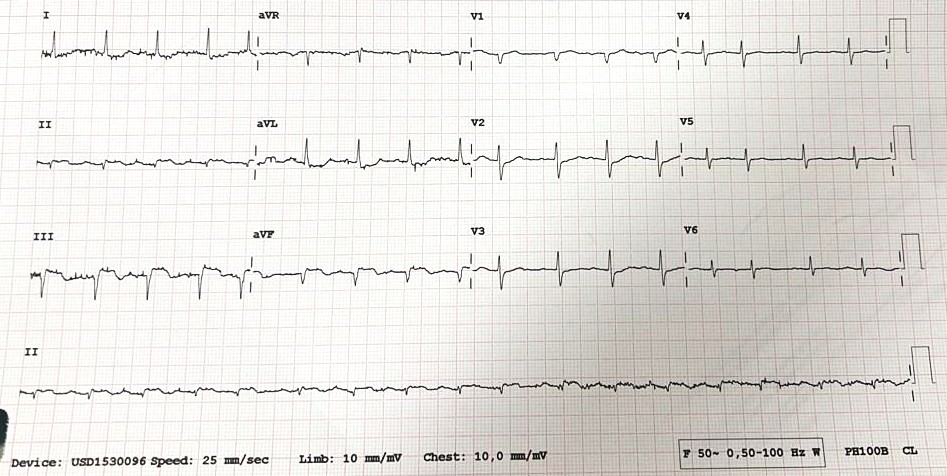
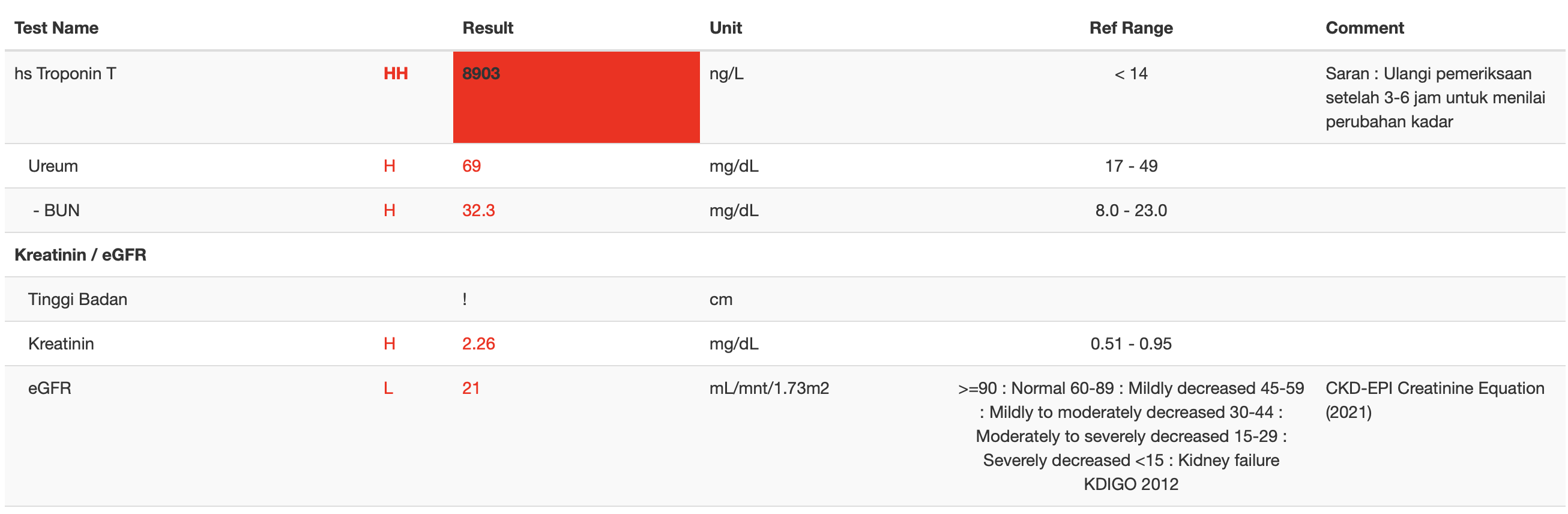
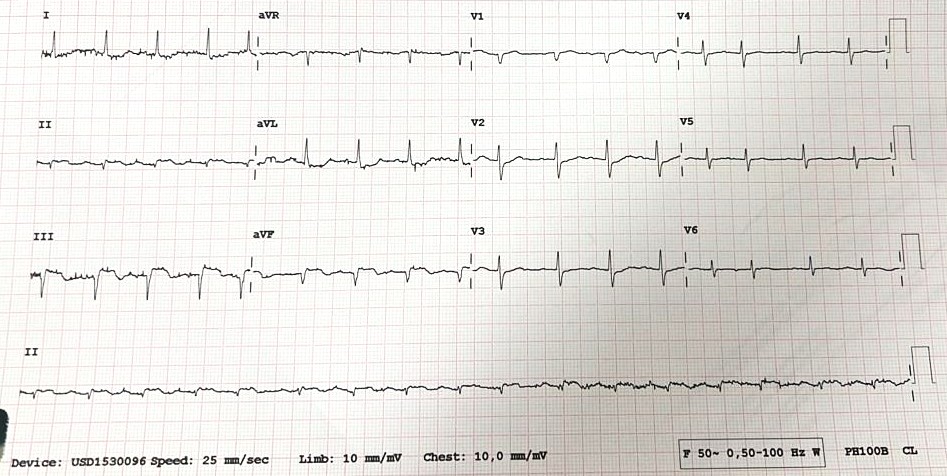
ST-segment elevation in the inferior leads, consistent with acute inferior STEMI. Marked elevation of troponin T and impaired renal function present
Relevant Catheterization Findings
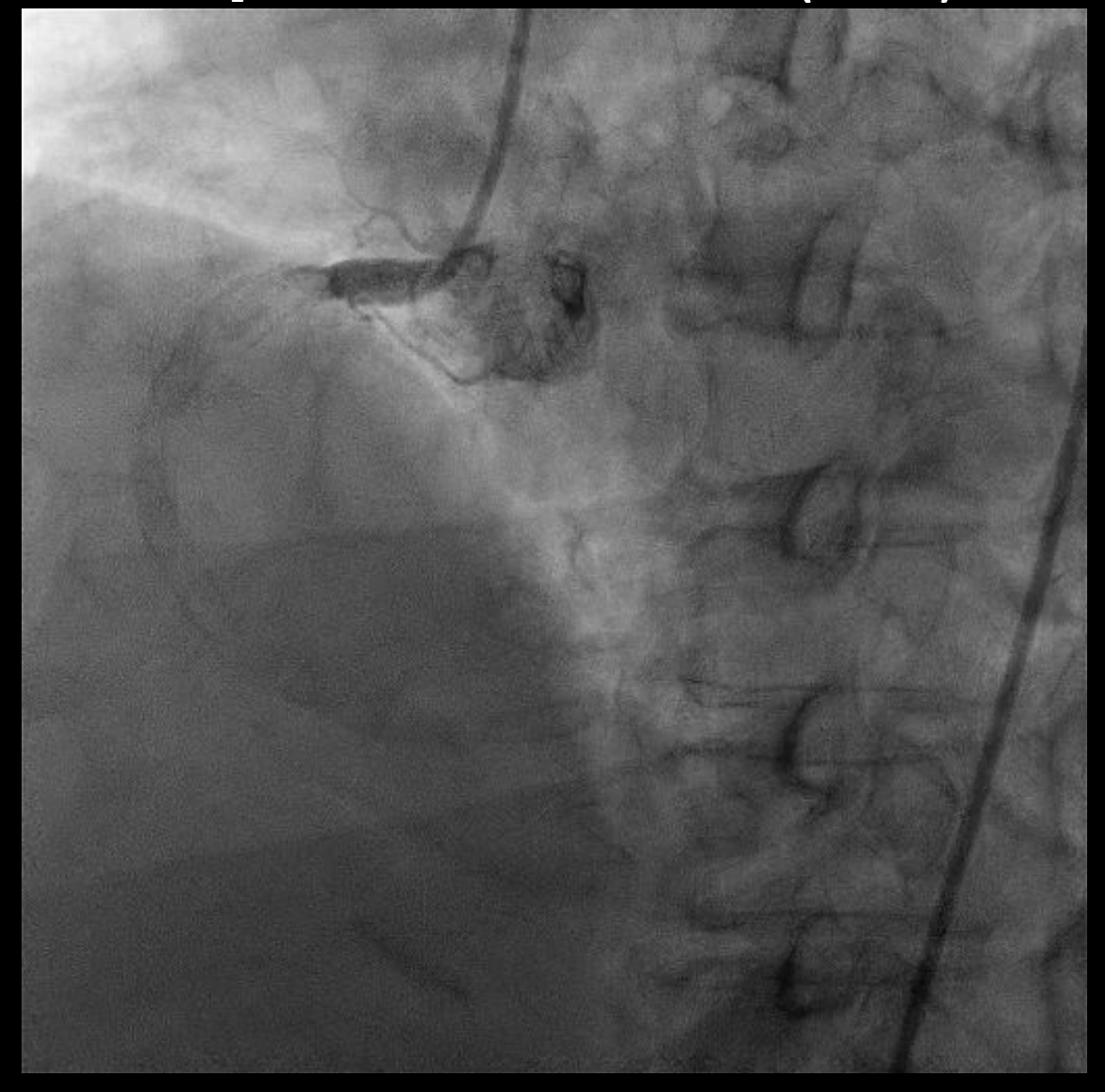
Dominant RCA with heavy calcification, total occlusion at RCA due to extending thrombus from the proximal to the distal segment of the RCA (TIMI grade 0 flow). LM and LCx were normal. LAD was normal except for myocardial bridging at its mid portion.
 angio-1.mov
angio-1.mov
angio-2.mov
angio-4.mov
Interventional Management
Procedural Step
Via transfemoral access, initial attempts to advance a guidewire to the distal vessel were unsuccessful. To facilitate better guiding support, an anchor-wire technique was employed by placing a guidewire in a RV branch. Subsequently, a guidewire was successfully advanced across the occlusion into the PDA. Initial pre-dilatation was performed sequentially with 1.5 mm and 2.0 mm SC balloons. Subsequently, the intervention was escalated using larger 2.5 mm to 3.0 mm NC balloons to dilate the segment from the proximal to the distal RCA.Following two unsuccessful conventional thrombus aspirations, TIMI 0 flow and Grade V thrombus burden persisted despite intracoronary epinephrine administration at distal RCA via thrombo-suction catheter. The patient developed profound hemodynamic instability (BP 60/49 mmHg) refractory to vasopressor support. We therefore decided to rapidly employ the guiding catheter (BL 3.5/5F) as a large-bore aspiration device despite the inherent risk of vessel injury. The catheter was advanced with the support of an anchor balloon. The guiding catheter was connected to a 3-way manifold and a balloon inflation device. Using negative pressure, it was advanced to the distal RCA for direct thrombus aspiration. This maneuver was repeated once, achieving successful thrombus extraction.Following thrombus removal, the vessel was prepared with a 3.0 mm NC balloon. A 4.0 × 24 mm drug-eluting stent was then implanted in the mid RCA.

BL:5F - as a large-bore aspiration device.mov
Case Summary
We present a case of inferior STEMI with high thrombus burden with total RCA occlusion identified as the culprit lesion. Following catheter-guided thrombectomy using a BL 3.5/5 F catheter, the patient achieved complete revascularization and significant improvement in RCA flow. The target vessel reached optimal stent expansion with restoration of TIMI grade 3 flow and no complications.