Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251103_007
When the Rock Strikes Back: Catastrophic Left Main Dissection Following Rotablation in a Heavily Calcified Bifurcation
By Rido Adrianto Sukaton, Amir Aziz Alkatiri, Arwin Saleh Mangkuanom, Doni Firman
Presenter
Rido Adrianto Sukaton
Authors
Rido Adrianto Sukaton1, Amir Aziz Alkatiri1, Arwin Saleh Mangkuanom1, Doni Firman1
Affiliation
National Cardiovascular Center Harapan Kita, Indonesia1
View Study Report
CASE20251103_007
Coronary - Complex PCI - Left Main
When the Rock Strikes Back: Catastrophic Left Main Dissection Following Rotablation in a Heavily Calcified Bifurcation
Rido Adrianto Sukaton1, Amir Aziz Alkatiri1, Arwin Saleh Mangkuanom1, Doni Firman1
National Cardiovascular Center Harapan Kita, Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
A 59-year-old female presented with angina pectoris during daily activities. Risk factors included hypertension, dyslipidemia, and type 2 diabetes. Physical examination findings were within normal limits.

Relevant Test Results Prior to Catheterization
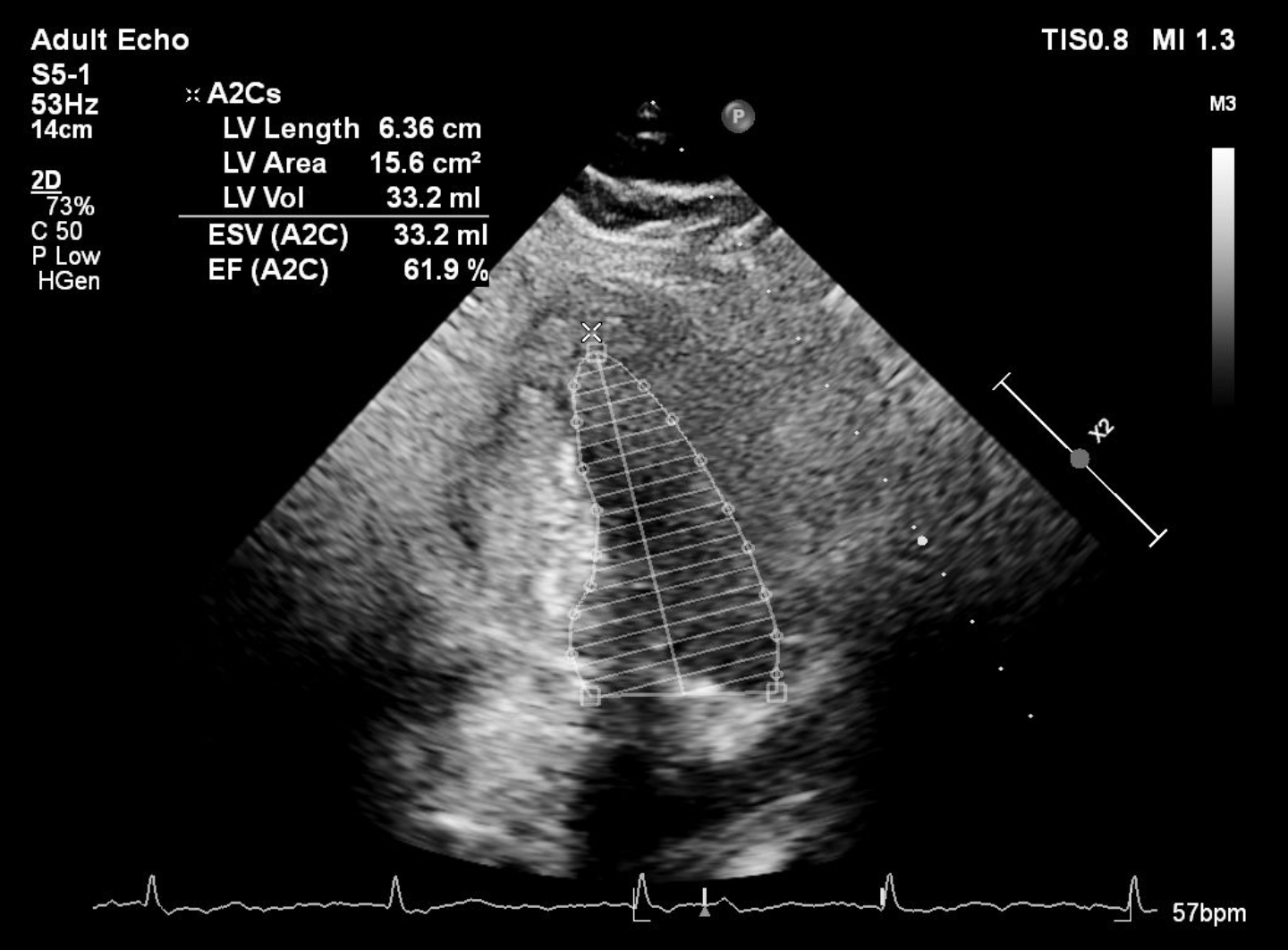
Resting ECG was normal. Referring hospital’s treadmill test showed positive ischemic response with high-risk Duke score. Echocardiography showed preserved ejection fraction.

Relevant Catheterization Findings
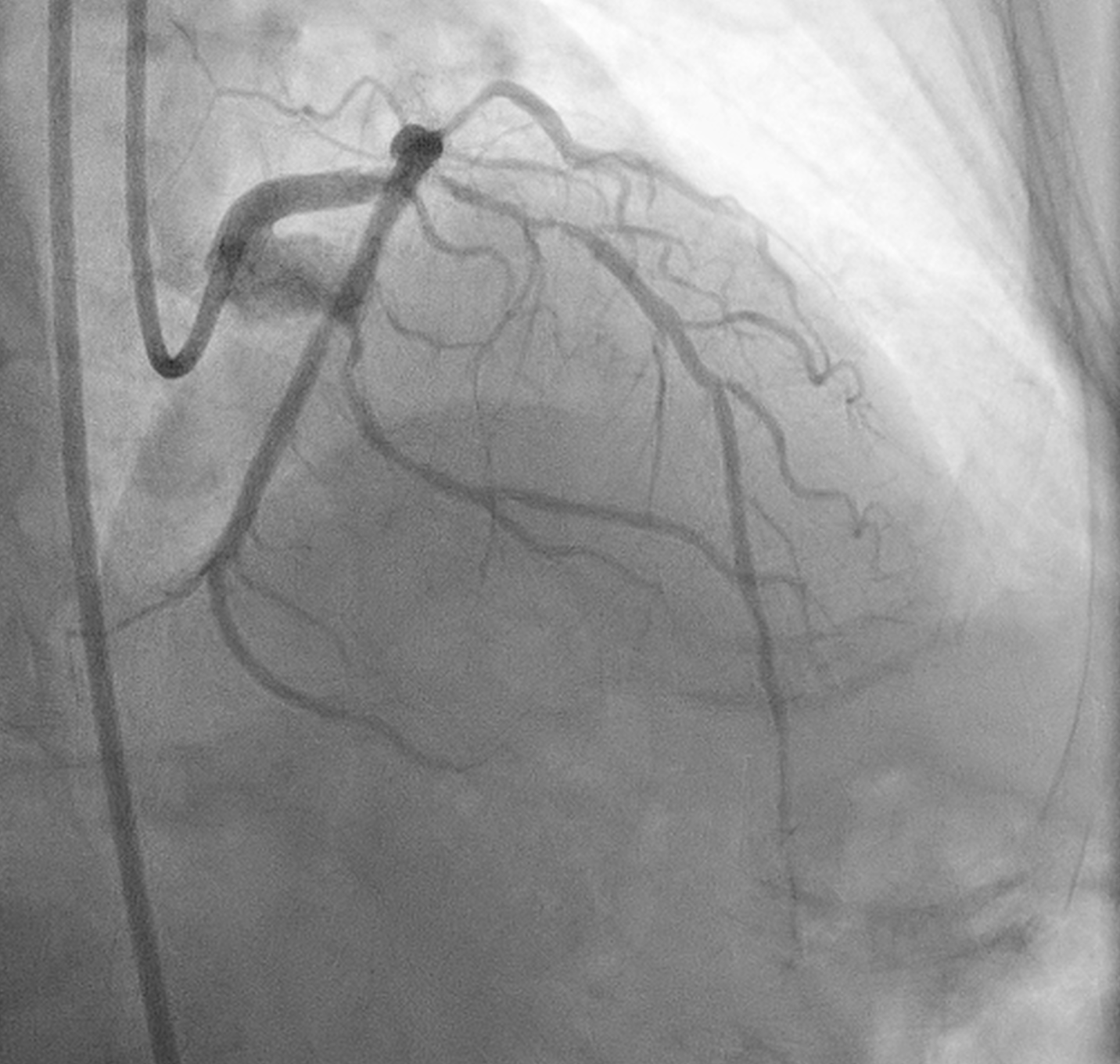
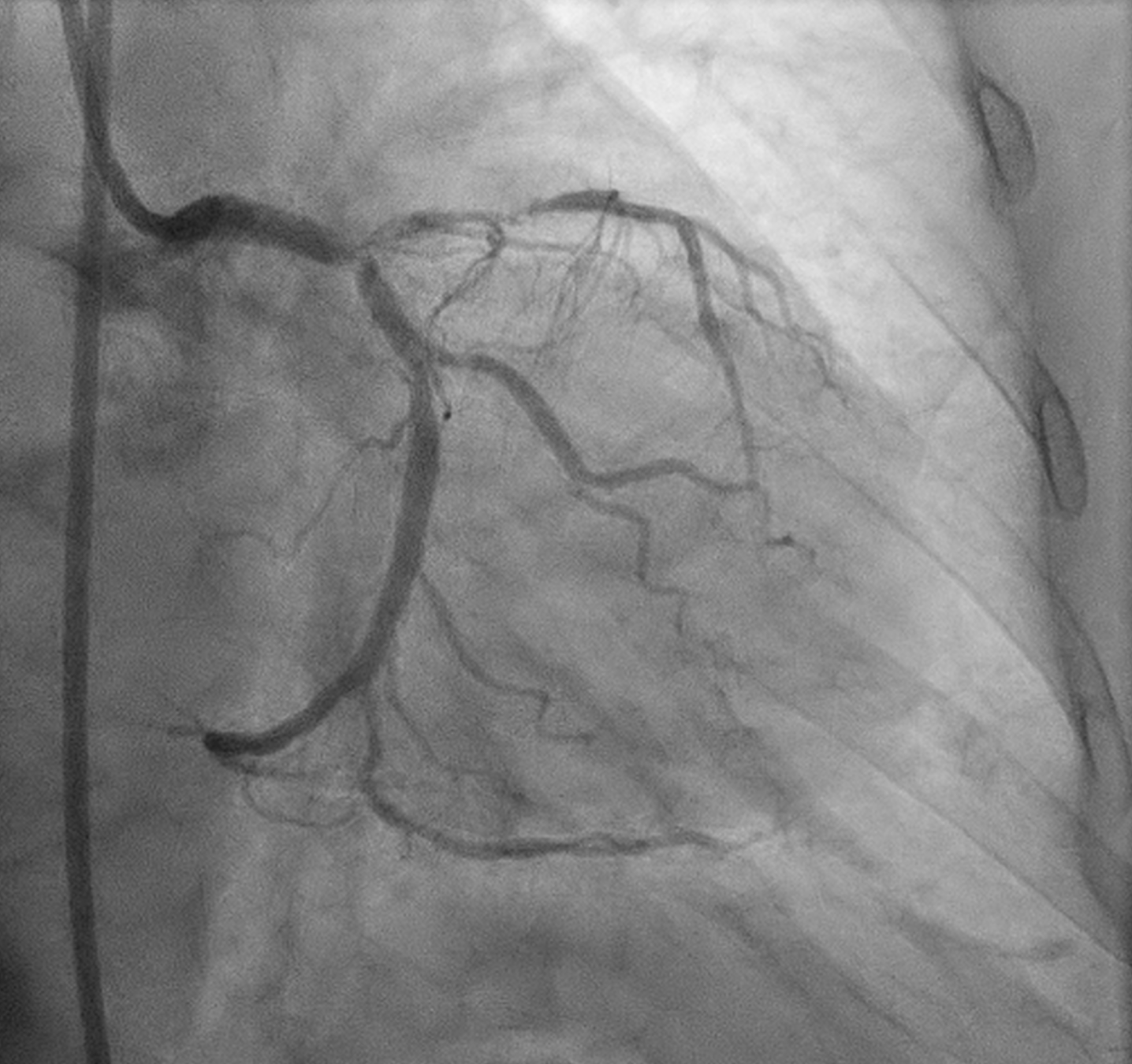
Angiography showed small non-dominant RCA with proximal severe stenosis, Left Main with severe tubular calcified stenosis at distal segmen, bifurcation lesion (medina1-1-1), LAD with diffuse calcified subtotal stenosis from ostial–mid, and LCX iwth severe tubular calcified stenosis at ostial.

 Screen Recording 2025-11-03 at 18.53.50.mov
Screen Recording 2025-11-03 at 18.53.50.mov
Screen Recording 2025-11-03 at 18.53.06.mov
Screen Recording 2025-11-03 at 18.52.45.mov
Interventional Management
Procedural Step
Procedure was done via Right femoral artery using 7F sheath (later exchanged for a 7F long sheath due to vessel tortuosity). The left coronary artery was cannulated using a 7F EBU 3.5 guiding catheter.
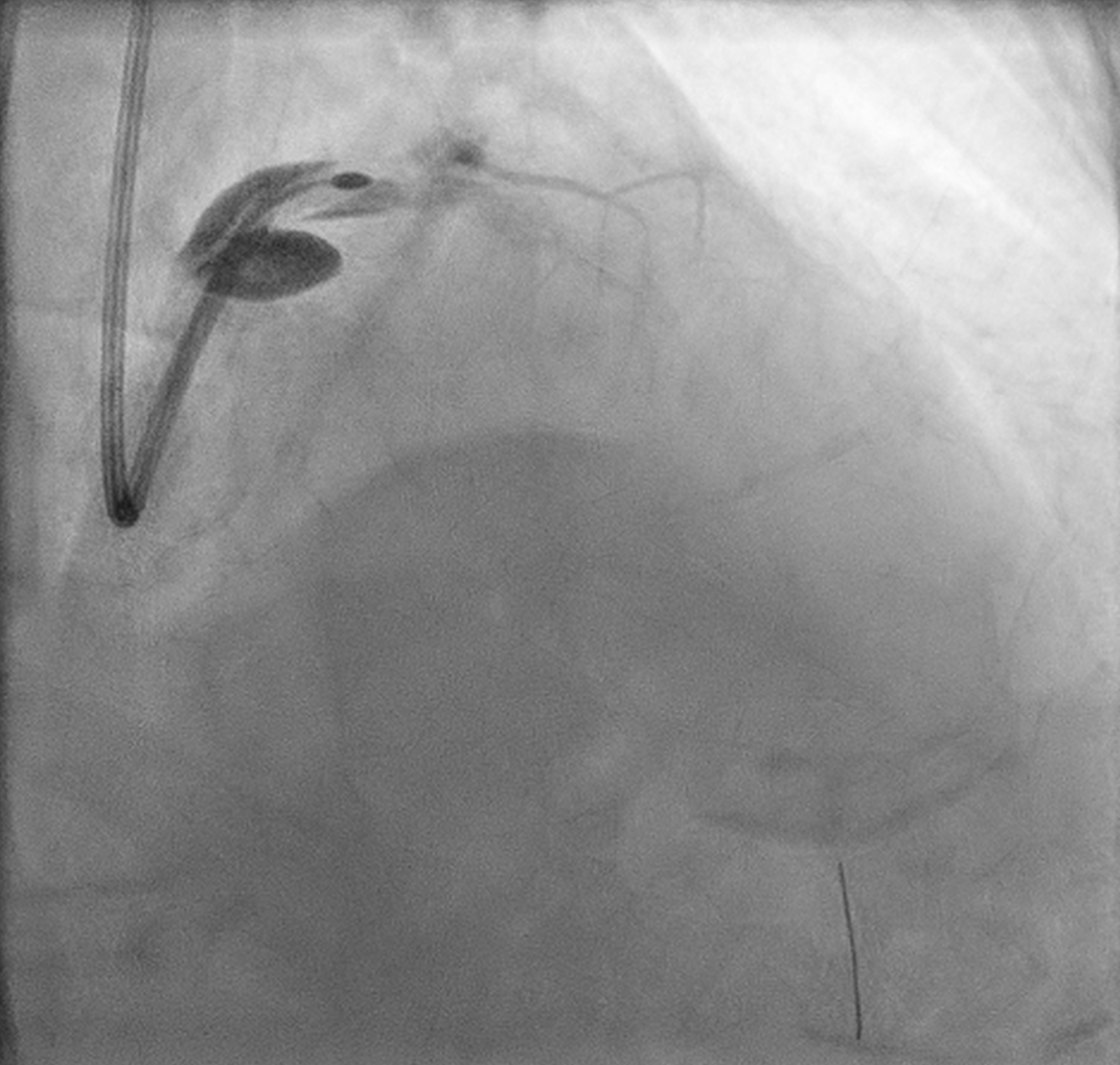
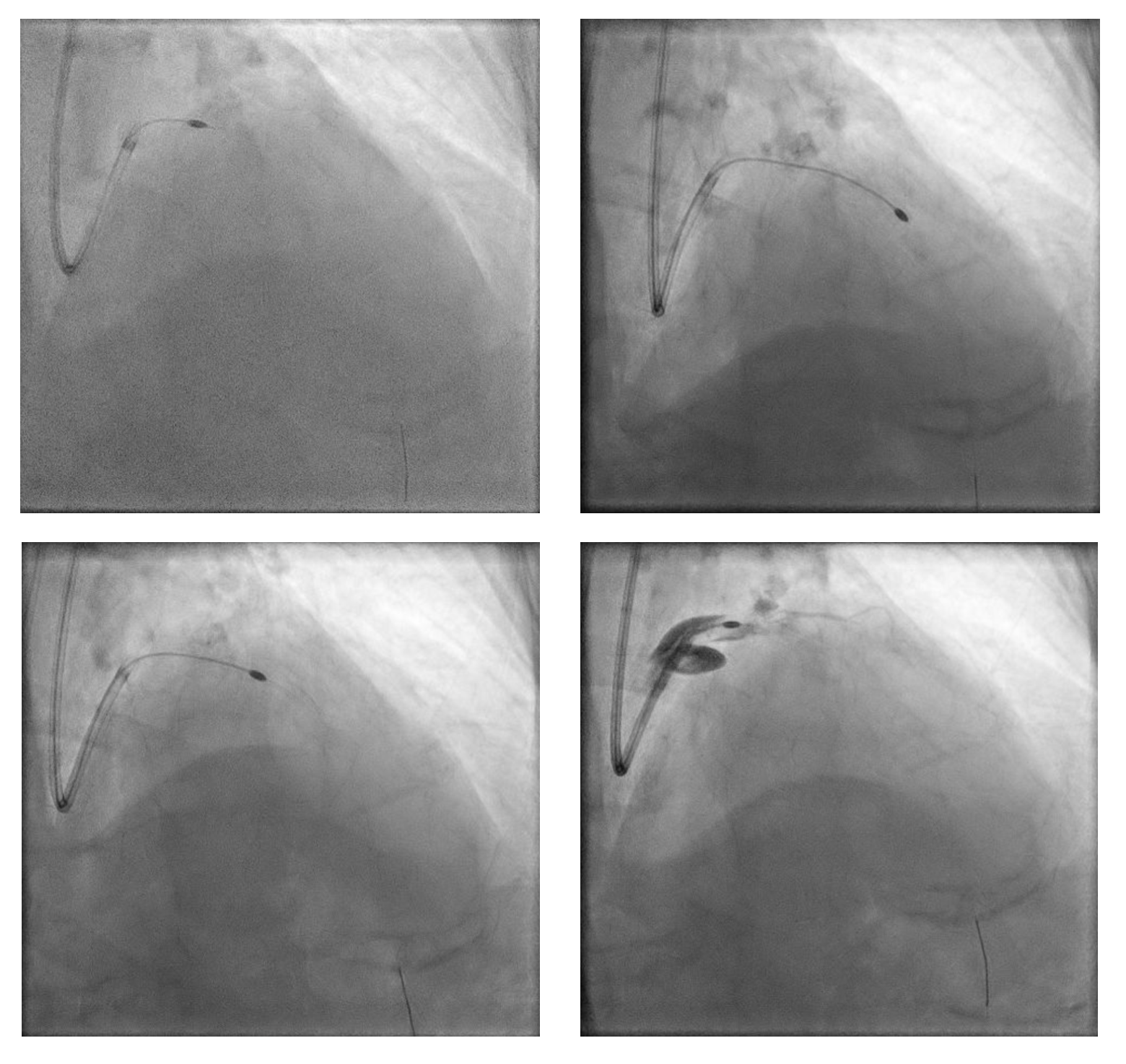
PCI was initiated with Full Dose Heparin. LAD wired with Runthrough NS Floppy; predilatation with 2.0 × 15 mm SC balloon. IVUS failed to cross proximal LAD, showing nodular calcium. Rotational atherectomy was performed using Rotapro 1.75 mm burr (180,000 rpm, four runs) followed by one polishing run at 150,000 rpm. Chest pain and ST elevation occurred shortly after rotablation due to Type F dissection in distal LM (TIMI 0 LAD). Bailout stenting with Promus Premier 3.5 × 38 mm from LM–LAD was performed using jailed-balloon technique, followed by post-dilatation and IVUS optimization.
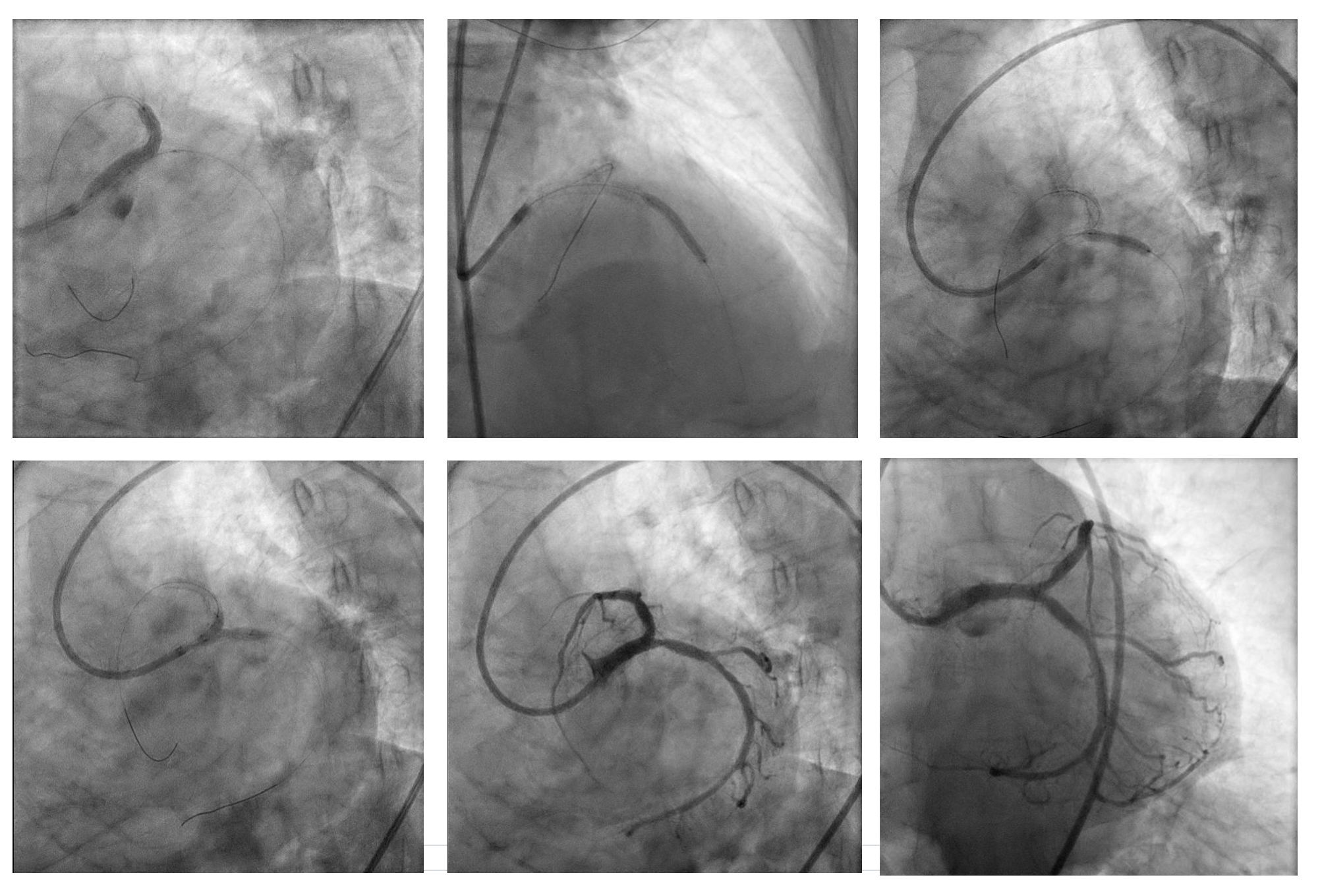
A second stent (Promus Premier 2.75 × 24 mm) was implanted in proximal–mid LAD overlaping with previous stent, then high-pressure post-dilatation and POT (NC 4.5×8 mm) was performed. LCx was rewired and treated with TAP stenting (Promus Premier 3.5 × 18 mm) after sequential and final kissing balloon dilatations. Post-IVUS confirmed well-expanded and well-apposed stents (MSA LAD 5.22 mm²; LCx 7.82 mm²).
Final angiogram showed TIMI 3 flow with no residual dissection. Procedure duration 30:52 min; contrast 180 mL; DAP 117.05 Gy·cm².
Screen Recording 2025-11-03 at 19.23.09.mov
Screen Recording 2025-11-03 at 19.25.10.mov
Screen Recording 2025-11-03 at 19.25.51.mov
PCI was initiated with Full Dose Heparin. LAD wired with Runthrough NS Floppy; predilatation with 2.0 × 15 mm SC balloon. IVUS failed to cross proximal LAD, showing nodular calcium. Rotational atherectomy was performed using Rotapro 1.75 mm burr (180,000 rpm, four runs) followed by one polishing run at 150,000 rpm. Chest pain and ST elevation occurred shortly after rotablation due to Type F dissection in distal LM (TIMI 0 LAD). Bailout stenting with Promus Premier 3.5 × 38 mm from LM–LAD was performed using jailed-balloon technique, followed by post-dilatation and IVUS optimization.
A second stent (Promus Premier 2.75 × 24 mm) was implanted in proximal–mid LAD overlaping with previous stent, then high-pressure post-dilatation and POT (NC 4.5×8 mm) was performed. LCx was rewired and treated with TAP stenting (Promus Premier 3.5 × 18 mm) after sequential and final kissing balloon dilatations. Post-IVUS confirmed well-expanded and well-apposed stents (MSA LAD 5.22 mm²; LCx 7.82 mm²).
Final angiogram showed TIMI 3 flow with no residual dissection. Procedure duration 30:52 min; contrast 180 mL; DAP 117.05 Gy·cm².
Case Summary
Successful complex PCI of calcified LM bifurcation (Medina 1-1-1) in a 63-year-old woman with 3-vessel disease. Catastrophic Type F LM dissection occurred after rotablation run, promptly managed with bailout LM-LAD stenting and TAP stenting of LCx under IVUS guidance. Final IVUS showed well-expanded, well-apposed stents with restored TIMI 3 flow, highlighting the importance of prompt recognition, imaging guidance, and structured bailout strategy in high-risk rotablation cases.