Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251103_004
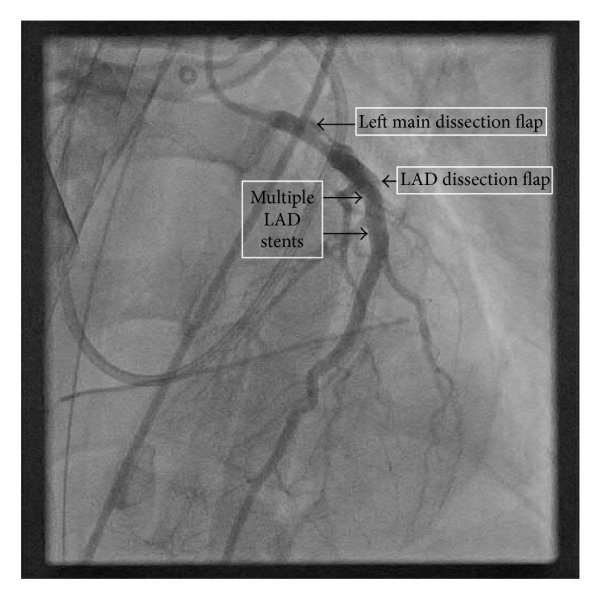
When Diagnosis Turns Into Emergency: Left Main Dissection Rescued by Two-Stent Technique
By Chanikarn Kanaderm
Presenter
Chanikarn Kanaderm
Authors
Chanikarn Kanaderm1
Affiliation
Central Chest Institute of Thailand, Thailand1
View Study Report
CASE20251103_004
Coronary - Complication Management
When Diagnosis Turns Into Emergency: Left Main Dissection Rescued by Two-Stent Technique
Chanikarn Kanaderm1
Central Chest Institute of Thailand, Thailand1
Clinical Information
Relevant Clinical History and Physical Exam
A59-year-old woman is referred for pre-operative coronary evaluation prior toplanned mitral valve replacement for symptomatic severe mitral regurgitation. Pastmedical history includes she denies coronary artery disease risk. On examination Cardiac exam reveals alaterally displaced, dynamic PMI and a grade 3/6 high-pitched holosystolicmurmur best heard at the apex with radiation to the left axilla.
Relevant Test Results Prior to Catheterization
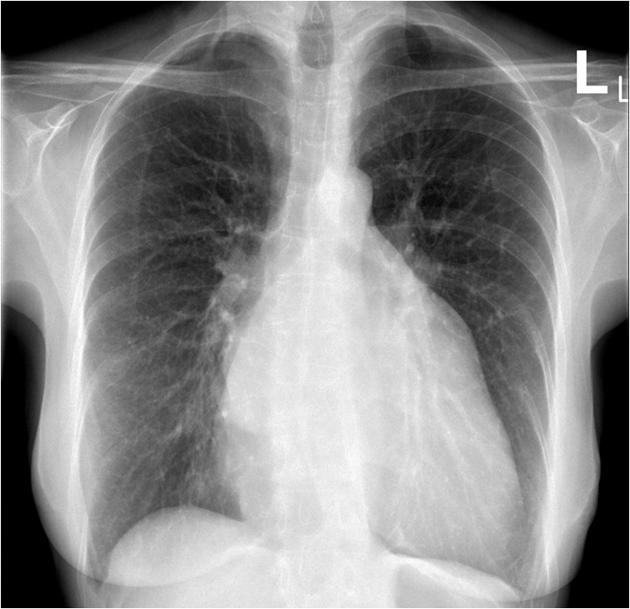
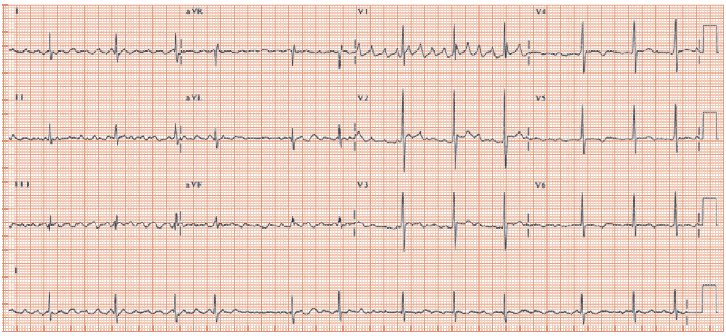
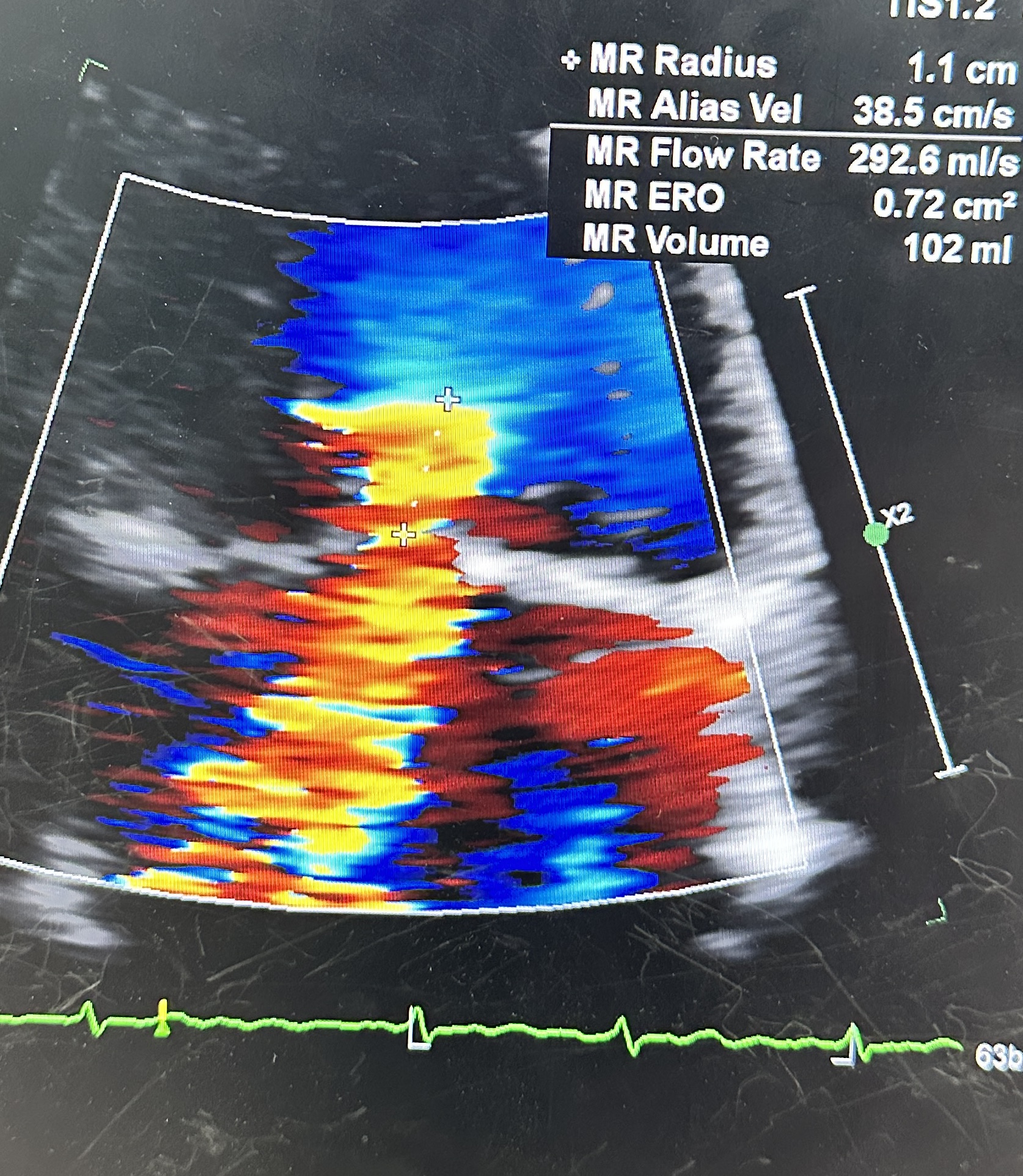
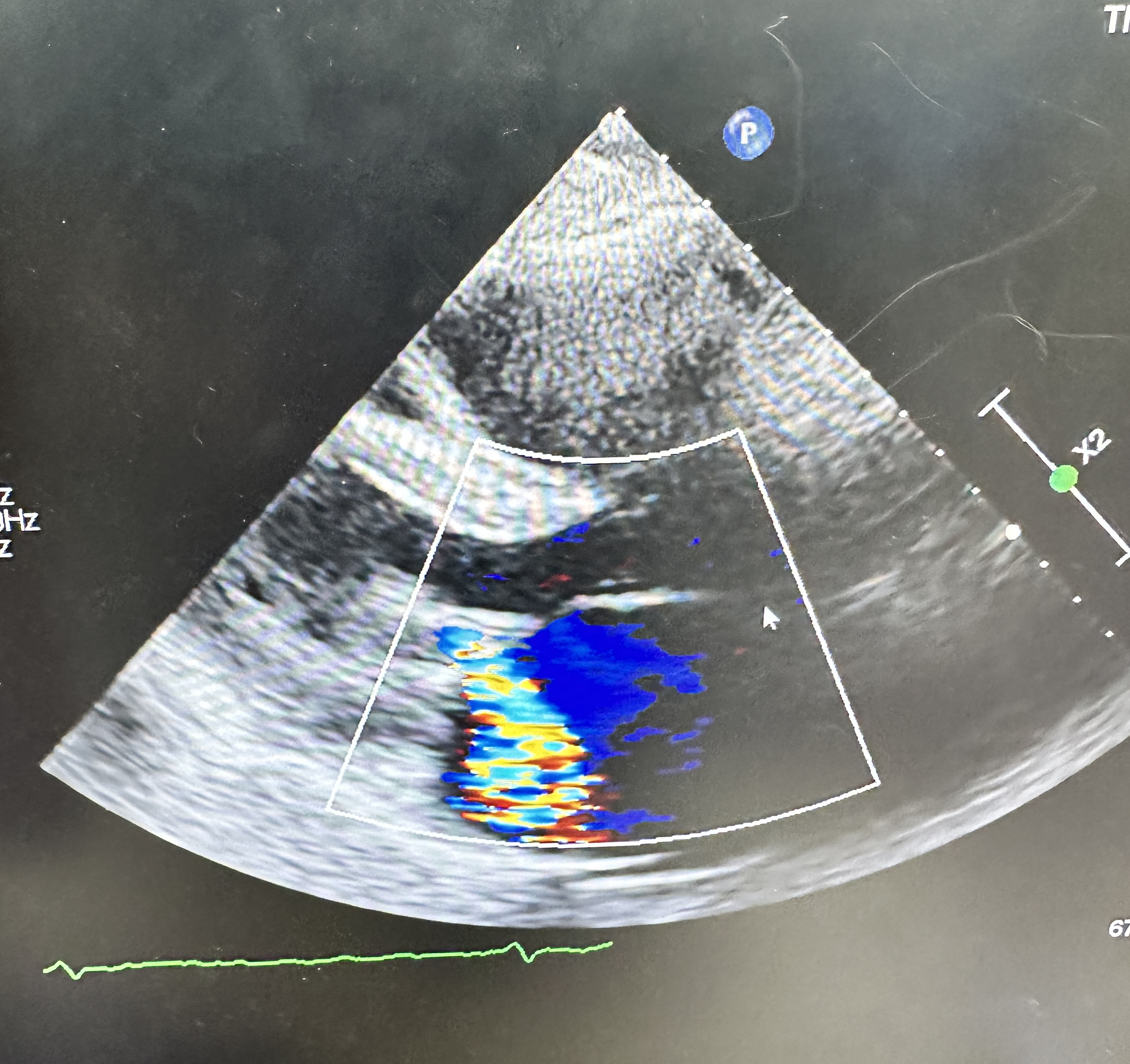
ECG: AF without acute ischemic change.CXR:CardiomegalyEchocardiogram: Severe primary (degenerative) mitral regurgitation due to mitral valve prolapses with flail P2 segment (Carpentier Type II), by integrative criteria (EROA ≥0.4 cm²,regurgitant volume ≥60 mL, vena contracta ≥0.7 cm, systolic PV flow reversal,dense triangular CW jet). Baseline ECG: sinus rhythm without acuteischemic change.
Relevant Catheterization Findings
Right Coronary Artery (RCA): Dominance right. Large caliber, no significant stenosis. Angiographically normal with TIMI 3 flow.

 IMG_8942.mov
IMG_8942.mov
Interventional Management
Procedural Step
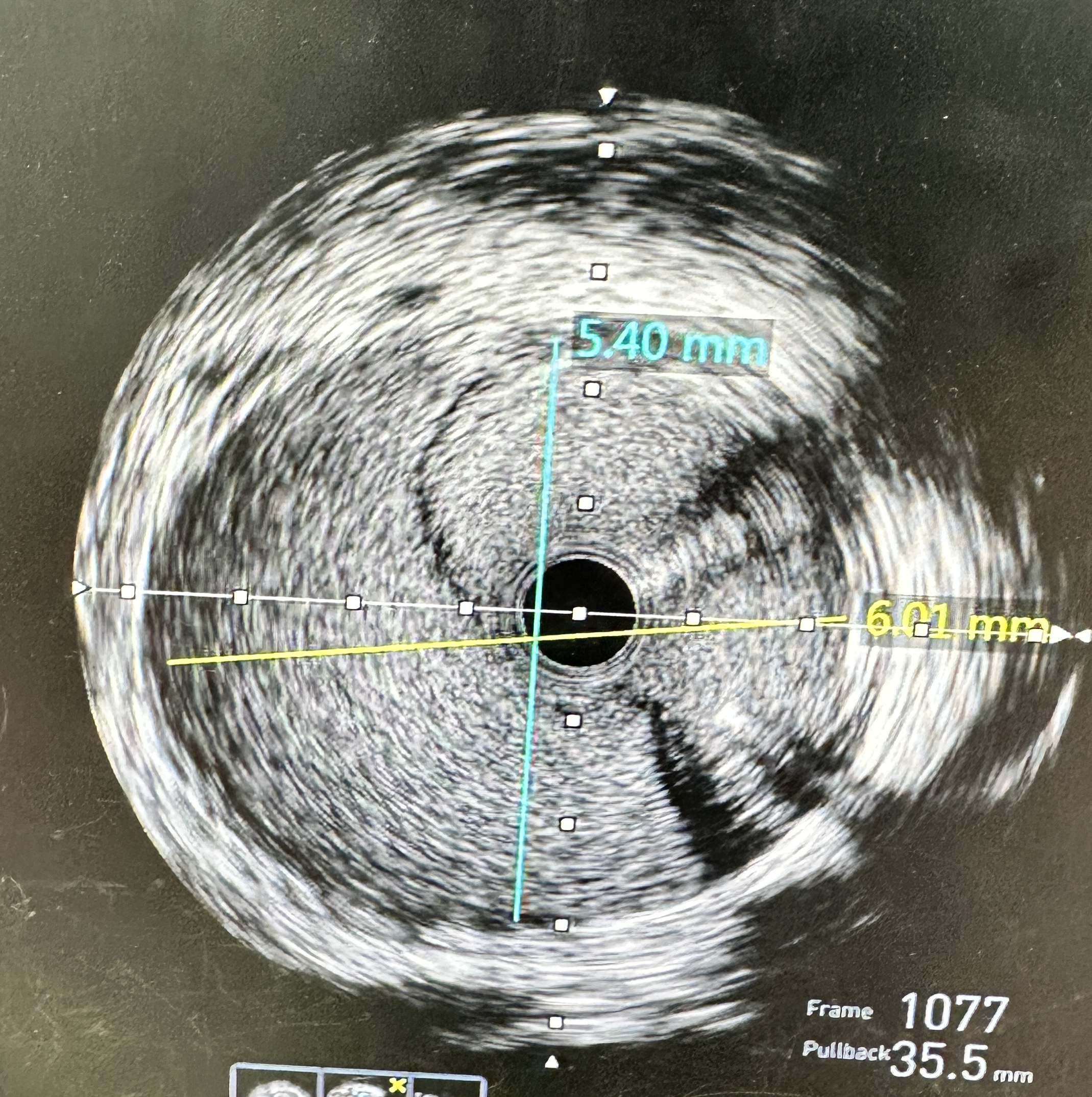
- Actions: Stopped contrast injections; converted to RFA for stronger guide backup. Wired LAD and LCX in true lumen (confirmed by IVUS).
- Stenting: LM → LAD drug-eluting stent (DES) to seal LM entry; mini-TAP to LCX for ostial coverage.
- Imaging: IVUS pre-PCI confirmed dissection/intimal flap with intramural hematoma extending into proximal LAD/LCX; post-PCI showed good expansion/apposition, no residual entry.
- Final result: TIMI 3 flow in LAD and LCX; LM sealed; no residual flow-limiting dissection.