Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251103_003
CHIP PCI for a Patient With HFrEF and Three-Vessel Disease Declined for Surgery
By Cheng-De Chang Chien, Chun-Yuan CHU
Presenter
Cheng-De Chang Chien
Authors
Cheng-De Chang Chien1, Chun-Yuan CHU2
Affiliation
Kaohsiung Medical University Hospital, Taiwan1, Kaohsiung Medical University Hospital, Taiwan2
View Study Report
CASE20251103_003
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
CHIP PCI for a Patient With HFrEF and Three-Vessel Disease Declined for Surgery
Cheng-De Chang Chien1, Chun-Yuan CHU2
Kaohsiung Medical University Hospital, Taiwan1, Kaohsiung Medical University Hospital, Taiwan2
Clinical Information
Relevant Clinical History and Physical Exam
54-year-old man, active smoker with history of heart failure with reduced ejection fraction (30%), Type 2 diabetes mellitus, Systemic Sclerosis, and dyslipidemia, ESRD. He presented persistent shortness of breath after walking long distances, edema in both lower legs and visited the emergency department for help. Initial vital signs showed BT: 35.8 ℃; HR: 99 bpm; RR: 18 cpm; BP: 129/79 mmHg; SpO2: 96 %. Physical examination showed bilateral basal crackle sounds and bilateral pitting edema .


Relevant Test Results Prior to Catheterization
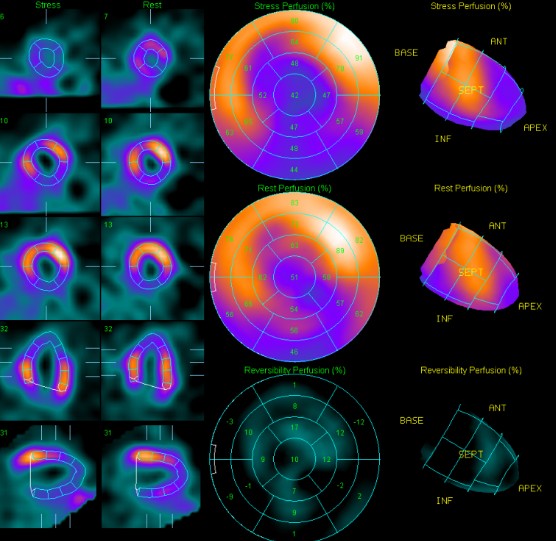
An electrocardiogram demonstrated sinus rhythm with poor R progression. Echocardiogram showed LA, LV dilatation , Impaired LV systolic function (A4C 31% ), impaired LV diastolic function.Previous Thallium-201 myocardial perfusion scan showed fixed perfusion defects in the apical, inferolateral, proximal inferior, and inferoseptal walls of the left ventricle, suggestive of prior myocardial infarction with mixed viable and nonviable myocardium.
Relevant Catheterization Findings
Coronary angiogram was performed 4 months ago(2025/06/12), which showed 3-vessel disease and middle left circumflex (LCx) chronic total occlusion (CTO). He was then referred to CVS OPD for SDM of CABG. After discussion, the patient declined CABG due to personal factors (single/ poor economic condition/ pre-dialysis status) and decided PCI. PCI was postponed scheduled for several times due to his work schedule before this admission.
Interventional Management
Procedural Step
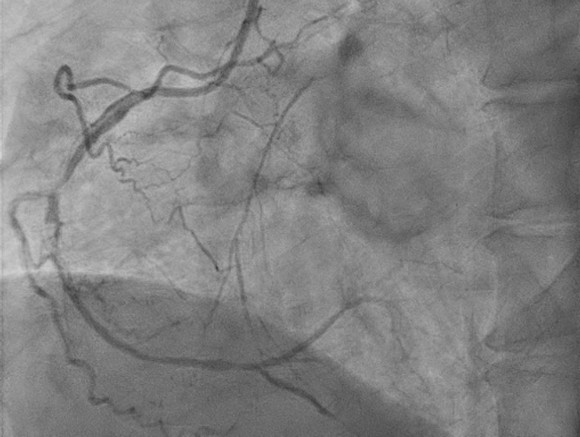
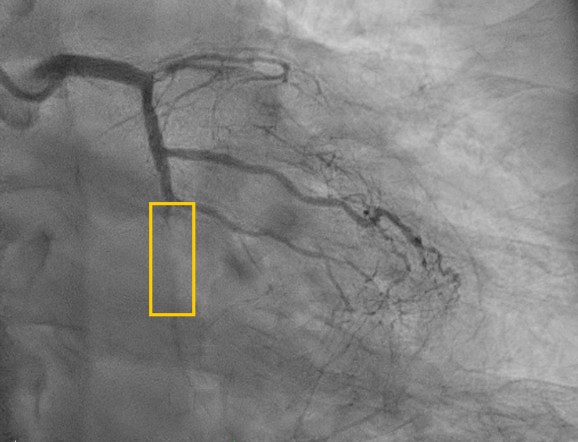
Before the procedure , we had contacted CVS team backed up for a possible emergent ECMO implantation. First, we performed PTCA for RCA successfully and prominent retrograde perfusion at middle-distal LAD via collateral branches from RCA is noted .
This time Left coronary angiography showed progression of LAD lesion (99% stenosis to total occlusion). We used Runthrough floppy to OM1 branch , then advanced Sasuke with XT-A via runthrough floppy for better support. For failure of passing through LCX distal lesion, we exchange XT-A to Gaia 2. Lesion was then crossed successfully then dilated with small balloons gradually (1.0 mm then 2.0 mm). We then confirmed with IVUS and showed the wire was in the true lumen.
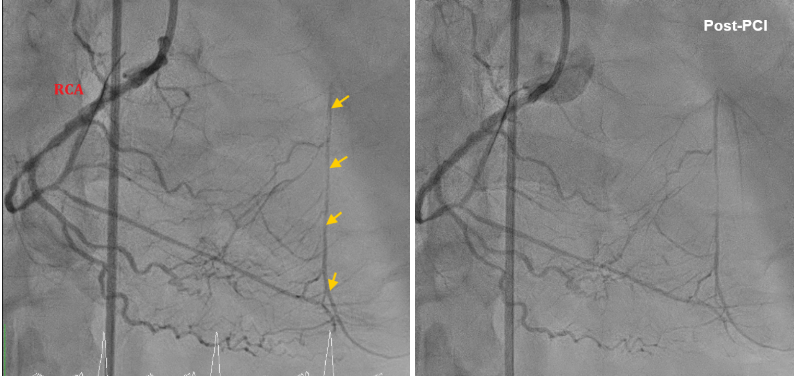
After finishing PTCA of LCx, we then coped with LAD CTO. We passed the 1st CTO lesion of LAD with XT-A , successfully advanced to the diagonal branch. However, 2nd CTO lesion was noted over bifurcation of 2nd diagonal branch and LAD. We then advanced SASUKE double lumen catheter with UB3 for better controllability. UB3 was advanced to distal LAD successfully. For the poor economic situation, 2 bare-metal stents were placed at proximal-middle LAD finally. The final angiogram showed an acceptable result. As a result, he had a stable hemodynamic condition peri- and post-PCI. The PCI was successful, efficient(total flouro time 77 min), and smooth. He was discharged with improved symptoms .

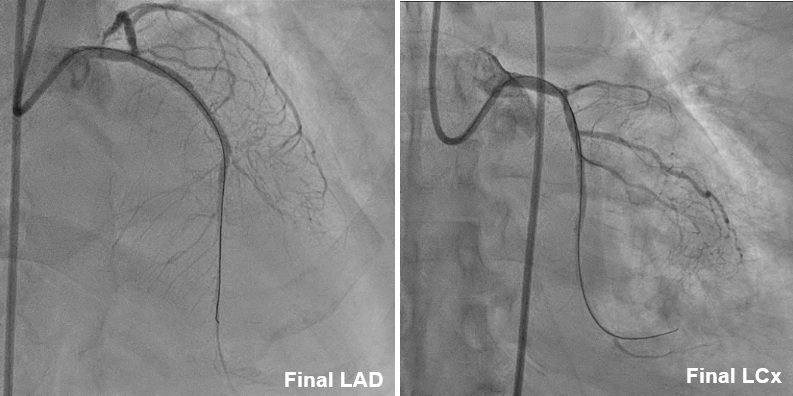
This time Left coronary angiography showed progression of LAD lesion (99% stenosis to total occlusion). We used Runthrough floppy to OM1 branch , then advanced Sasuke with XT-A via runthrough floppy for better support. For failure of passing through LCX distal lesion, we exchange XT-A to Gaia 2. Lesion was then crossed successfully then dilated with small balloons gradually (1.0 mm then 2.0 mm). We then confirmed with IVUS and showed the wire was in the true lumen.
After finishing PTCA of LCx, we then coped with LAD CTO. We passed the 1st CTO lesion of LAD with XT-A , successfully advanced to the diagonal branch. However, 2nd CTO lesion was noted over bifurcation of 2nd diagonal branch and LAD. We then advanced SASUKE double lumen catheter with UB3 for better controllability. UB3 was advanced to distal LAD successfully. For the poor economic situation, 2 bare-metal stents were placed at proximal-middle LAD finally. The final angiogram showed an acceptable result. As a result, he had a stable hemodynamic condition peri- and post-PCI. The PCI was successful, efficient(total flouro time 77 min), and smooth. He was discharged with improved symptoms .
Case Summary
- We use IVUS in all vessels especially CTO lesions for ensuring no subintimal penetration and stent sizing. IVUS offers a real-time cross-sectional image of the lumen and the vessel wall and assisting guide-wire crossing,especially in long and calcified complex lesions.- SASUKE double lumen microcatheter played an important role in the severe calcification and tortuosity- Repeat coronary angiography would be arranged 6 months later for high risk of ISR (all bare-metal stents, severely calcification)