Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251103_002
106 Days of Relentless Care and Hope: A Journey Through Acute Coronary Syndrome and Recovery
By Tse-Wei Chen
Presenter
Tse-Wei Chen
Authors
Tse-Wei Chen1
Affiliation
National Cheng Kung University Hospital, Taiwan1
View Study Report
CASE20251103_002
Coronary - ACS/AMI
106 Days of Relentless Care and Hope: A Journey Through Acute Coronary Syndrome and Recovery
Tse-Wei Chen1
National Cheng Kung University Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
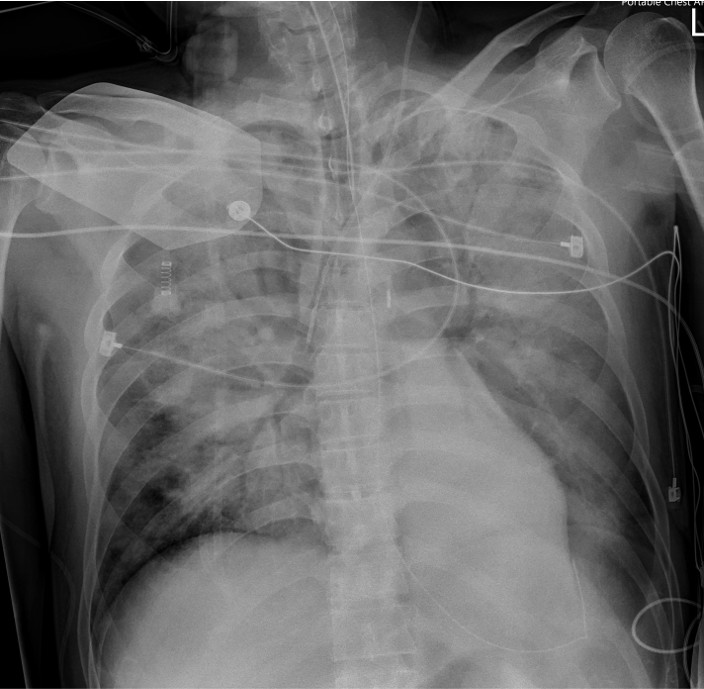
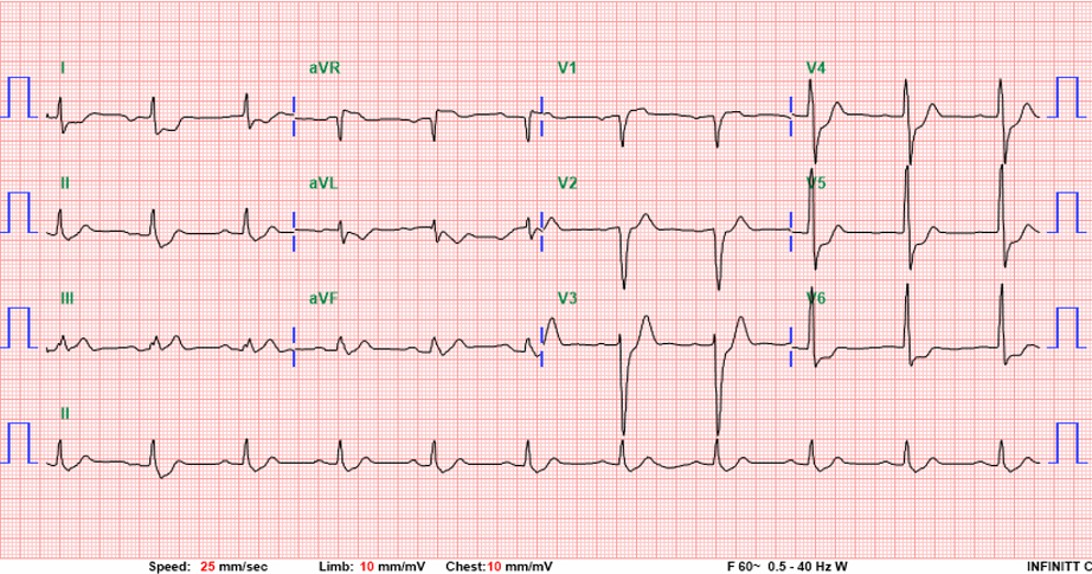
A 50-year-old man with hypertension and ulcerative colitis on vedolizumab developed dyspnea and chest tightness while visiting Taiwan. On February 28, he collapsed after bathing with pulseless electrical activity arrest. Cardiopulmonary resuscitation for 48 minutes achieved return of spontaneous circulation. Electrocardiogram showed ST elevation in aVR with diffuse ST depression. Lactate was 11.5 mmol/L. ECMO and IABP were initiated for cardiogenic shock.
 TCTAP-1(1).mp4
TCTAP-1(1).mp4
TCTAP-1(2).mp4
TCTAP-1(3).mp4
Relevant Test Results Prior to Catheterization
Electrocardiogram showed ST elevation in aVR with diffuse ST depression (V4–V6), suggesting left main or triple-vessel ischemia. Echocardiography revealed a severely reduced LVEF of 10–20%. Laboratory tests showed creatinine 1.37 mg/dL, AST/ALT 161/119 U/L, and lactate 11.5 mmol/L. Chest CT demonstrated bilateral dependent consolidation without aortic dissection, consistent with a STEMI equivalent and cardiogenic shock.


2nd PCI(2).mp4
LCX STENT.mp4
LM DCB.mp4
Relevant Catheterization Findings
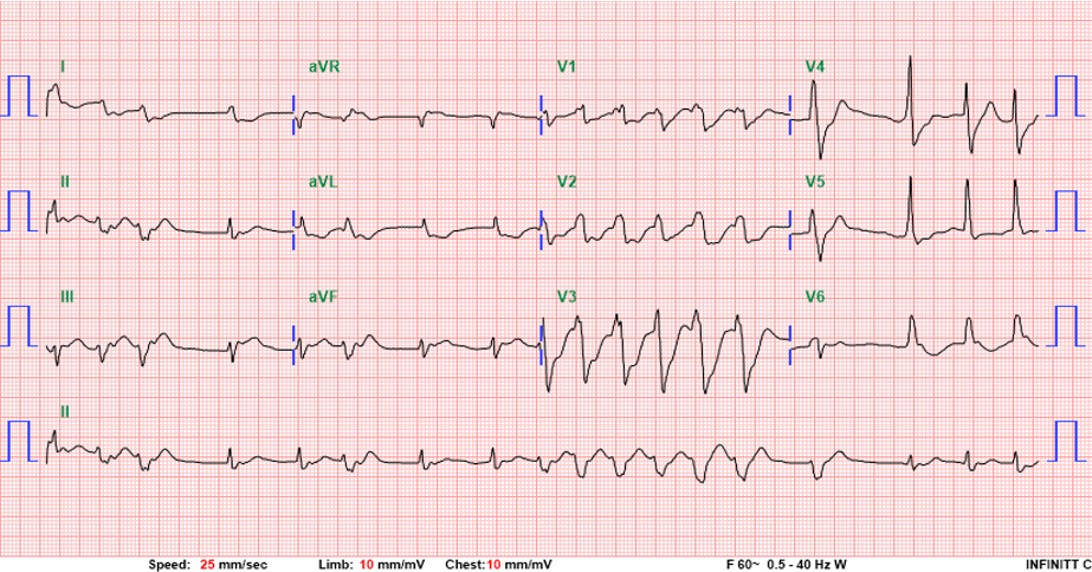
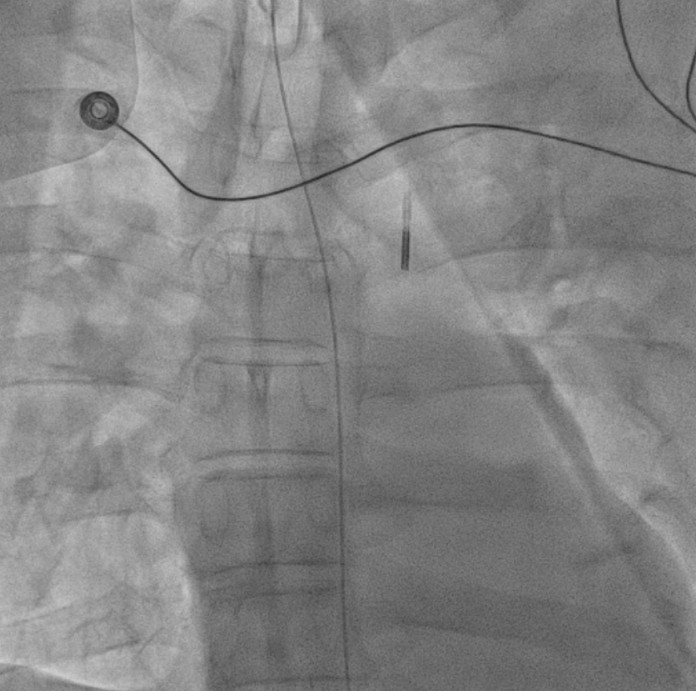
Coronary angiography revealed critical left main and triple-vessel coronary artery disease. The right coronary artery and posterolateral branch were totally occluded, serving as infarct-related lesions. TIMI flow improved from 0 to 3 after deployment of two drug-eluting stents in the RCA and RCA-PL. Residual severe disease in the left main, LAD, and LCX was reserved for staged PCI. Periprocedural VT was defibrillated twice (200 J) under VA-ECMO and IABP support.

Severe MR(1).mp4
Severe MR(2).mp4
Severe MR(3).mp4
Interventional Management
Procedural Step
Primary Intervention (Feb 28): During extracorporeal cardiopulmonary resuscitation, two drug-eluting stents were implanted in the right coronary artery and posterolateral branch under VA-ECMO and IABP support. Ventricular tachycardia during PCI was successfully defibrillated, and targeted temperature management was initiated.
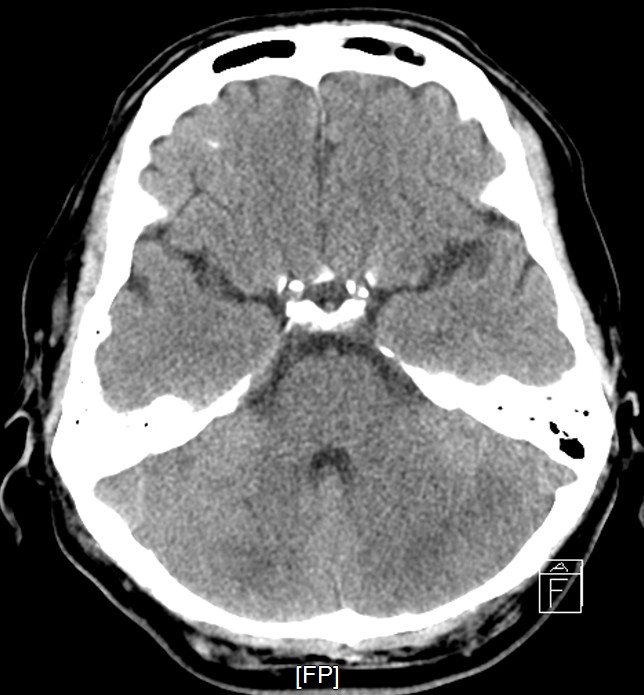
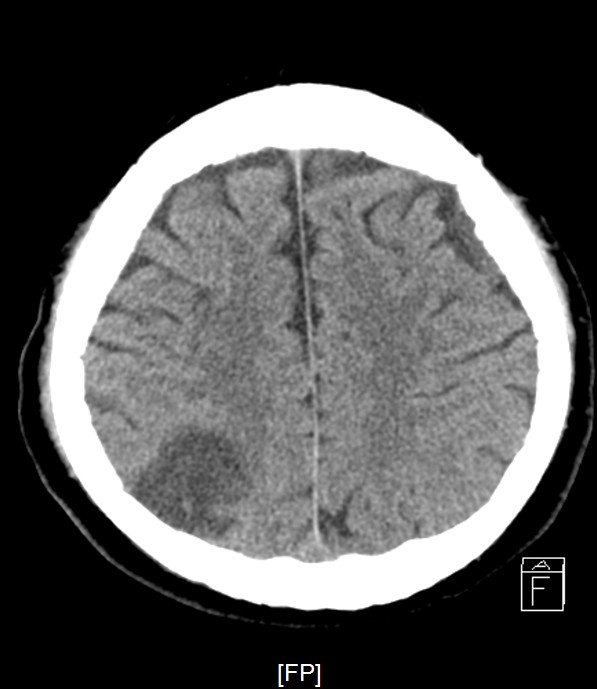
Staged PCI (Mar 6): One DES was placed in the LCX and one DCB in the LM–LCX segment. ECMO and IABP were successfully removed on March 8. Continuous renal replacement therapy was started for acute kidney injury. Brain CT showed watershed infarcts and a small subarachnoid hemorrhage, followed by gradual neurological recovery.
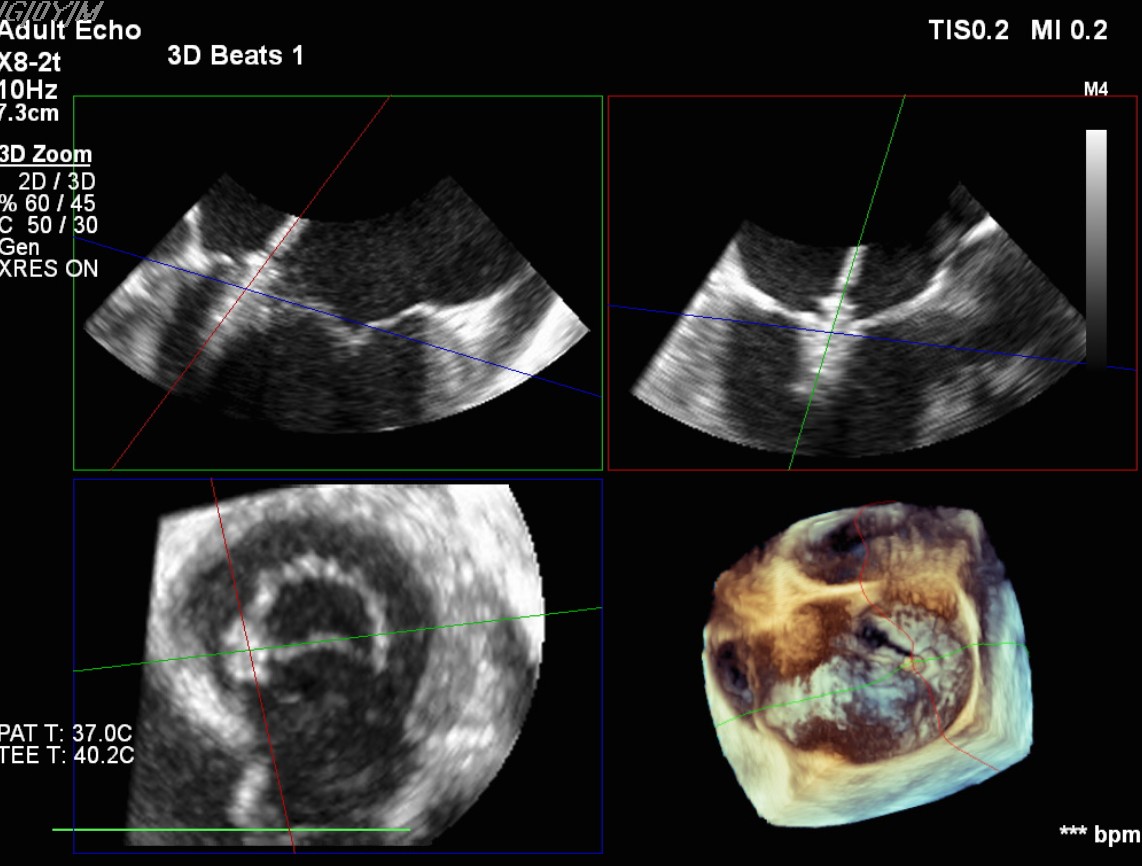
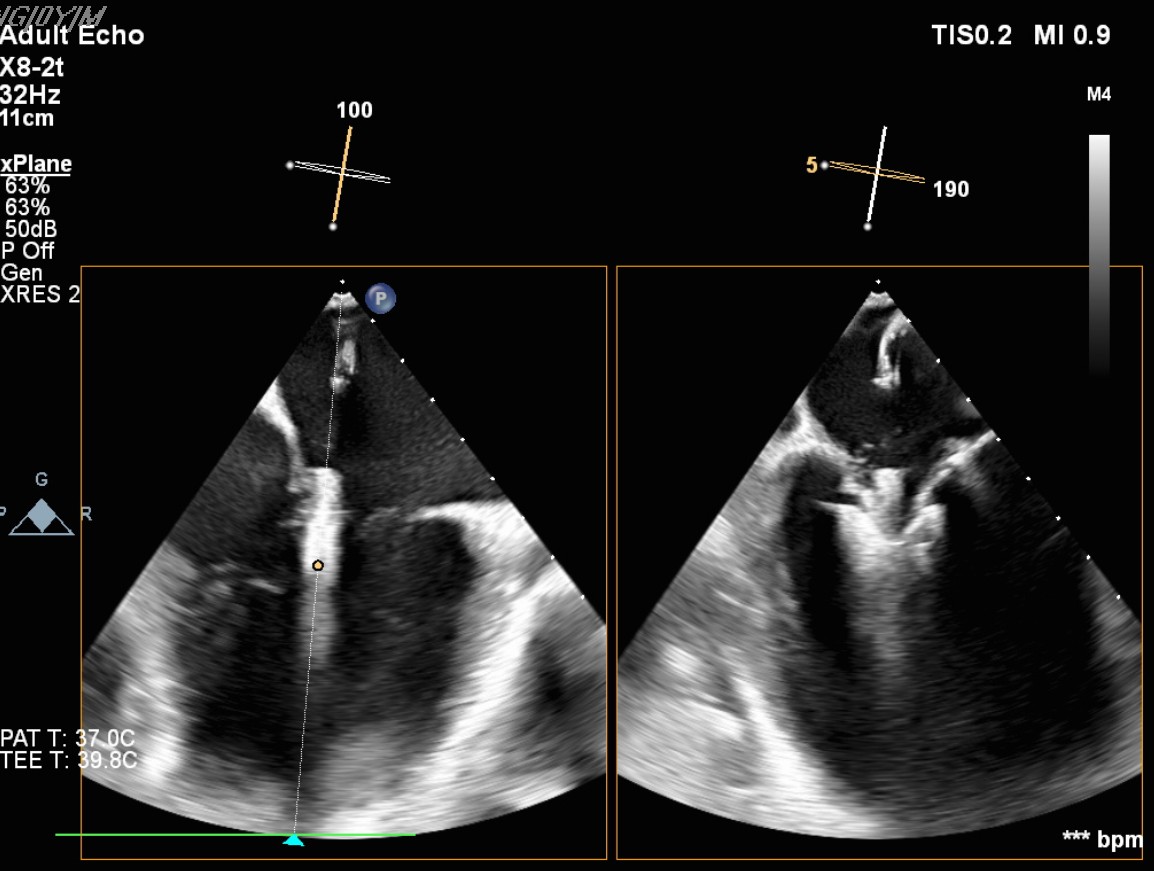
Transcatheter Edge-to-Edge Repair (Mar 27): TEE demonstrated severe mitral regurgitation with low cardiac output (~2 L/min). Two G4 XTW MitraClips were implanted successfully, improving hemodynamics.
Staged LM–LAD PCI (Apr 18): Two DES were deployed in the LM–LAD under mechanical and pharmacologic support.
Supportive Management (Mar–Jun): Multiple ventilator-associated pneumonias (S. maltophilia, E. cloacae) and ARDS were managed with prone positioning (Mar 18–21, Apr 23–25, May 1–3). Tracheostomy was performed on April 7, and VATS decortication for left upper lobe hematoma on April 30. Recurrent AF with RVR required cardioversion (Mar 7, Jun 10). By June, the patient was successfully weaned, with LVEF 39% and moderate MR. He was discharged on June 13 in stable condition for medical air transport.

LAD STENT(1).mp4
LAD STENT(2).mp4
5st CAG(3).mp4
Staged PCI (Mar 6): One DES was placed in the LCX and one DCB in the LM–LCX segment. ECMO and IABP were successfully removed on March 8. Continuous renal replacement therapy was started for acute kidney injury. Brain CT showed watershed infarcts and a small subarachnoid hemorrhage, followed by gradual neurological recovery.
Transcatheter Edge-to-Edge Repair (Mar 27): TEE demonstrated severe mitral regurgitation with low cardiac output (~2 L/min). Two G4 XTW MitraClips were implanted successfully, improving hemodynamics.
Staged LM–LAD PCI (Apr 18): Two DES were deployed in the LM–LAD under mechanical and pharmacologic support.
Supportive Management (Mar–Jun): Multiple ventilator-associated pneumonias (S. maltophilia, E. cloacae) and ARDS were managed with prone positioning (Mar 18–21, Apr 23–25, May 1–3). Tracheostomy was performed on April 7, and VATS decortication for left upper lobe hematoma on April 30. Recurrent AF with RVR required cardioversion (Mar 7, Jun 10). By June, the patient was successfully weaned, with LVEF 39% and moderate MR. He was discharged on June 13 in stable condition for medical air transport.
Case Summary
This 106-day journey demonstrates the life-saving potential of integrated mechanical circulatory support, multistaged high-risk PCI, and structural intervention in post-arrest STEMI complicated by multiorgan failure. From 48-minute CPR and ECMO to recovery with an LVEF of 39%, the case underscores the vital role of staged PCI under evolving hemodynamic conditions. Multidisciplinary collaboration among interventional, critical care, and surgical teams was pivotal, truly a testament to relentless care and hope.