Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251103_001
Staying Safe in the Storm: Hemodynamic Support With Impella in High-Risk PCI
By Youning Chang, Yilin Tsai
Presenter
Youning Chang
Authors
Youning Chang1, Yilin Tsai2
Affiliation
National Yang Ming Chiao Tung Hospital, Taiwan1, Taipei Veteran General Hospital, Taiwan2
View Study Report
CASE20251103_001
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
Staying Safe in the Storm: Hemodynamic Support With Impella in High-Risk PCI
Youning Chang1, Yilin Tsai2
National Yang Ming Chiao Tung Hospital, Taiwan1, Taipei Veteran General Hospital, Taiwan2
Clinical Information
Relevant Clinical History and Physical Exam
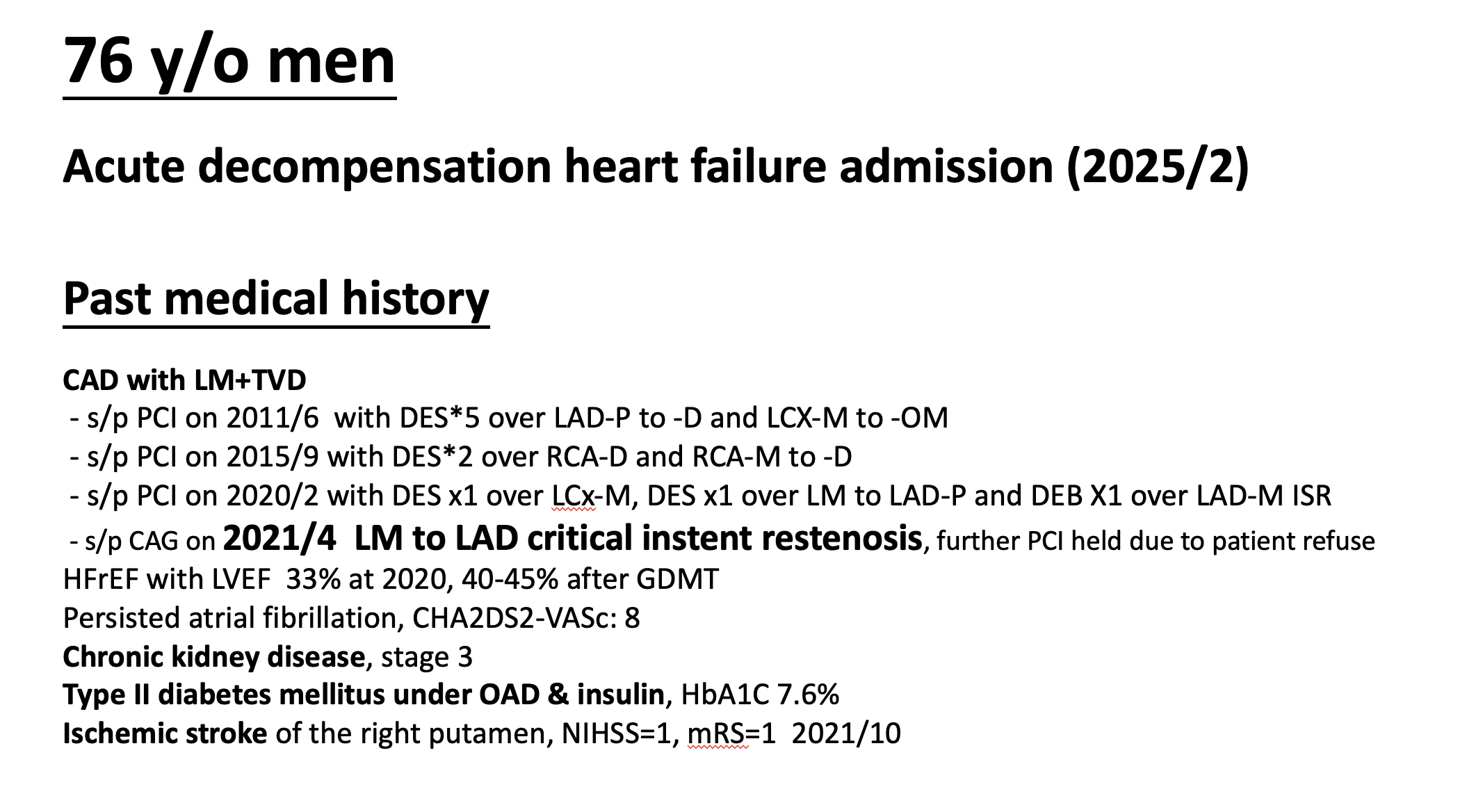
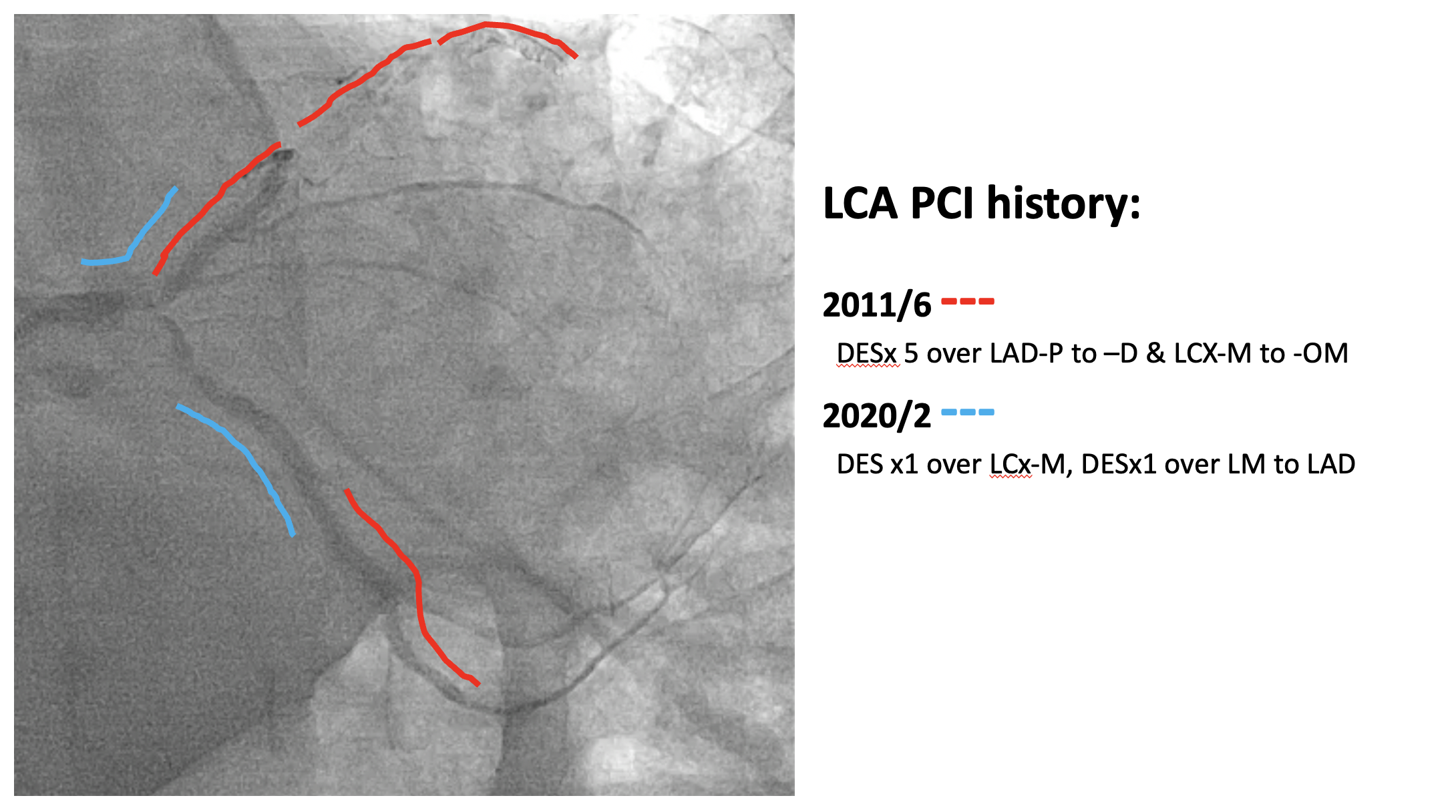
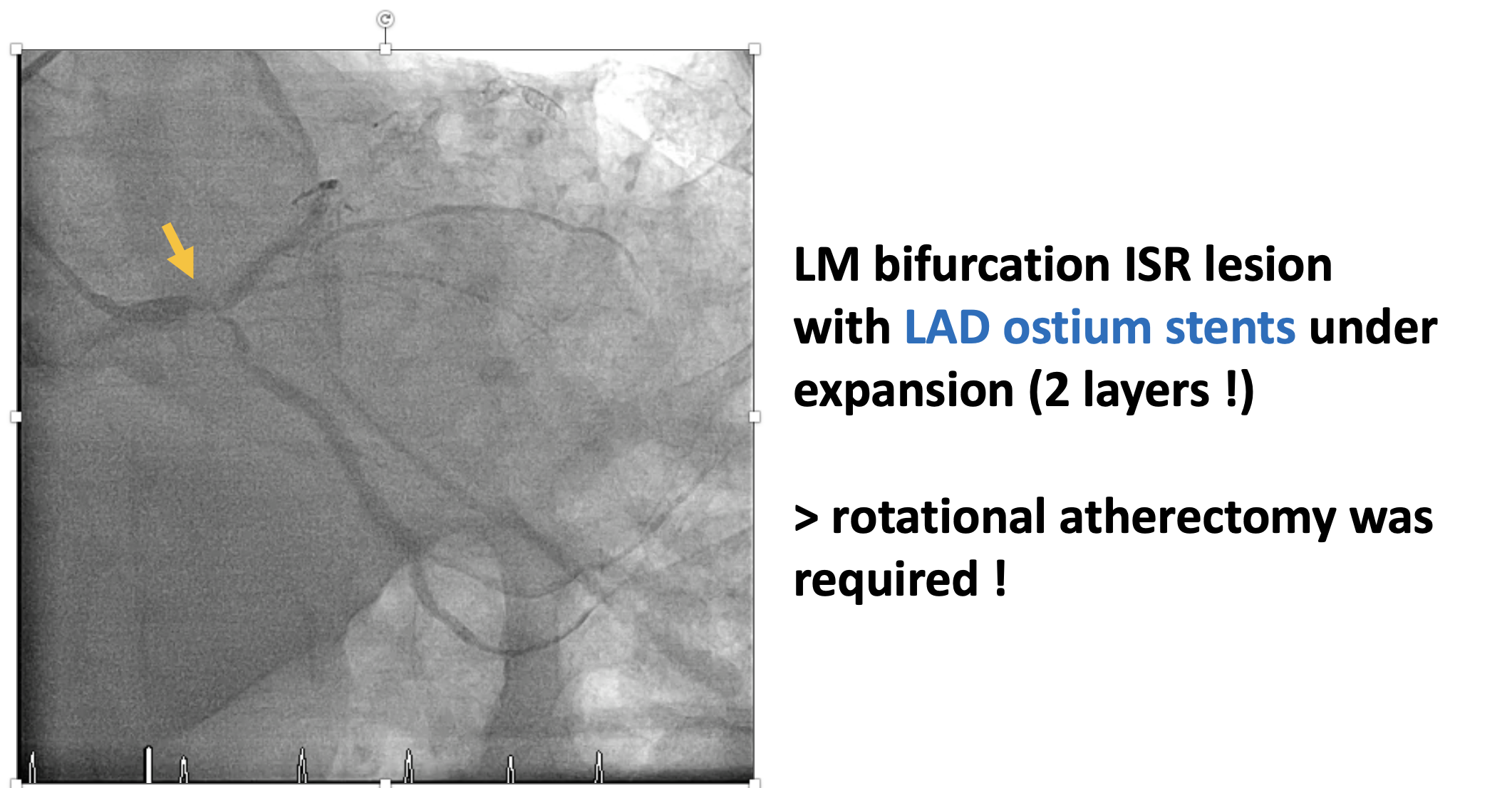
A 76-year-old man with multivessel coronary artery disease underwent multiple prior PCIs since 2011. He was admitted for acute decompensated heart failure with LVEF 32% and severe MR. Physical exam revealed pulmonary rales, elevated JVP. Despite optimal GDMT, he remained in NYHA IV. Hemodynamics showed CI 2.07 L/min/m² and PCWP 34 mmHg. Owing to low output and high-risk anatomy (LM bifurcation ISR with two stent layers), Impella-assisted PCI with rotational atherectomy and IVL were decided.
Relevant Test Results Prior to Catheterization
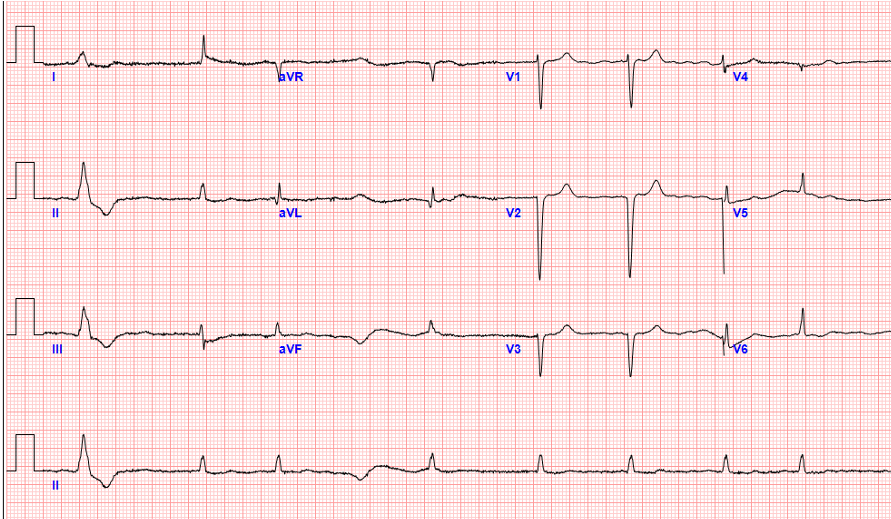
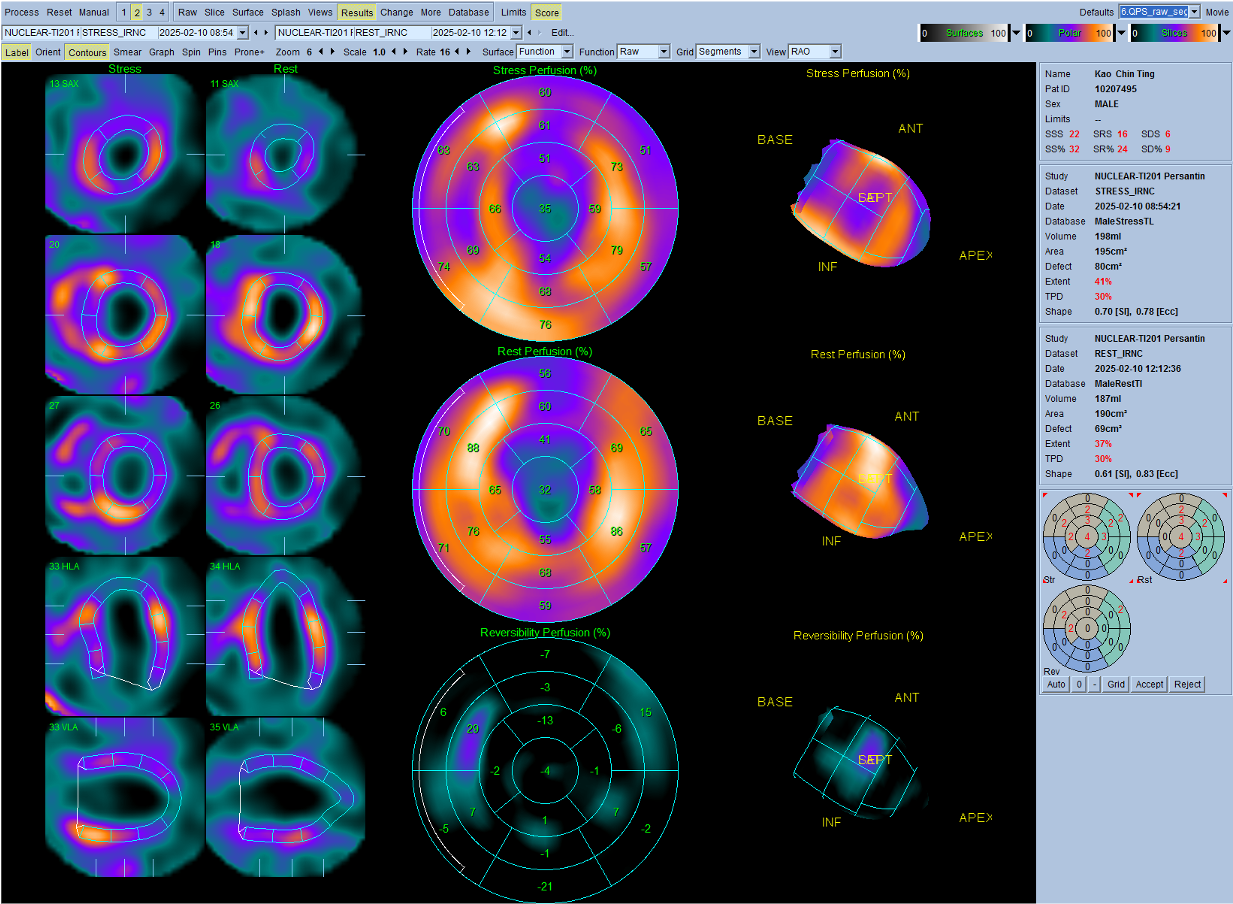
Echocardiography revealed LVEF 32% with severe functional mitral regurgitation, LVEDD 61 mm, and RV dysfunction (TAPSE 1.4 cm). BNP was 6421 pg/mL. Chest X-ray showed pulmonary congestion and cardiomegaly. ECG demonstrated sinus tachycardia with Q waves over anterior leads. Renal and hepatic profiles were mildly impaired, and NT-proBNP remained elevated despite guideline-directed medical therapy.

 Pre--procedure TTE A4C.mp4
Pre--procedure TTE A4C.mp4
pre-procedurel TTE A2C.mp4
Relevant Catheterization Findings
Coronary angiography revealed severe in-stent restenosis of the distal left main and bifurcation involving the LAD and LCx, with multiple overlapping stent layers. TIMI-2 flow was noted in LAD, and the LCx ostium was heavily calcified. LVEDP was 32 mmHg, and cardiac index 2.07 L/min/m². The lesion was classified as a high-risk CHIP case, requiring hemodynamic support with Impella CP before complex PCI.

LCA CAUDAL ANGIO.mp4
LCA CRAN ANGIO LAD CTO.mp4
LCA SPIDER ANGIO.mp4
Interventional Management
Procedural Step
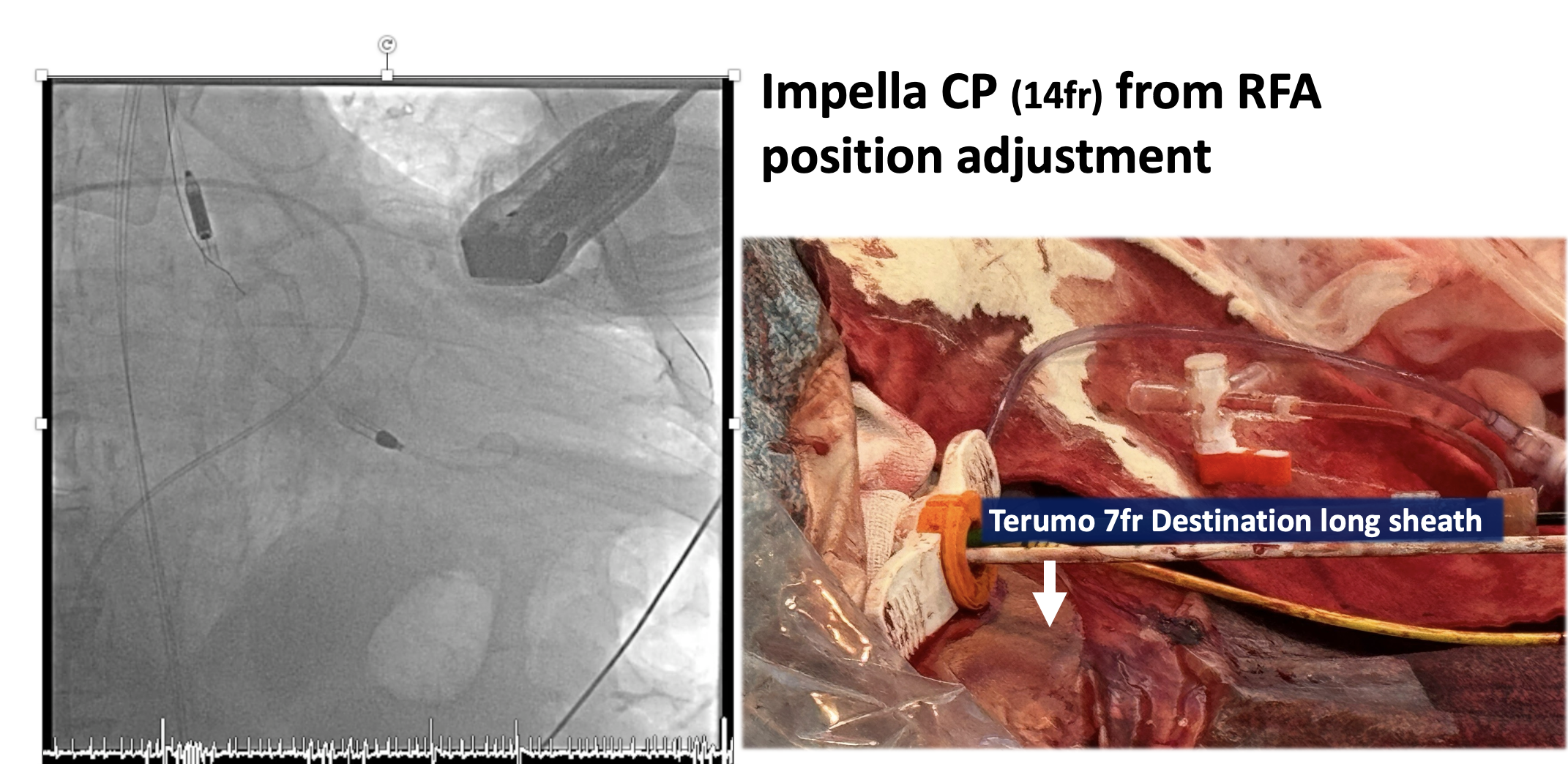
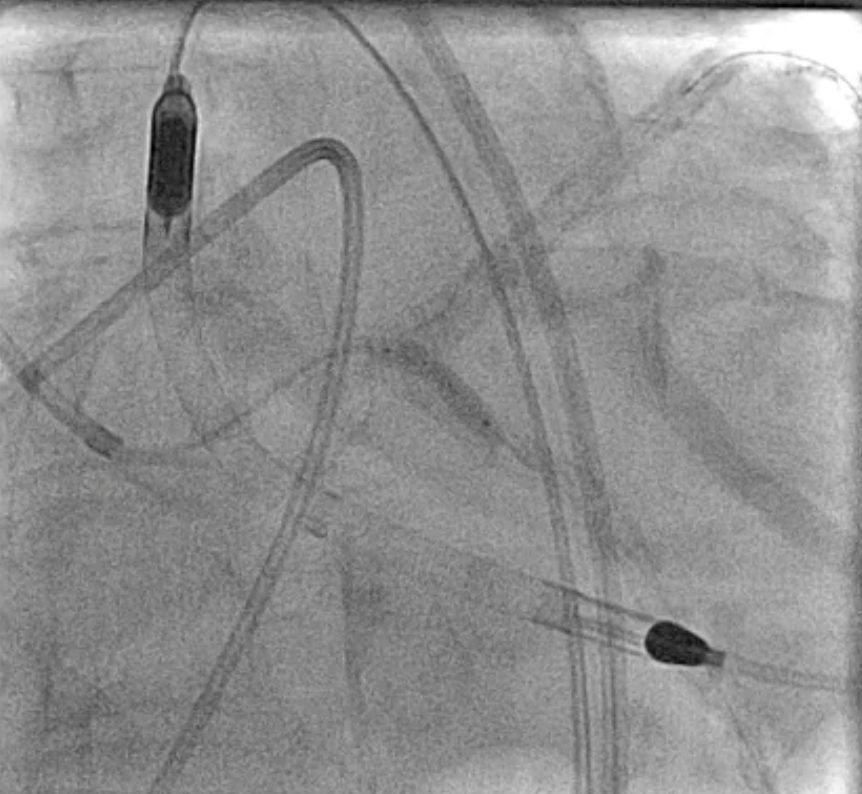
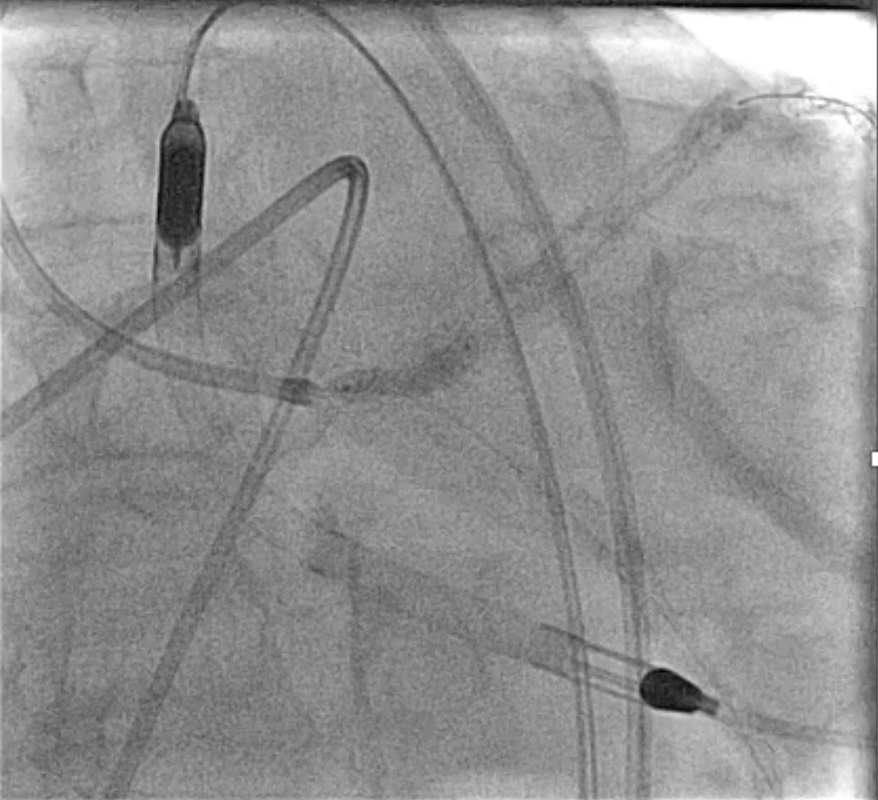
An Impella CP was inserted via the right femoral artery for hemodynamic support (baseline CI 2.07 L/min/m², PCWP 34 mmHg). The LM was engaged with a 7 Fr EBU 3.5 guiding catheter. Angiography demonstrated heavily calcified distal LM bifurcation ISR with multiple stent layers extending into both LAD and LCX. Rotational atherectomy (RA) using a 1.5-mm burr was first attempted at the LAD-distal segment, but severe calcification prevented smooth burr passage even under Dyna mode. After changing to a 2.0-mm burr, the lesion was successfully crossed and adequately modified. Subsequently, the 1.5-mm burr was redirected for LCX lesion debulking, but burr entrapment occurred at the proximal LCX during the third run. Hemodynamics remained stable under Impella support. The burr was freed using a combination of deep seating a Guideplus ST for additional backup, small-balloon anchoring, and gentle forward–reverse rotation maneuvers. To ensure complete plaque modification, a 2.0-mm burr was used again to finalize both LAD and LCX runs. Cutting balloon angioplasty yielded suboptimal expansion; therefore, intravascular lithotripsy (IVL 3.5 mm, ≈40 pulses per ostium) was applied to achieve calcium fracture and full balloon compliance. Lesions were treated with DEB 4.0×30 mm LM–LAD and 3.0×30 mm LCX, followed by kissing balloon inflation. The Impella was removed uneventfully, and the patient recovered without hemodynamic compromise. Final angiogram showed well-apposed stents.
LM to LAD 1.5 burr pass.mp4
LCX burr entrapment.mp4
LM-LCX 2.0 burr passed previous entrapped part.mp4
Case Summary
This case highlights the critical role of mechanical circulatory support in complex high-risk PCI. Impella CP provided stable hemodynamics throughout prolonged bifurcation intervention, enabling safe management of burr entrapment and aggressive calcium modification. The combined use of rotational atherectomy, intravascular lithotripsy, and advanced guide support techniques achieved optimal stent expansion with complete revascularization. Early use of percutaneous support allows interventionalists to focus on lesion preparation and procedural precision, minimizing complications and improving outcomes in complex coronary interventions.