Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251102_023
A Gentle Rescue- Treating Severe Heart Failure With Complex 3VD and 3 CTO
By Tan Jihtze
Presenter
Tan Jihtze
Authors
Tan Jihtze1
Affiliation
Dalin Buddhist Tzu Chi Hospital , Taiwan1
View Study Report
CASE20251102_023
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
A Gentle Rescue- Treating Severe Heart Failure With Complex 3VD and 3 CTO
Tan Jihtze1
Dalin Buddhist Tzu Chi Hospital , Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
A 57-year-old man, Mr. Chen, who suffers from atrial flutter, chronic heart failure classified as NYHA class III, chronic kidney disease stage IV, and cholestasis with a total bilirubin level of 3.0 mg/dL. His chief complaint is progressively worsening shortness of breath on exertion. He was treated with heart failure guideline directed medical therapy: Entresto, Empagliflozin, Spironolactone, Bisoprolol and Amiodarone.

Relevant Test Results Prior to Catheterization
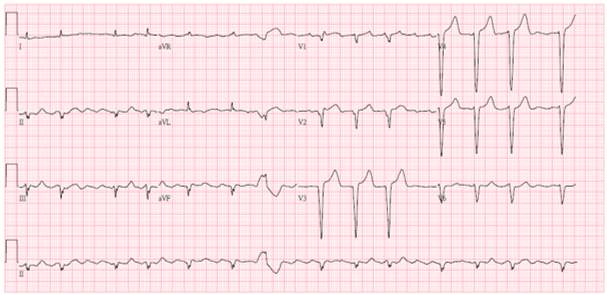
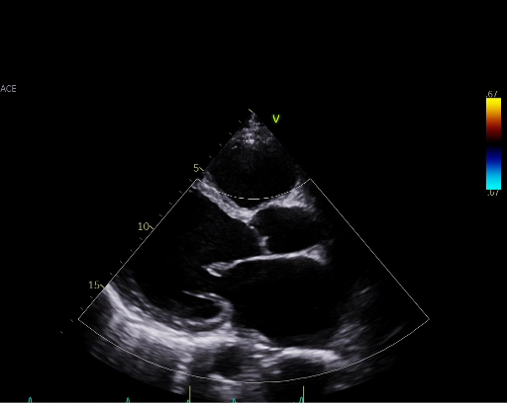
Chest X ray showed cardiomegaly. ECG showed atrial fibrillation rhythm with poor R progression. Echocardiography revealed markedly depressed left ventricular systolic function, with a left ventricular ejection fraction (LVEF) of 20.19%, accompanied by moderate mitral and tricuspid regurgitation.
Relevant Catheterization Findings
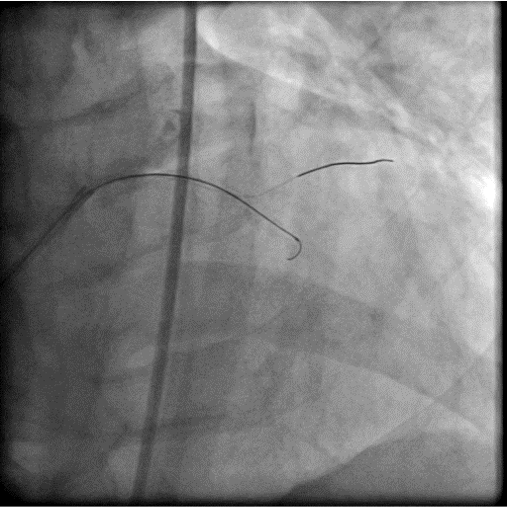
The coronary angiogram showed middle LAD CTO, LCX critical stenosis and RCA CTO with collateral from LCX. J-CTO score for LAD was 3 points . J-CTO score for RCA was 4 points. The CHIP PCI score was 11.
 LAD.mp4
LAD.mp4
LCX.mp4
RCA.mp4
Interventional Management
Procedural Step
The procedure was done in two stage. For first stage, we use upfront IABP as a mechanical support with ECMO access route prepared and ECMO team standby. The LAD CTO was the first target as it was relatively short, not a donor vessels and would provide greatest benefit to the patient. With antegrade approach and wire escalation technique ( Fielder XTA, Fielder XTR, Gaia 1st), we finally punctured into the proximal cap with Gaia 3rd and immediately deescalate the wire to Sion black to navigate through the CTO body and finally managed to reach distal true lumen with a Sion Black. Then we did the circumflex lesion starting with a Sion Black. However, the Sion Black and Fielder XTR could not cross the lesion. We then escalate the wire to Gaia 1st.
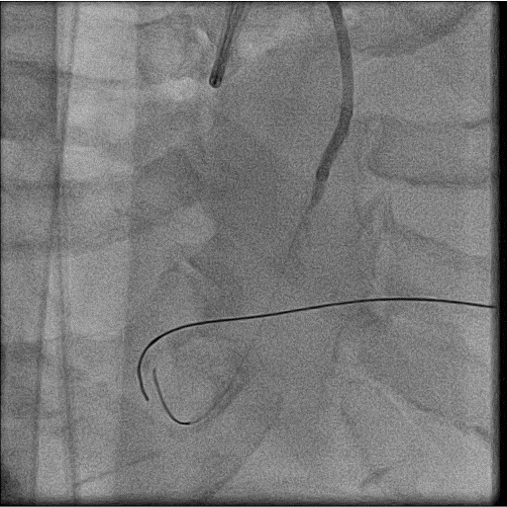
For 2nd stage procedure, we did the RCA CTO with primary retrograde approach due to ambiguous proximal cap and distal cap is a bifurcation. The initial retrograde wire escalation technique was failed to puncture into the distal cap by using SIon, Gladius EX and even Gaia 3rd wire. So we shift to antegrade approach starting with Gladius EX wire but we failed too. Then retrograde puncture was reattempted with Miracle 6 wire. It successfully punctured into the distal cap. By using kissing wire technique, antegrade wire entered distal true lumen. The procedure was finished with balloon dilatation and stenting. We were abled to preserve the distal PL and PDA branch.

LAD.mp4
LCX.mp4
RCA final 1.mp4
For 2nd stage procedure, we did the RCA CTO with primary retrograde approach due to ambiguous proximal cap and distal cap is a bifurcation. The initial retrograde wire escalation technique was failed to puncture into the distal cap by using SIon, Gladius EX and even Gaia 3rd wire. So we shift to antegrade approach starting with Gladius EX wire but we failed too. Then retrograde puncture was reattempted with Miracle 6 wire. It successfully punctured into the distal cap. By using kissing wire technique, antegrade wire entered distal true lumen. The procedure was finished with balloon dilatation and stenting. We were abled to preserve the distal PL and PDA branch.
Case Summary
In conclusion, successful management of complex PCI cases requires meticulous planning and gentle technique to minimize procedural risks. While mechanical circulatory support can be valuable in stabilizing high-risk patients, the success and safety of the procedure ultimately depend more on careful execution and operator skill. Moreover, mechanical support itself does not eliminate the possibility of complications and, in some cases, may even introduce additional risks if not judiciously used.