Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251102_021
Transcatheter Closure of Ruptured Right Sinus of Valsalva With Multifunctional Occluder: A Comprehensive Assessment & Procedural Guide
By Chai Yih Tan, Kai Soon Liew, Prabahkar Subramaniam, Mohd Khairi Othman, Christian Sunur, Nadiah Baddrudin, Dharmaraj Karthikesan, Saravanan Krishinan, Abdul Rahim Wong, Kantha Rao Narasamuloo
Presenter
Nadiah Baddrudin
Authors
Chai Yih Tan1, Kai Soon Liew1, Prabahkar Subramaniam1, Mohd Khairi Othman1, Christian Sunur1, Nadiah Baddrudin1, Dharmaraj Karthikesan1, Saravanan Krishinan1, Abdul Rahim Wong2, Kantha Rao Narasamuloo1
Affiliation
Hospital Sultanah Bahiyah, Malaysia1, Lincoln University College, Malaysia2
View Study Report
CASE20251102_021
Structural - Other Structural Interventions
Transcatheter Closure of Ruptured Right Sinus of Valsalva With Multifunctional Occluder: A Comprehensive Assessment & Procedural Guide
Chai Yih Tan1, Kai Soon Liew1, Prabahkar Subramaniam1, Mohd Khairi Othman1, Christian Sunur1, Nadiah Baddrudin1, Dharmaraj Karthikesan1, Saravanan Krishinan1, Abdul Rahim Wong2, Kantha Rao Narasamuloo1
Hospital Sultanah Bahiyah, Malaysia1, Lincoln University College, Malaysia2
Clinical Information
Relevant Clinical History and Physical Exam
The patient is a 33 years old gentleman without co-morbidity. He reports an episode of syncope after a strenuous exercise during adolescence time. He had no repeated episode of syncope & remained well until a year ago where he developed reduced effort tolerance without other symptoms of heart failure. From clinical examination, he has no clubbing & cyanosis. Apex is not displace with normal first & second heart sound. A continuous murmur was heart over the left sternal edge.
Relevant Test Results Prior to Catheterization
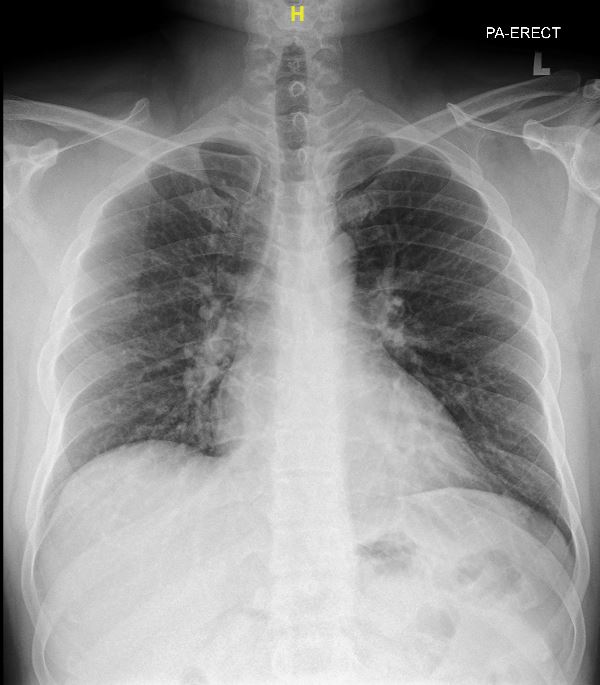
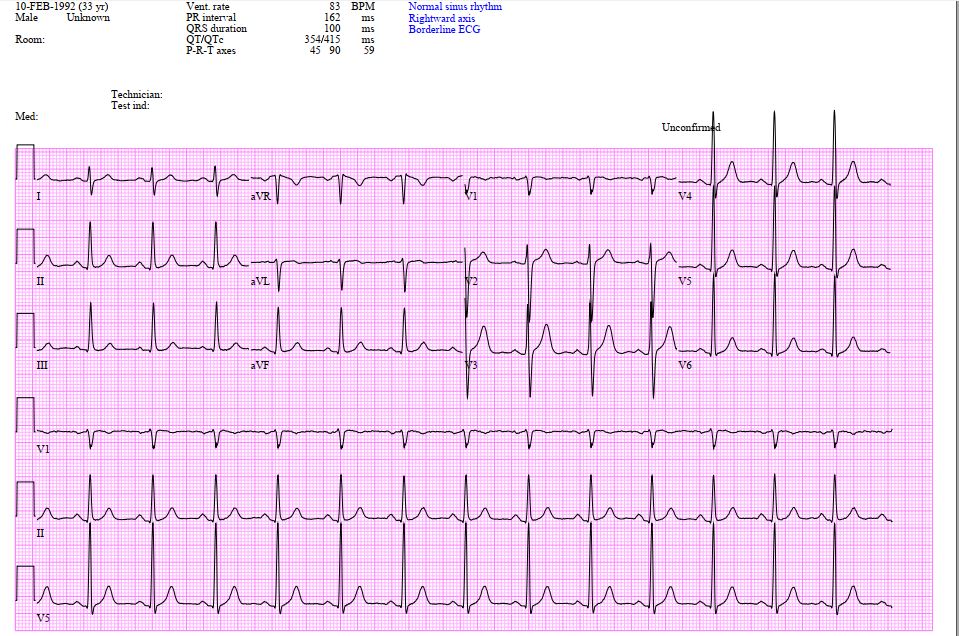
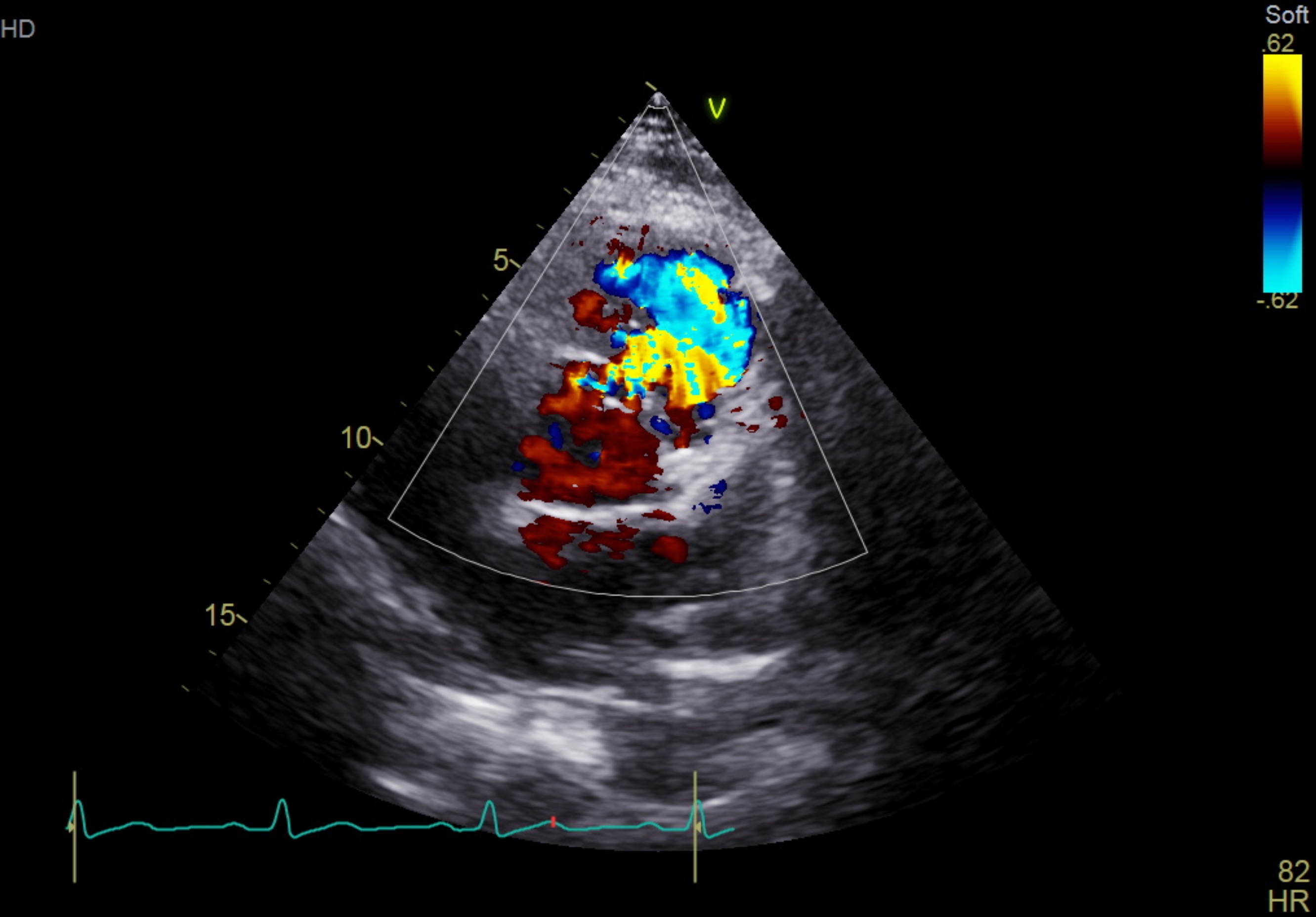
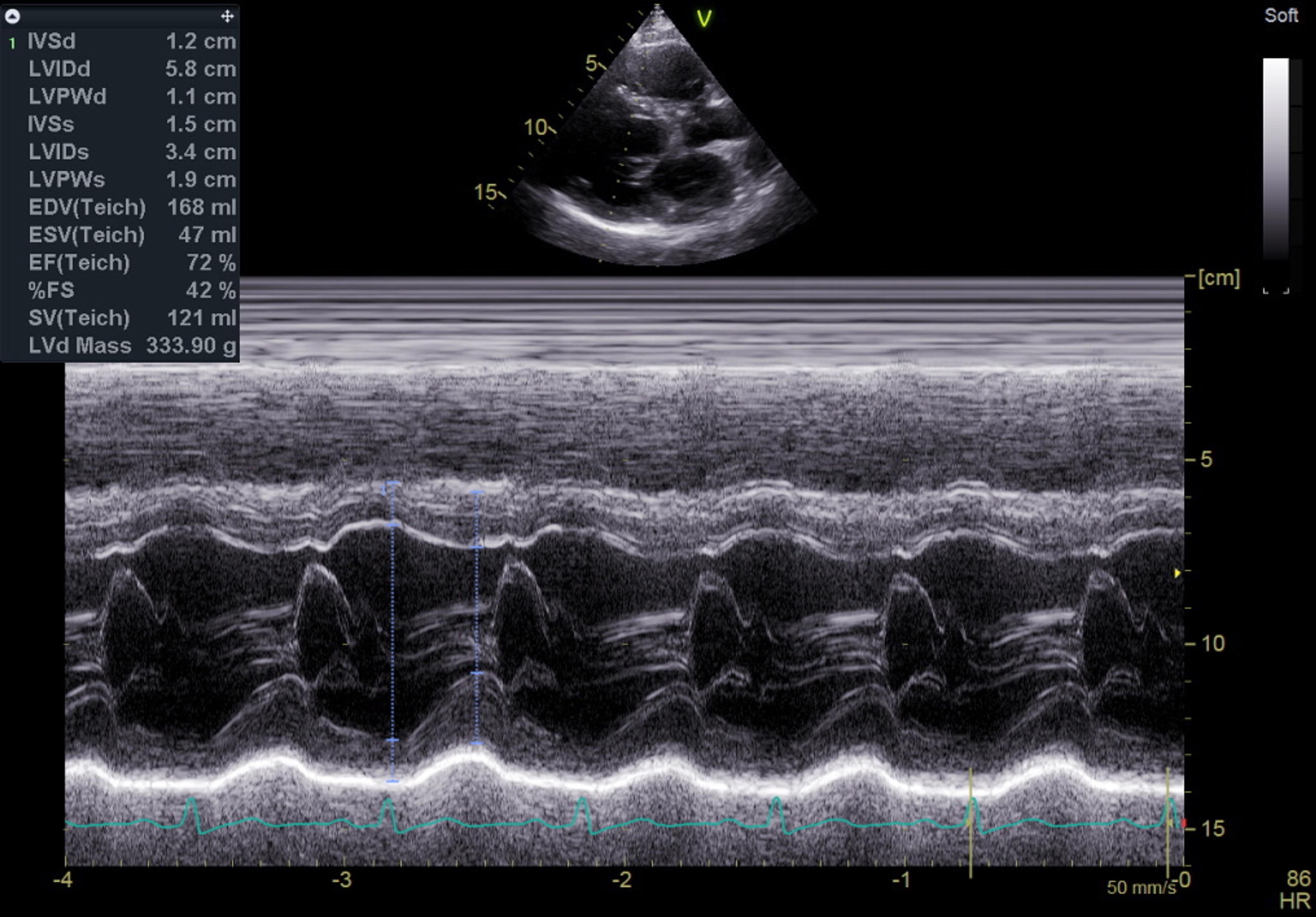
The electrocardiogram shows sinus rhythm, normal axis with left ventricular hypertrophy. The chest X-ray shows a normal cardiac silhouette without prominent pulmonary trunk. His NT-ProBNP was raised with normal troponin reading.The trans-thoracic echocardiogram revealed a ruptured right sinus of valsalva (SOV) with left to right shunting to right ventricle. The aorta is dilated without aortic valve regurgitation. The left ventricle is dilated with 63% of ejection fraction.
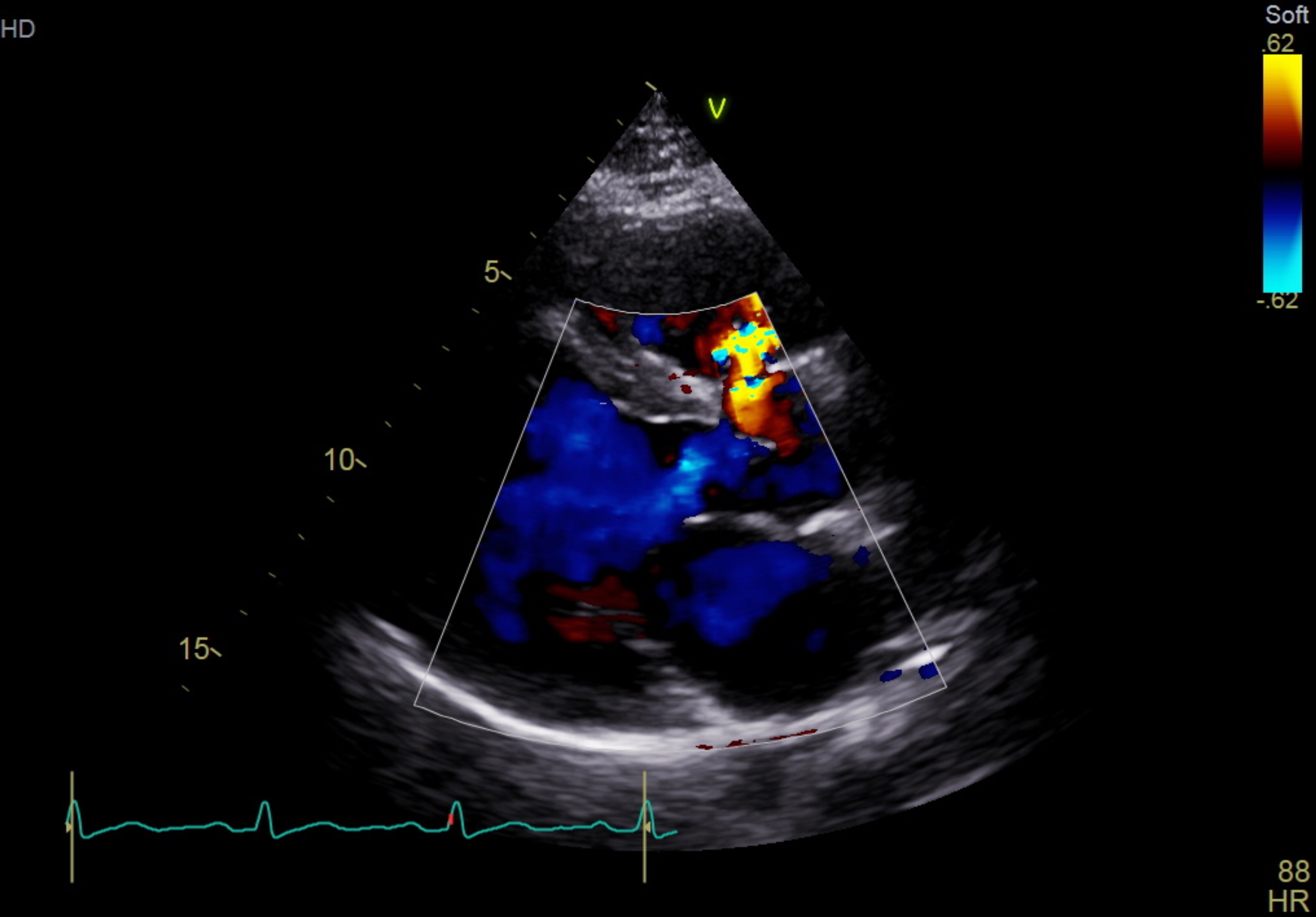
 PLAX CFM.mp4
PLAX CFM.mp4
PSAX CFM.mp4
Relevant Catheterization Findings
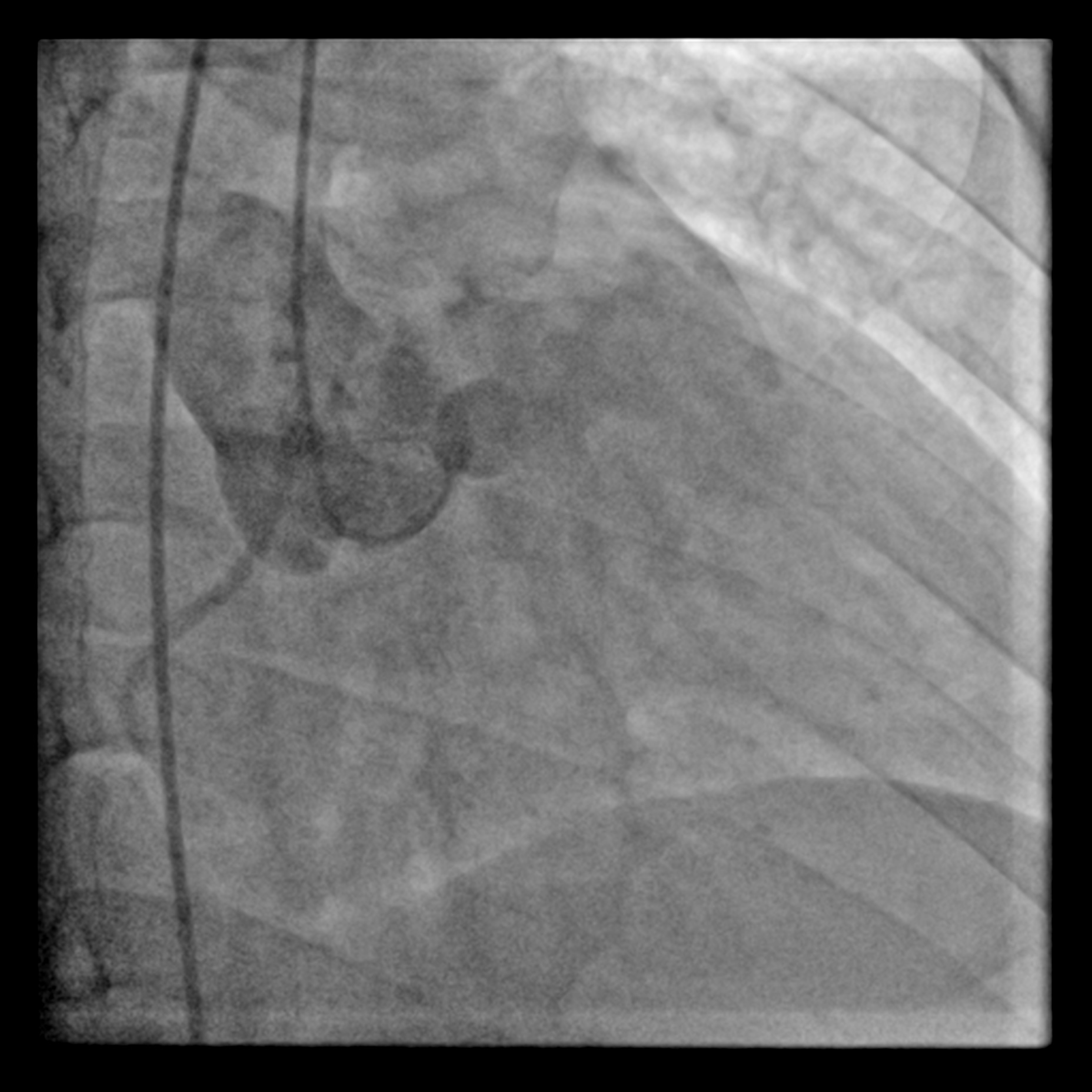
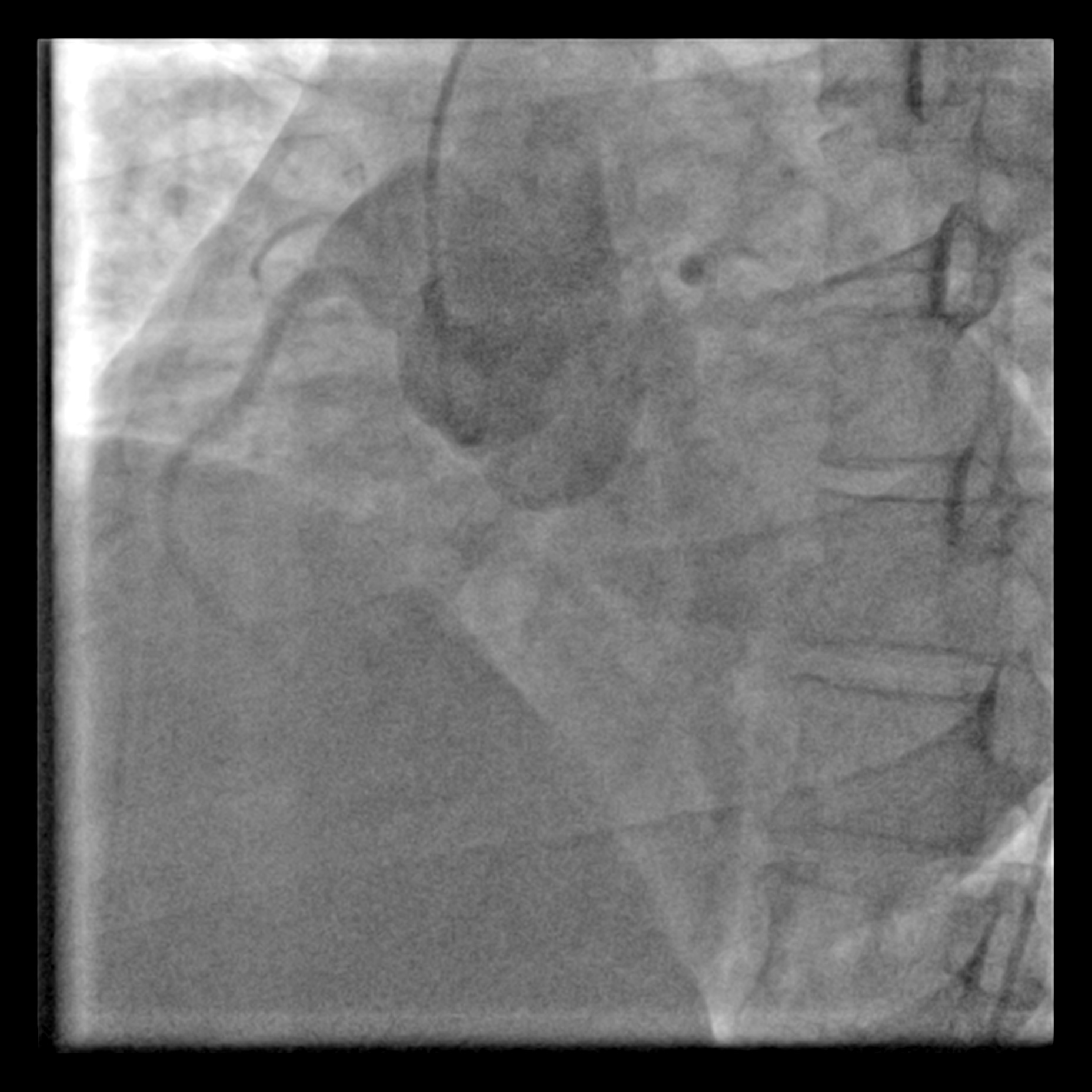
Via right femoral arterial access, a pigtail catheter was placed in SOV & non selective shot was taken with injector 2 views were used: left anterior and right anterior oblique view were taken to delineate the shunt. Right heart catheterisation was not perform in view of absence of pulmonary hypertension albeit left ventricle is dilated from echocardiography.
LAO.mp4
RAO.mp4
Interventional Management
Procedural Step
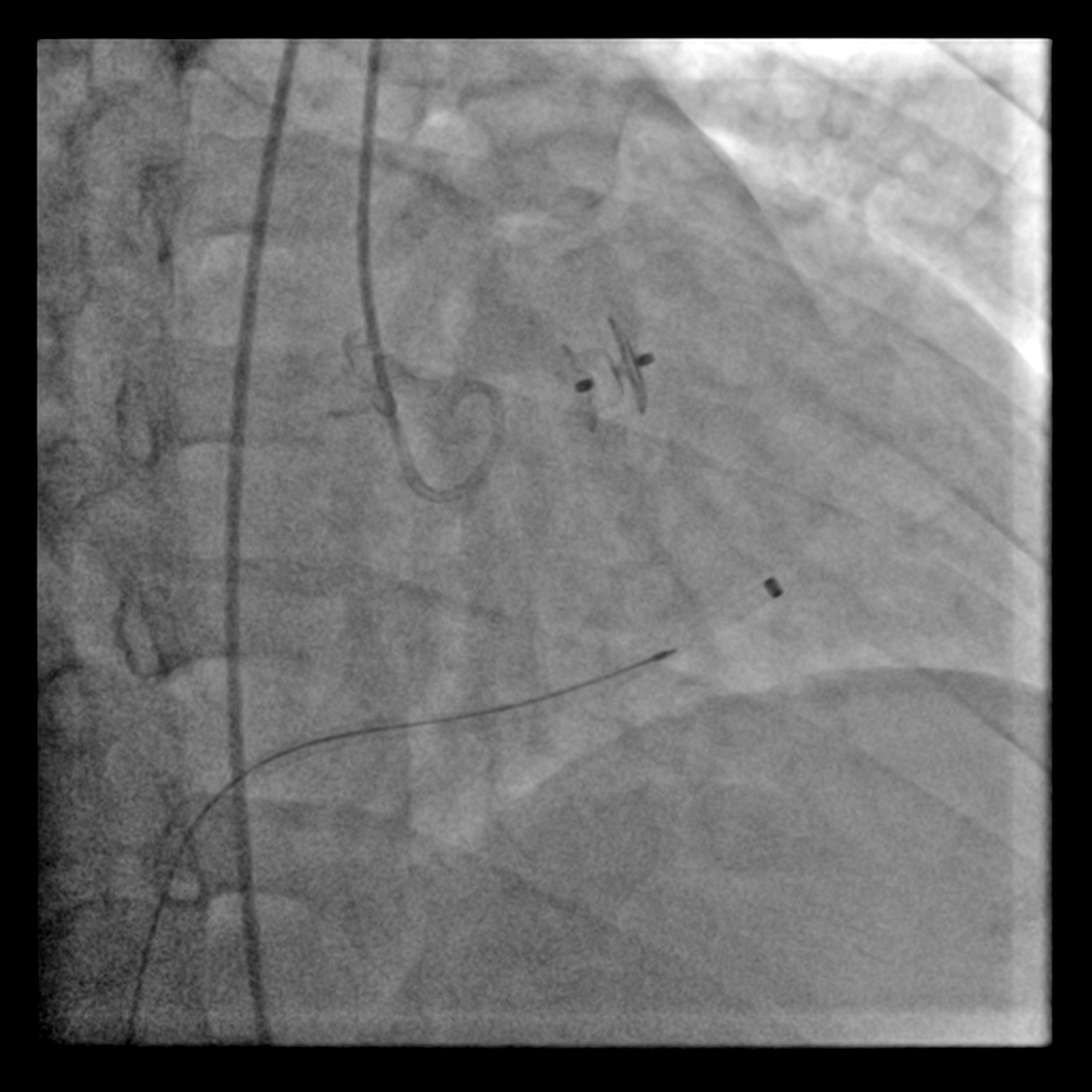
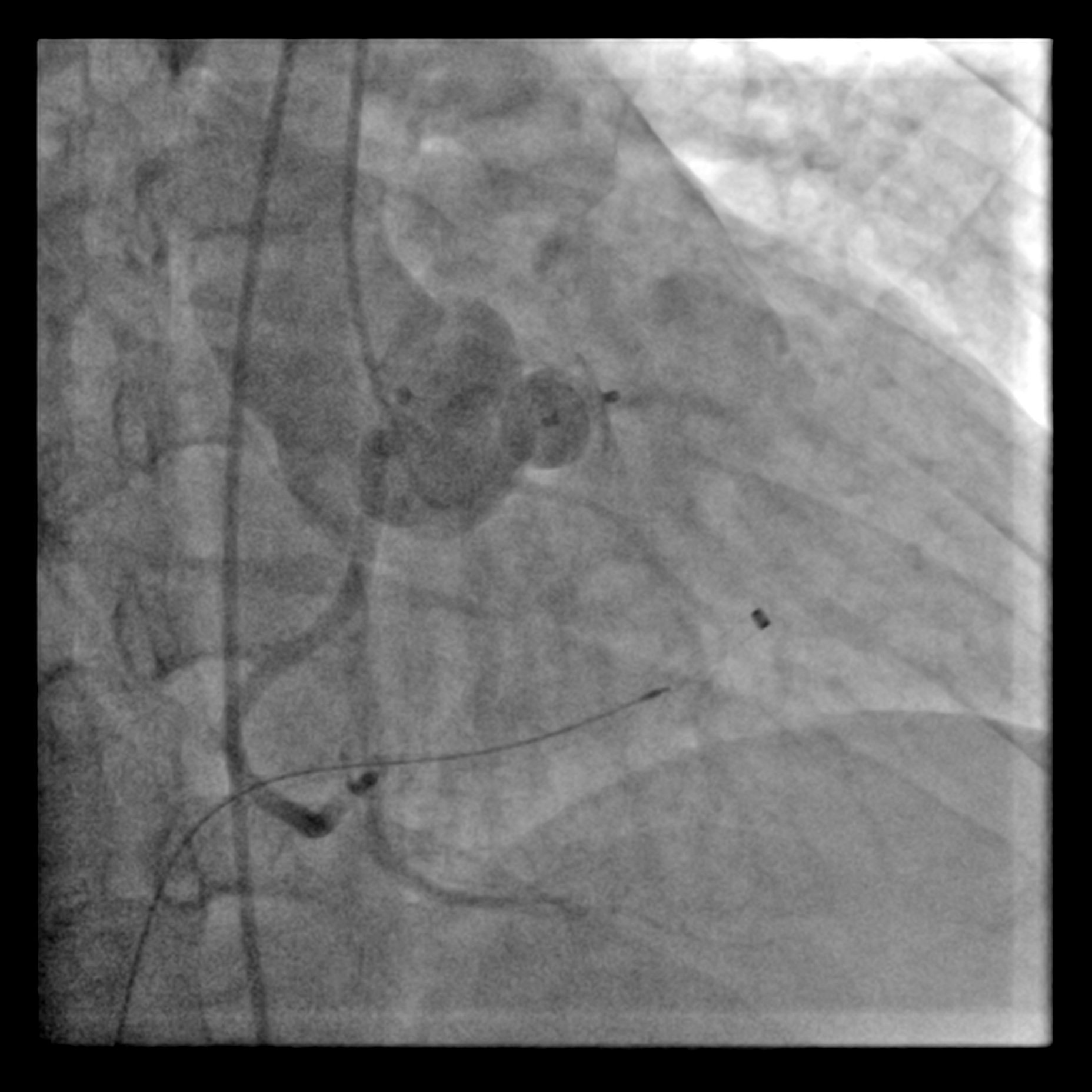
The procedure was commenced with one 7Fr sheath in right femoral vein & one 6Fr sheath in right femoral artery. From arterial access, a diagnostic Judkins right (JR) catheter 6Fr was positioned in right SOV. The defect was crossed with J-tipped Glidewire & subsequently advanced into right pulmonary artery. A Multipurpose (MPA) catheter was introduced via right femoral access & advanced into right pulmonary artery where the Glidewire was snared & externalised through the venous access. This created an arteriovenous wire loop. The delivery sheath was advanced over this loop wire, through the venous access, crossing the SOV's defect & positioned in ascending aorta. A 10-8mm KONAR-MFO VSD occluder (Lifetech) was smoothly deployed antegradely but left unreleased. A repeated non-selective aortogram was made with Pigtail catheter in ascending aorta confirmed preserved right coronary flow was & absence of aortic regurgitation. A trans-thoracic echocardiography confirmed the stable position & good defect sealing. The aortic valve demonstrated normal mobility without evidence of aortic stenosis & regurgitation. The occluder was then released under fluoroscopic guidance.
wiring of defect.mp4
snaring of Glidewire.mp4
Final shot.mp4
Case Summary
In case like this, involving an isolated, small defect without associated significant aortic regurgitation, percutaneous closure is considered superior over surgical repair due to its minimally invasive nature. The deivces used for this procedure can be ventricular septal defect or patent ductus arteriosus. One of the potential complication of this procedure is the coronary artery's ostium occlusion by the device's disc. This underscores the critical importance of meticulous peri-procedural imaging to mitigate the risk. Another potential complication is device's interference with the leaflet of aortic valve. Aortic stenosis & regurgitation must be excluded before releasing the device.