Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251102_019
Complex Anatomy, High Stakes: Unprotected Left Main With Three-Vessel Disease
By Hsin-Hui Chen, Yen-Lien Chou
Presenter
Hsin-Hui Chen
Authors
Hsin-Hui Chen1, Yen-Lien Chou1
Affiliation
Tri-Service General Hospital, National Defense Medical University, Taiwan1
View Study Report
CASE20251102_019
Coronary - Complex PCI - Calcified Lesion
Complex Anatomy, High Stakes: Unprotected Left Main With Three-Vessel Disease
Hsin-Hui Chen1, Yen-Lien Chou1
Tri-Service General Hospital, National Defense Medical University, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
A 73-year-old woman with a long-standing history of hyperlipidemia presented with chest tightness that worsened following an episode of emotional stress after an argument with her husband three months ago. She denied smoking or alcohol consumption. Her family history was notable for hypertension in both parents and all six siblings. A physical examination revealed regular heartbeats without significant murmurs and no pitting edema in the lower limbs.
Relevant Test Results Prior to Catheterization
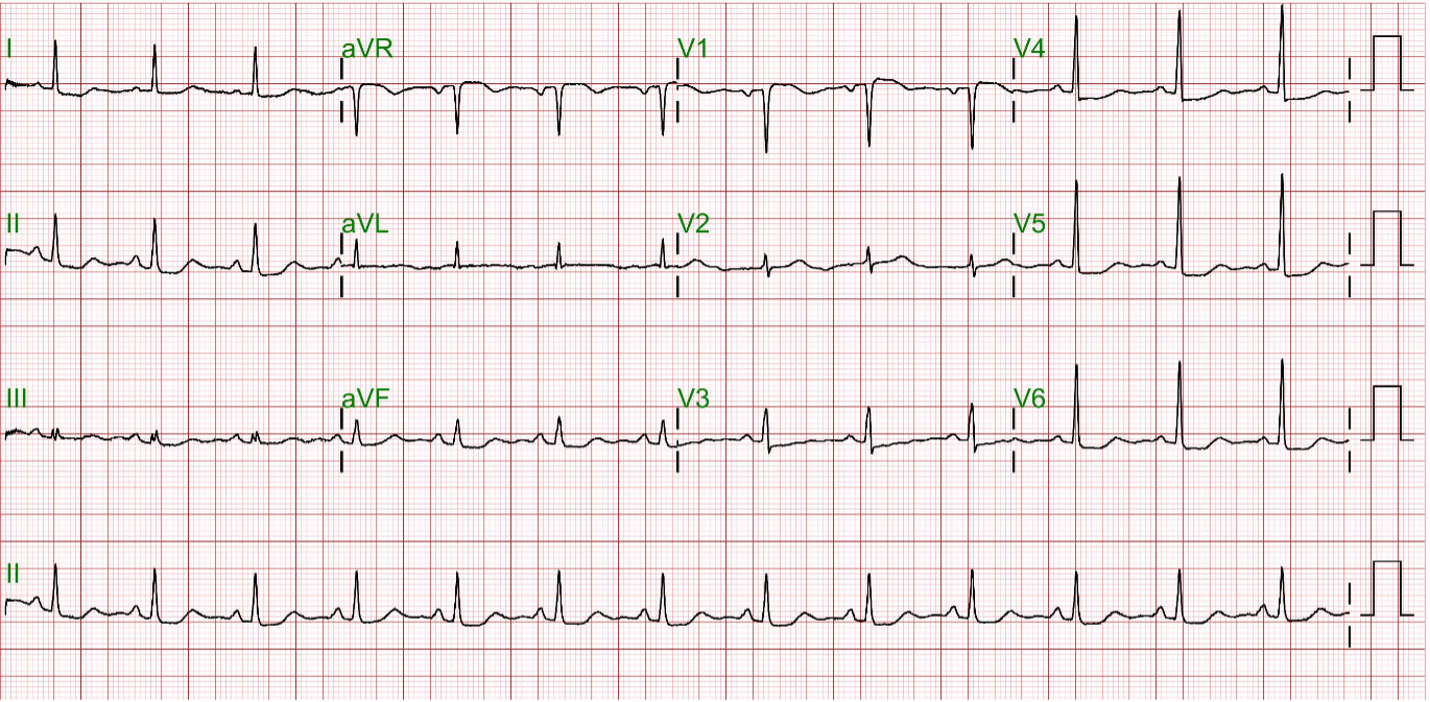
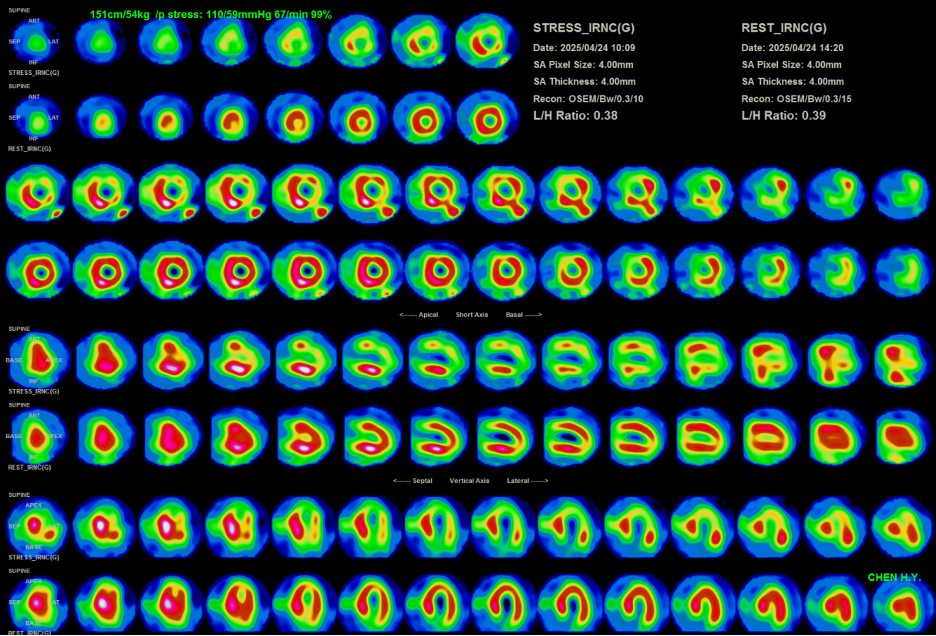
Laboratory studies revealed low-density lipoprotein cholesterol (LDL-C) 146 mg/dL, total cholesterol 230 mg/dL, and hemoglobin A1c 5.8%. Electrocardiography demonstrated normal sinus rhythm with diffuse ST-segment depression in leads II, III, aVF, and V4–V6. Transthoracic echocardiography showed a preserved ejection fraction of 60%. Thallium-201 myocardial perfusion imaging suggested significant coronary artery disease involving the left anterior descending and left circumflex arteries
Relevant Catheterization Findings
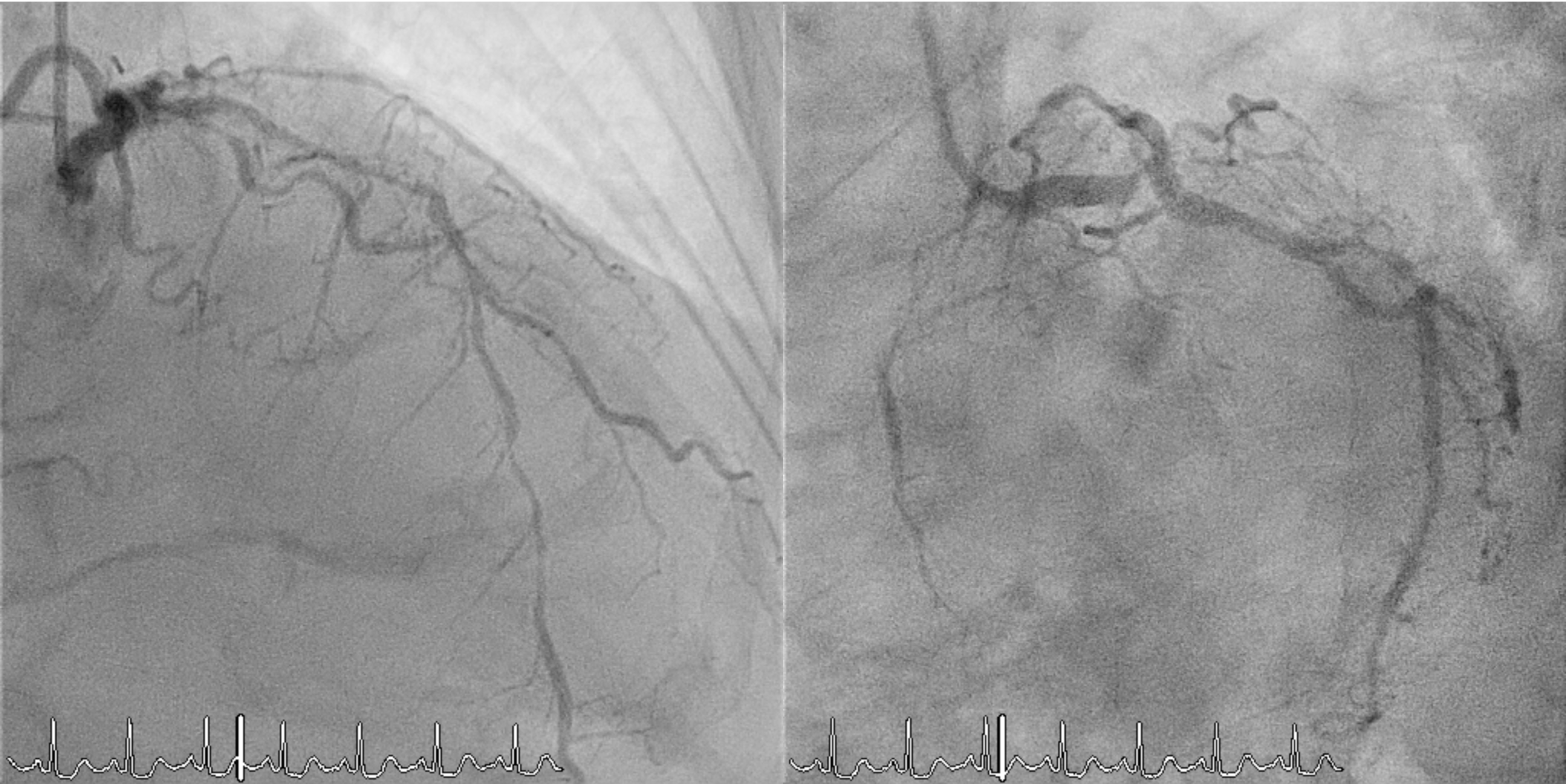
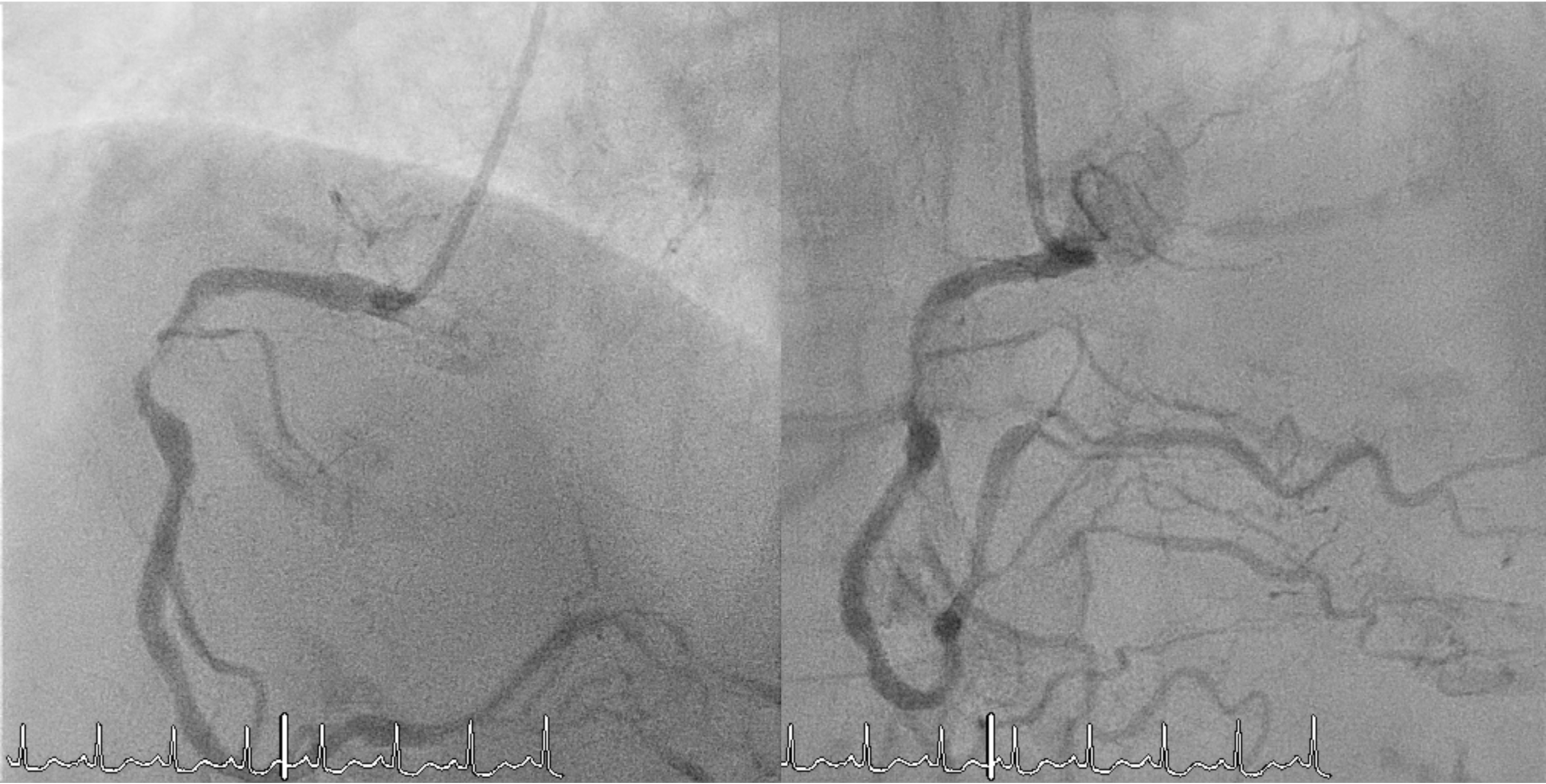
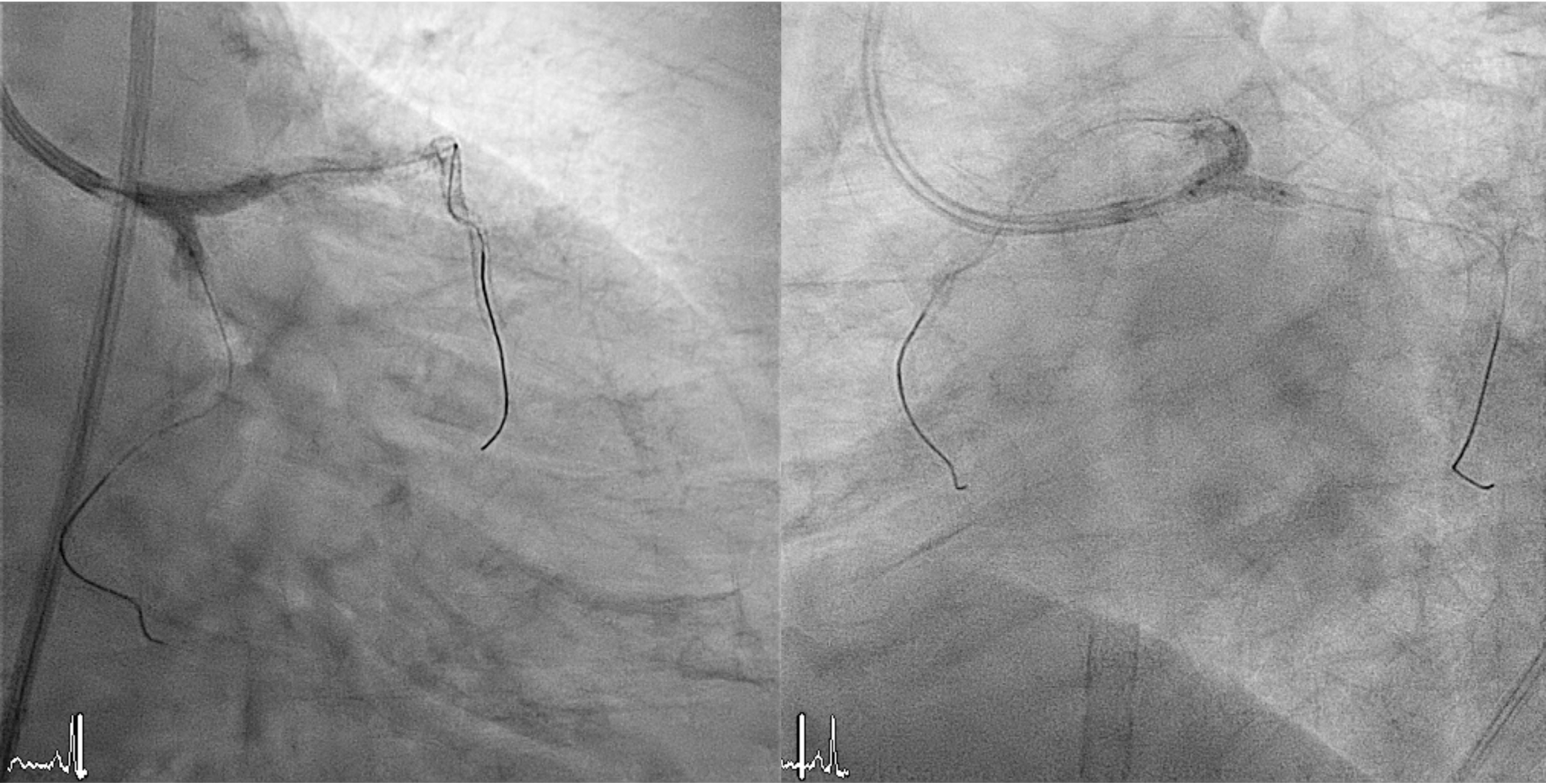
Coronary angiography revealed complex multivessel disease, with a syntax score of 42 points. The LMCA had a distal 95% eccentric lesion (Medina 1,0,0). The LAD showed diffuse disease with 70% stenosis proximally and 80% distally. The LCx had a proximal 90% and mid–distal diffuse 90% stenosis, with the OM showing a 70% proximal–mid lesion. The RCA had a proximal 85% and mid–distal 60% stenosis, and the small PDA had an 80% proximal lesion.
 0502_02A.mp4
0502_02A.mp4
0502_02B.mp4
0502_04B.mp4
Interventional Management
Procedural Step
1. Prophylactic mechanical circulatory support with extracorporeal membrane oxygenation (ECMO) was initiated in response to a complex high-risk PCI case that had a high BCIS Jeopardy Score of 12 points.2. Arterial access was obtained via the right femoral artery. A 7 Fr EBU 3.5 guiding catheter was used for the left coronary system, and a 6 Fr JR 3.5 catheter for the right.3. Intravascular ultrasound (IVUS) evaluation revealed long, circumferential calcification with a small luminal area in the LAD (MLA= 2.43mm2), and a prominent calcium nodule extending from the left main to the LCx (MLA= 2.52mm2).4. Owing to severe calcification and an undilatable lesion in the LAD, rotational atherectomy from the proximal to mid segment was performed using a 1.25-mm burr, followed by cutting balloon angioplasty.5. Intravascular lithotripsy (IVL, 3.0 mm) was performed on the proximal LCx and left main bifurcation, combined with cutting balloon angioplasty.6. Double-kissing (DK) crush stenting technique was applied at the left main bifurcation for complex lesion management.7. Finally, three drug-eluting stents (DES) were implanted in the LAD, one in the LCx, and one in the RCA.


22A.mp4
213A.mp4
213B.mp4
Case Summary
This case illustrates the management of complex, heavily calcified coronary artery disease involving an unprotected left main bifurcation and three-vessel disease. Effective lesion preparation with rotational atherectomy and intravascular lithotripsy achieved adequate calcium modification and stent expansion. The DK-crush technique provided optimal results for the left main bifurcation. In patients with extensive calcification, high SYNTAX scores, and hemodynamic risk, prophylactic mechanical circulatory support such as ECMO should be considered to ensure procedural safety during high-risk PCI.