Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251102_018
When the True Lumen Disappears: Salvage Dilemma After Subintimal Stenting in Diffuse LAD Disease
By Jin Kiang Cheng, Waye Young Lau, Wee Pang Ng, Vicknesan Kulasingham
Presenter
Jin Kiang Cheng
Authors
Jin Kiang Cheng1, Waye Young Lau1, Wee Pang Ng1, Vicknesan Kulasingham1
Affiliation
Hospital Sultanah Aminah Johor Bahru, Malaysia1
View Study Report
CASE20251102_018
Coronary - ACS/AMI
When the True Lumen Disappears: Salvage Dilemma After Subintimal Stenting in Diffuse LAD Disease
Jin Kiang Cheng1, Waye Young Lau1, Wee Pang Ng1, Vicknesan Kulasingham1
Hospital Sultanah Aminah Johor Bahru, Malaysia1
Clinical Information
Relevant Clinical History and Physical Exam
A 62-year-old Malay male, active smoker, diabetic mellitus, dyslipidemia, ischemic heart disease presented with unstable angina. Previous month Myocardial perfusion scan showed infarction involving the RCA and LCx territories. He was scheduled for emergency coronary angiography. Clinically, the patient had resolved chest pain, haemodynamically stable. Cardiovascular examination revealed a dual rhythm with no murmurs, and pulmonary examination showed equal.
Relevant Test Results Prior to Catheterization
• ECG: Sinus rhythm, heart rate 75 bpm • Echocardiogram: Preserved left ventricular function (EF 55%) with mild regional wall motion abnormalities in RCA and LCx territories. • MPS: Infarcted RCA and LCx territories, viable anterior wall.
Relevant Catheterization Findings
Coronary Angiography Findings
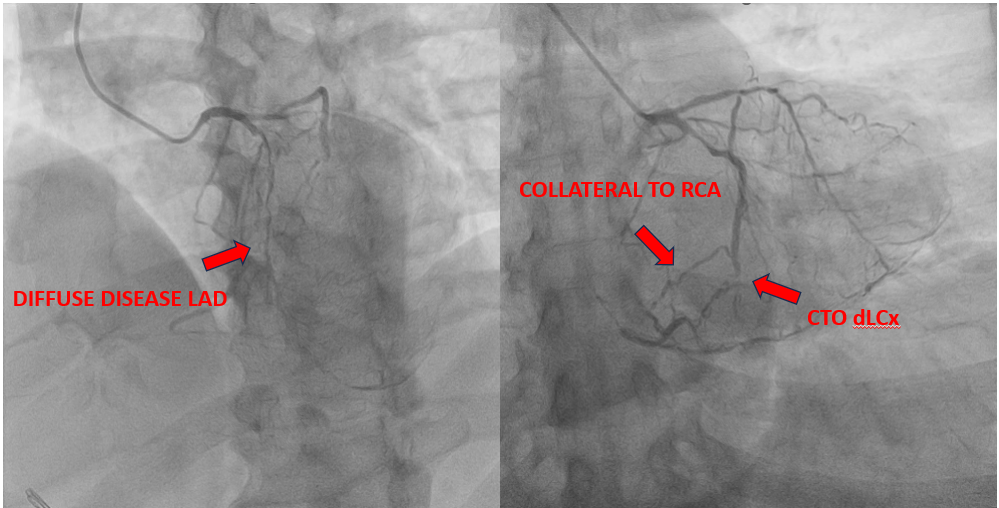
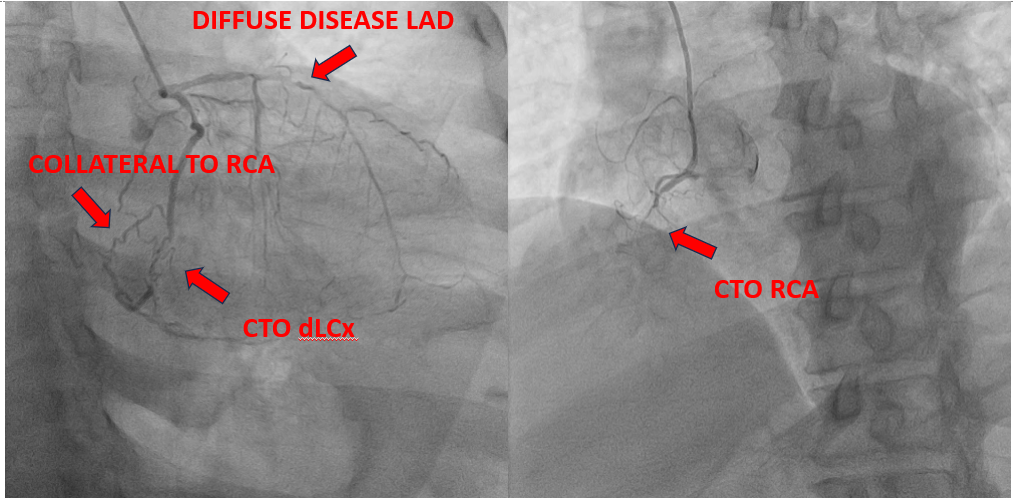
• The LM coronary artery was normal.
• The LAD artery showed diffuse severe disease with approximately 99% stenosis extending from the proximal to distal segment.
• The RCA was completely occluded, with collateral flow observed from the mid LCx to the RCA.
• The distal LCx was completely occluded.
• Collateral circulation from the mid LCx supplied the right coronary territory.
Interventional Management
Procedural Step
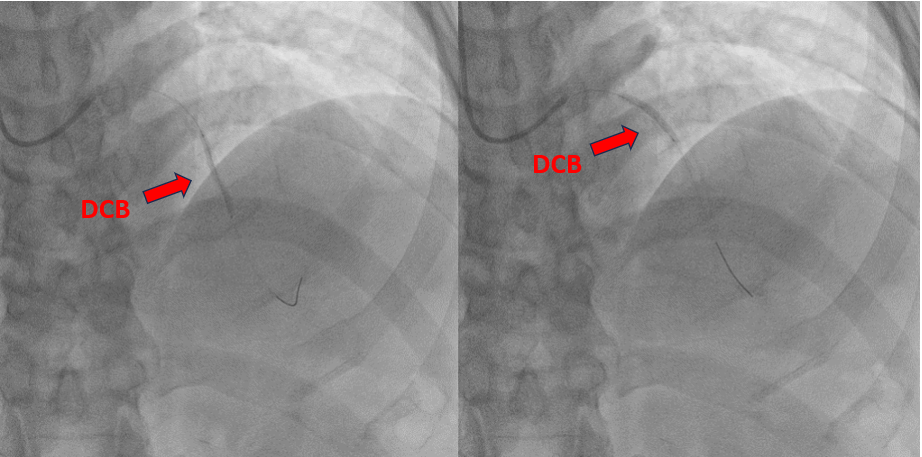
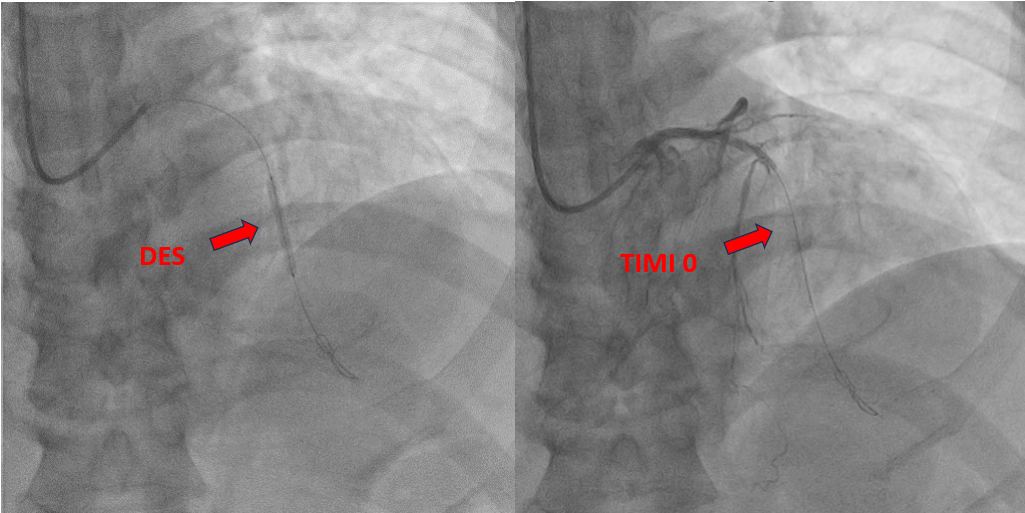
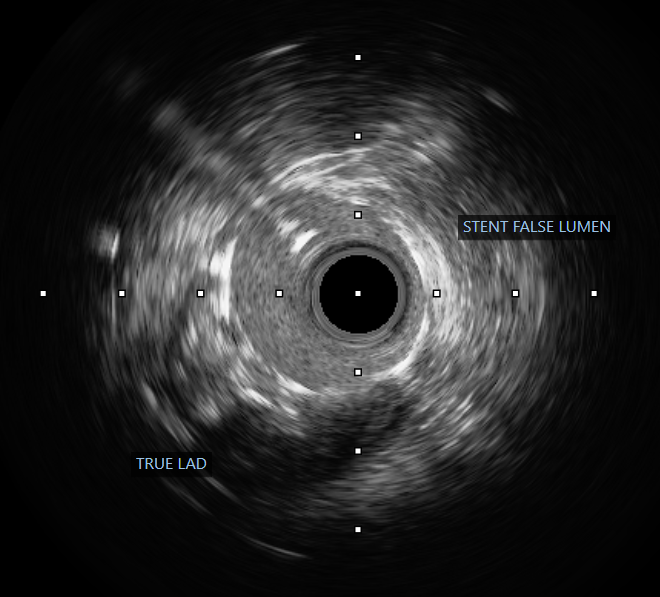
The procedure was performed via a 6 French femoral approach. The LAD was wired using a BMW guidewire and pre-dilated sequentially with non-compliant balloons sized 2.5 × 15 mm and 3.0 × 15 mm, achieving satisfactory lumen expansion. Considering the diffuse nature of the lesion, a DCB-only strategy was selected to avoid multiple overlapping stents. DCB angioplasty was carried out, sized 2.5 × 30 mm and 3.0 × 25 mm, each inflated for 60 seconds. The final angiogram revealed mild vessel recoil and a non–flow-limiting dissection with TIMI 3 flow. To optimize the result, the operator attempted re-wiring for bailout stenting; however, the guidewire inadvertently entered a false lumen. Despite this, pre-dilatation was performed followed by deployment of a 2.5 × 26 mm Onyx drug-eluting stent from the mid to distal LAD. Subsequently, the vessel flow deteriorated to TIMI 0. Intravascular ultrasound confirmed subintimal stent placement with a long false lumen extending from the mid LAD before the septal branch. Multiple attempts to re-enter the true lumen, both proximally and distally, were unsuccessful. The patient developed chest discomfort, which was partially relieved with morphine. In view of persistent LAD occlusion, intra-aortic balloon pump (IABP) support was initiated for hemodynamic stabilization, and the patient was referred for urgent coronary artery bypass grafting (CABG).
 post dcb.mp4
post dcb.mp4
false lumen rewiring.mp4
post stenting.mp4
Case Summary
In patients undergoing DCB-only angioplasty, careful post-procedure assessment is essential. Non–flow-limiting dissections can be accepted when flow is preserved, and patient asymptomatic , as premature re-intervention may precipitate catastrophic complications. In cases requiring additional wiring or stenting, intravascular imaging should be used to confirm true lumen position and guide intervention safely. Once subintimal stenting occurs, percutaneous re-entry is technically demanding and often unsuccessful; thus, early recognition and timely surgical referral offer the best chance of myocardial salvage.