Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251102_014
Something Disappeared: An Unexpected Event in a Left Atrial Appendage Closure Case
By Jing-Han Yao, Bing-Han Luo
Presenter
Jing-Han Yao
Authors
Jing-Han Yao1, Bing-Han Luo1
Affiliation
China Medical University Hospital, Taiwan1
View Study Report
CASE20251102_014
Structural - LAAO
Something Disappeared: An Unexpected Event in a Left Atrial Appendage Closure Case
Jing-Han Yao1, Bing-Han Luo1
China Medical University Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
The patient is a 68-year-old female with past histroy of bronchiectasis, paroxysmal atrial fibrillation, type 2 DM and hypertension. She was prescribed with Dabigatran for stroke prevention. However, she presented hemoptysis since this January. Bronchoscopy revealed no source of active bleeding and her hemoptysis recurred after adding back the NOAC. Physical examination showed lung fine crackles, regular pulses now without other remarkable findings. She was admiited for LAA closure.
Relevant Test Results Prior to Catheterization
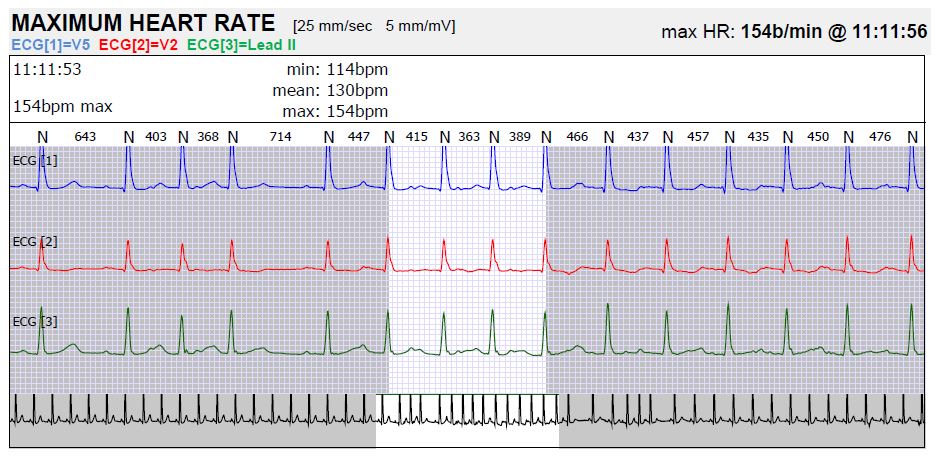
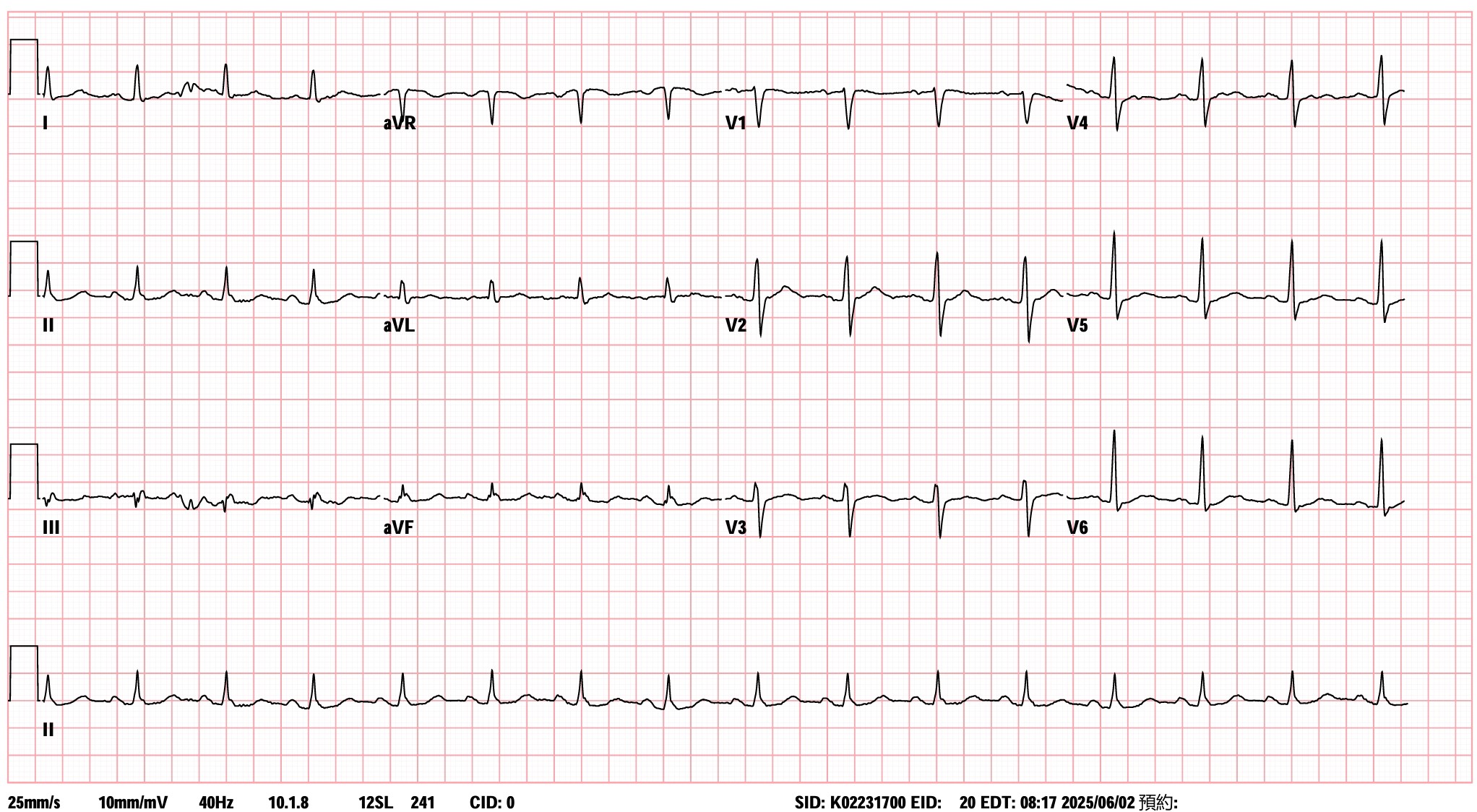
12-Leads EKG: Normal sinus rhythm
24 Holter's Scan: The basic rhythm was sinus in origin. Episodes of paroxysmal Af were noted.
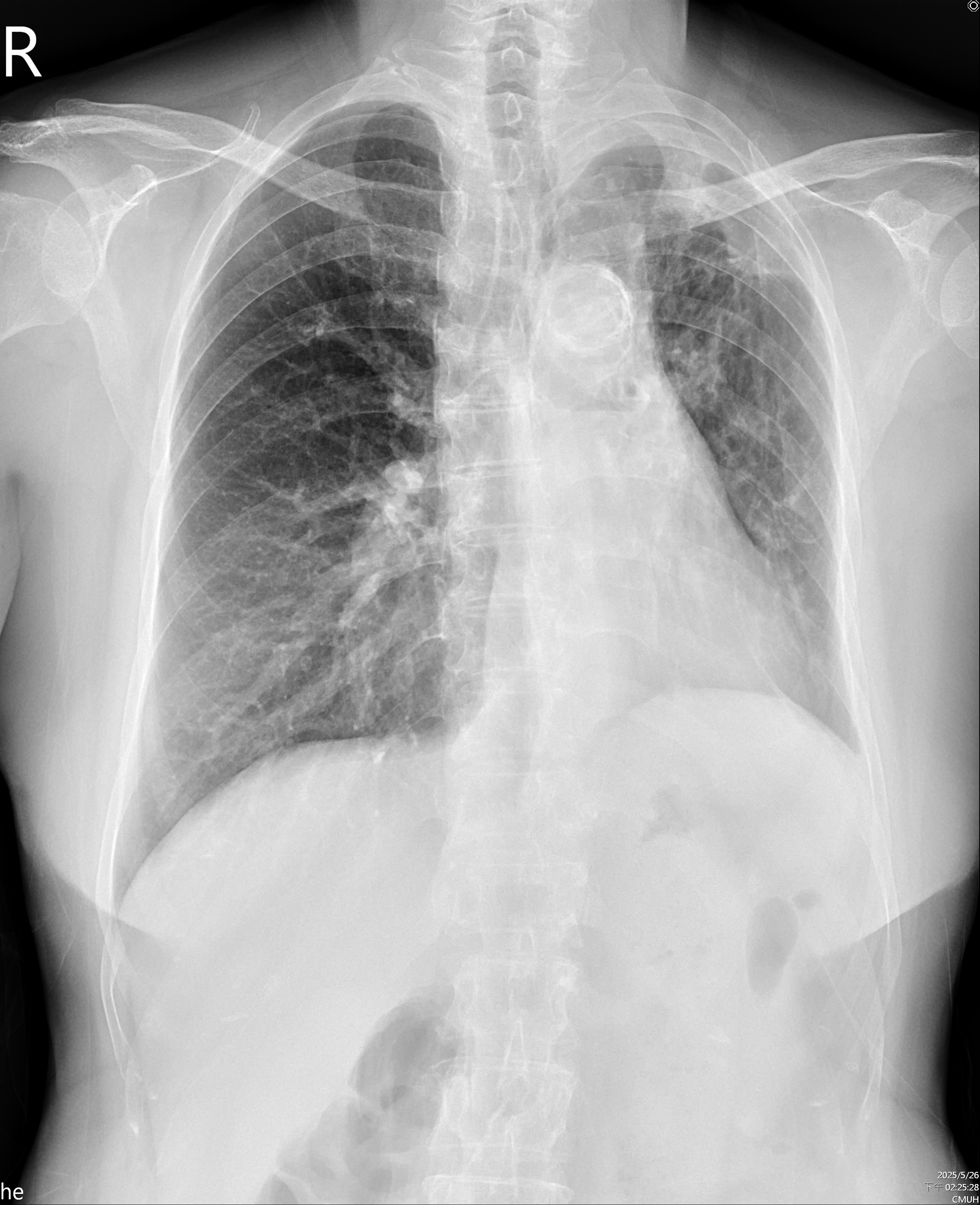
CXR: Tortuosity of the T-aorta without cardiomegaly, Calcification of aortic arch, bronchiectasis in both lower lungs.
Transthoracic Echocardiography: Preserved left ventricular ejection fraction, Normal right-sided size
Lab Tests: WBC: 6900/uL, Hb: 12.6 g/dL, Platelet: 241000/uL, Cr: 0.53 mg/dL, Na: 144 mmol/L, K: 3.5 mmol/L, PT: 12.9 sec, INR: 1.08, APTT: 39.7 sec
Relevant Catheterization Findings
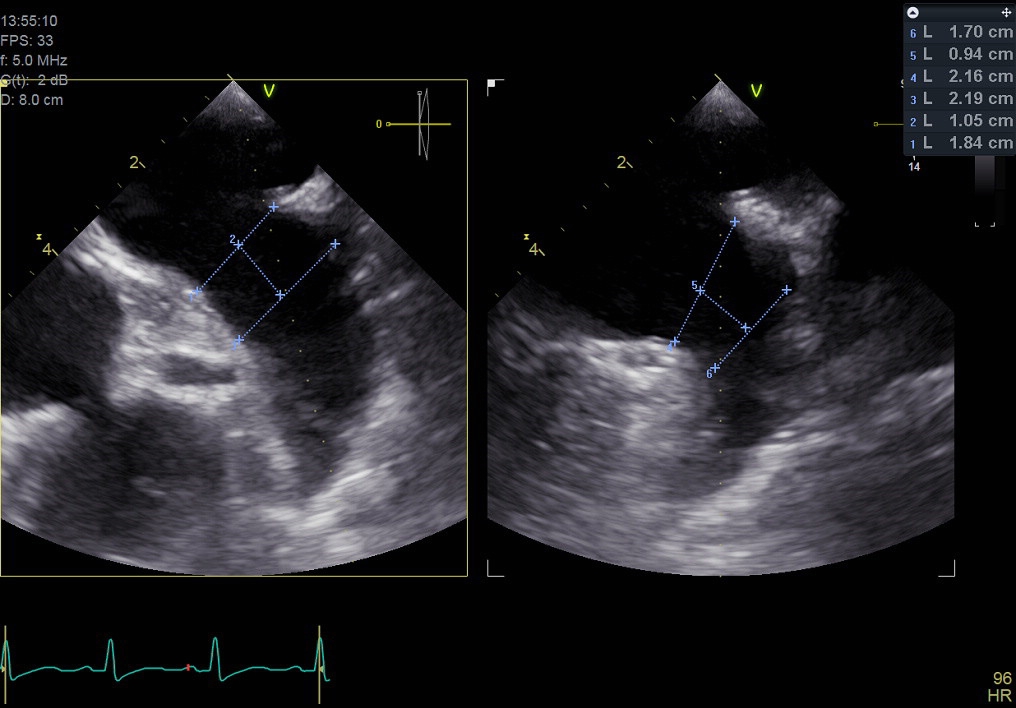
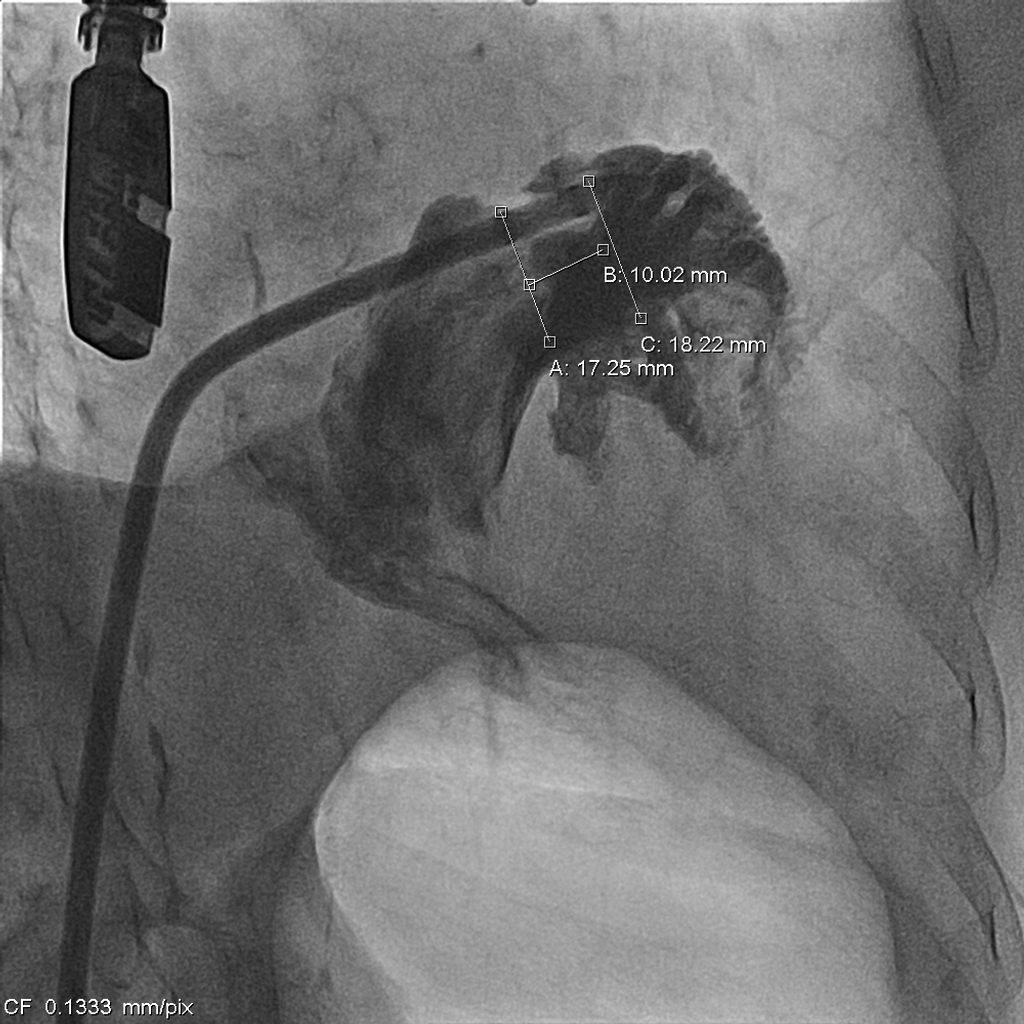
Coronary artery angiography showed only mild atheroscleorosis of left and right coronary arteriesWe used periprocedure transesophageal echocardiography to measure the size of left atrial appendage and we are going to place Lambree LAA closure systemTransseptal puncture was performed smoothly. LAA angio revealed ostial diameter was 17.3-25.3mm (diastole, systole). Landing zone diameter was 18.2-20.7mm.
 LAA Cine.mp4
LAA Cine.mp4
0527 LCA.mp4
0527 RCA.mp4
Interventional Management
Procedural Step
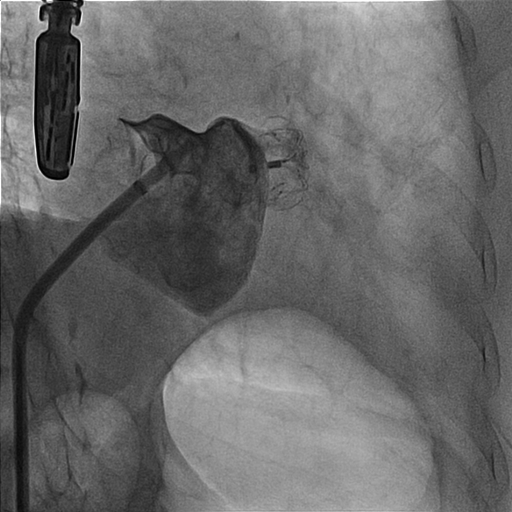
1. We made right femoral vein puncture and inserted 8 Fr sheath. Then we advanced the SL0 catheter to atrial septum.2. We used BRK transeptal needle to perform transeptal puncture under TEE guidance and advanced the dilator and SL0 catheter.3. The LAAO size was chosen under TEE and under angiography and we selected the 20/26 mm Lambre LAA Closure System (Lifetech Scientific).4. We deployed the LAA occlude. But the position of the LAAO changed soonly and unstable after the deployment under angiography and TEE view. (Image 1) (Video 1) 5. The procedure was going to be closed. However, the LAAO disappeared under the TEE view and dislodged to the aortic arch at the next moment. 6. SJM 12 Fr sheath (Abbott) was inserted through right femoral artery and we chose a JR4 8 Fr. guiding catheter. We used the JR4 to crush the LAAO at first.7. Then we used the AndraSnare (Andramed) to catch the device and pulled it to the opening of the right femoral sheath.8. It was stuck at the orifice of the sheath and kinked so that we changed to larger bore Gore sheath 24F.(Image 2)9. We used Conger GW 0.035 260cm to pass through the LAAO. And then ev3 Goose Snare 10mm 4.5Fr. (Medtronic) was used to grab the wire and LAAO together. We finally made extraction of the LAAO. (Video 2)(Image3)10. The final right common femoral artery angiography showed no contrast medium extravasation.11. The second LAAO was deployed successfully by using the Watchman Pro 27mm system (Boston Scientific).(Video 3)


Video 1 unstable LAAO.mp4
Video 2- LAAO extraction.mp4
Video 3 - 2nd LAAO.mp4
Case Summary
The accurate measurement of the left atrial appendage (LAA) size and choosing the appropriate size of the occluder is the main learning point of the case. Not only the size of the LAA matters but also the morphology influences the success of LAA deployment. Different sizes and shapes of the LAAOs are suitable for different conditions. The other important implication of this case is the management of the LAAO dislodgement. Besides the endovascular method, surgical extraction should be considered as the last resort. Using the catheter for extraction may cause intravascular injury, possible embolic events and the large bore arterial sheath may sacrifice the blood supply to the lower limbs.