Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251102_008
Heart Failure From a Large Coronary Artery Fistula Treated With Dual-Plug Transcatheter Closure
By ShuFan Deng
Presenter
ShuFan Deng
Authors
ShuFan Deng1
Affiliation
National Taiwan University Hospital, Taiwan1
View Study Report
CASE20251102_008
Endovascular - Other Endovascular Interventions
Heart Failure From a Large Coronary Artery Fistula Treated With Dual-Plug Transcatheter Closure
ShuFan Deng1
National Taiwan University Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
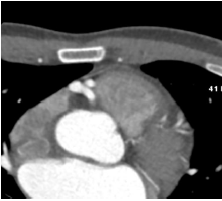
A 40-year-old man presented to the ER with 4 months of progressive dyspnea on exertion and bilateral lower-extremity pitting edema. He had no medical history. EKG-gated computed tomography revealed reduced ejection fraction and a large right coronary artery–to–pulmonary artery fistula. Diuretics improved his symptoms. Examination showed a pansystolic murmur at the left upper sternal border and 1+ pitting edema. He was referred to our hospital for fistula and heart failure management.
Relevant Test Results Prior to Catheterization
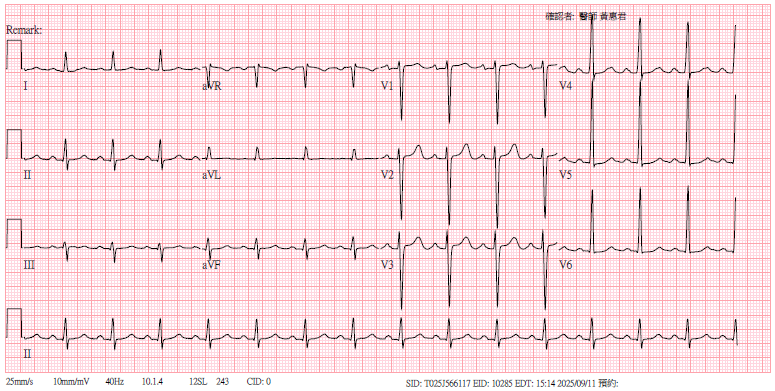
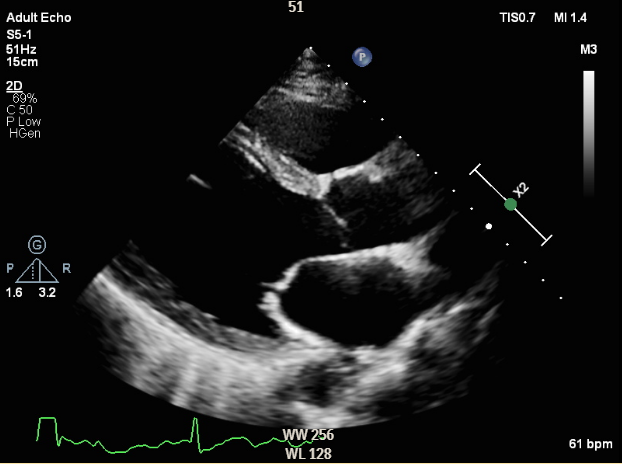
Electrocardiography showed normal sinus rhythm with left ventricular hypertrophy. Chest X-ray revealed borderline cardiomegaly and prominent pulmonary vasculature. Transthoracic echocardiography demonstrated a dilated left ventricle with a severely reduced ejection fraction of 32.7%. Laboratory tests showed elevated NT-proBNP (351.2 pg/mL), normal blood counts, preserved renal and hepatic function, and HbA1c of 6.1%.
Relevant Catheterization Findings
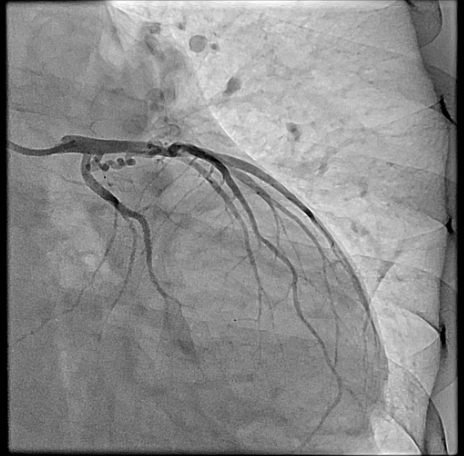
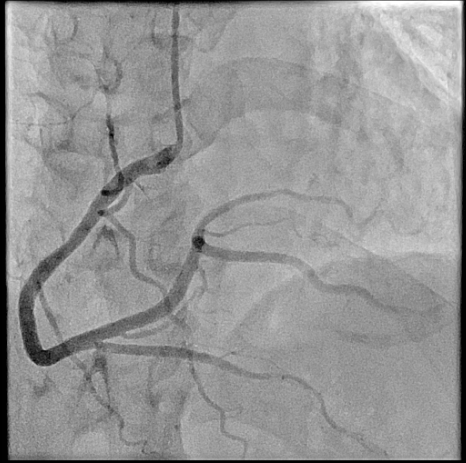
Right heart catheterization revealed a pulmonary capillary wedge pressure of 19 mmHg and mean pulmonary artery pressure of 47/27 mmHg. Pulmonary vascular resistance was 3.06 Wood units, with cardiac output of 4.9 L/min and Qp/Qs ratio of 1.24. Coronary angiography showed patent left main, LAD, and circumflex arteries. A small proximal LAD fistula and a large RCA fistula, both draining into the pulmonary artery, were identified.
Interventional Management
Procedural Step
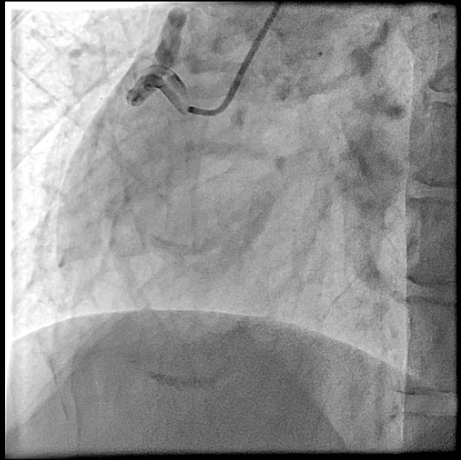
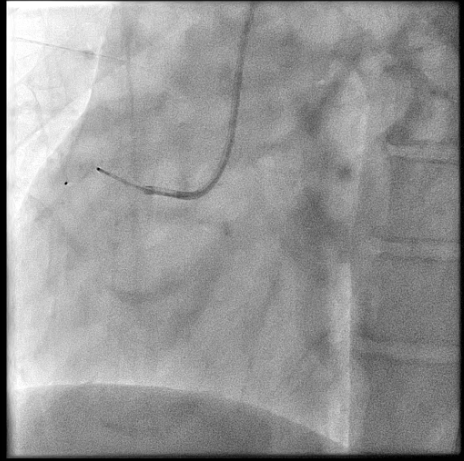
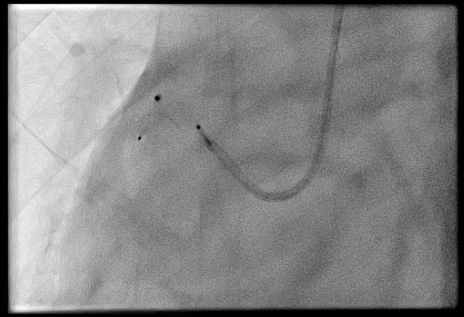
The procedure was performed via left radial artery access. The right coronary fistula was engaged with a 6F AL1 guide catheter. A 5F microcatheter advanced an ASAHI Sion Black wire into the fistula tract. Given the fistula’s large size and high flow, a two-device closure strategy was employed. A 7-mm AMPLATZER Vascular Plug 4 was initially deployed proximally, achieving partial flow reduction. To ensure complete occlusion, an 8-mm AMPLATZER Vascular Plug was subsequently positioned at the ostium. Final angiography confirmed marked flow reduction in the fistula while preserving native RCA flow. The small LAD fistula was left untreated due to minimal shunting. The procedure was completed without complications, and radial hemostasis was achieved.

Case Summary
Large coronary arteriovenous fistula cause heart failure by chronic volume overload from left-to-right shunting. Transcatheter closure offers definitive treatment while avoiding surgical risks. In this case, a dual-plug technique achieved complete occlusion of a high-flow fistula without compromising coronary perfusion. Symptom resolution after the procedure, combined with guideline-directed medical therapy, underscores the importance of eliminating hemodynamic burden in fistula-related heart failure with reduced ejection fraction. This case supports percutaneous closure as a safe, effective strategy in selected patients.