Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251102_006
Successful Dual-Branch Revascularization for Unprotected Aorto-Ostial LMT CTO With Separated Bifurcation and No Retrograde Option Using Imaging-Guided Plaque Modification
By Hidenari Matsumura, Yuki Yamaguchi, Nobuhiro Yoshijima, Hiroaki Nishida, Erito Furuse, Takeshi Mori, Hiroyuki Yokota, Kenichiro Shimoji
Presenter
Hidenari Matsumura
Authors
Hidenari Matsumura1, Yuki Yamaguchi1, Nobuhiro Yoshijima1, Hiroaki Nishida1, Erito Furuse1, Takeshi Mori1, Hiroyuki Yokota1, Kenichiro Shimoji1
Affiliation
Saiseikai Utsunomiya Hospital, Japan1
View Study Report
CASE20251102_006
Coronary - Complex PCI - Left Main
Successful Dual-Branch Revascularization for Unprotected Aorto-Ostial LMT CTO With Separated Bifurcation and No Retrograde Option Using Imaging-Guided Plaque Modification
Hidenari Matsumura1, Yuki Yamaguchi1, Nobuhiro Yoshijima1, Hiroaki Nishida1, Erito Furuse1, Takeshi Mori1, Hiroyuki Yokota1, Kenichiro Shimoji1
Saiseikai Utsunomiya Hospital, Japan1
Clinical Information
Relevant Clinical History and Physical Exam
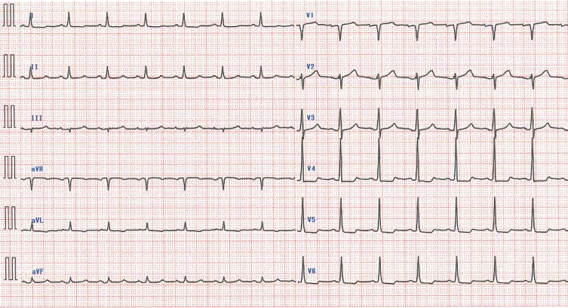
The patient was a 70-year-old man with a history of PCI to the right coronary artery and coronary artery bypass grafting using the Left Internal Thoracic Artery to the Left Anterior Descending artery (LITA–LAD). He had been stable on medical therapy, but developed exertional chest pain three months earlier. Despite medication adjustments, his symptoms gradually worsened, reaching Canadian Cardiovascular Society class II. The electrocardiogram showed nonspecific ST–T changes.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
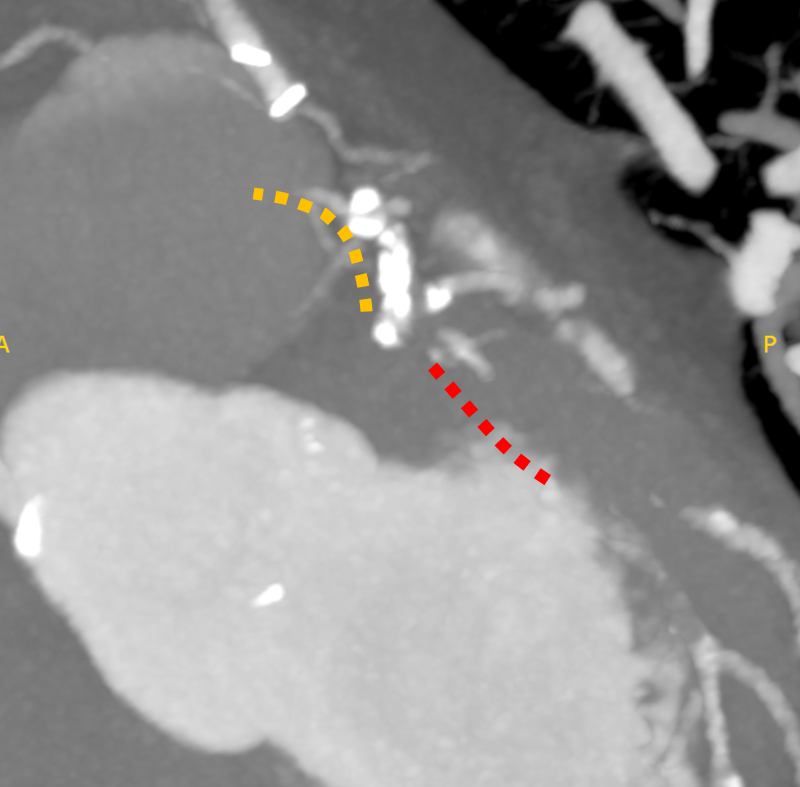
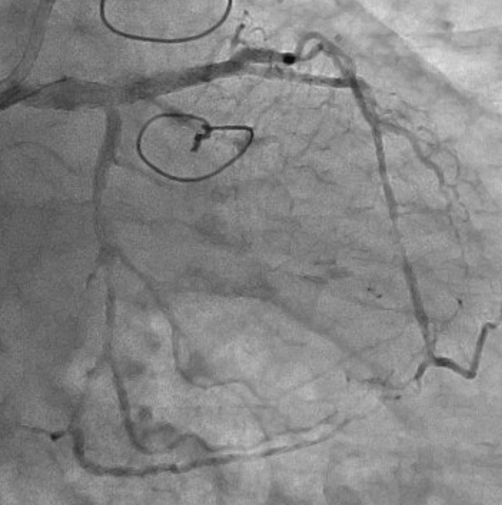
The left internal thoracic artery–left anterior descending artery (LAD) graft was completely occluded, and the native left coronary artery (LCA) was also occluded at the ostium of the left main trunk (LMT). The right coronary artery demonstrated no significant stenosis. From a right ventricular branch, non-interventional epicardial channels opacified the separated LAD and left circumflex artery. The occlusion length from the ostium of the long LMT to the bifurcation, was approximately 15 mm.
Interventional Management
Procedural Step
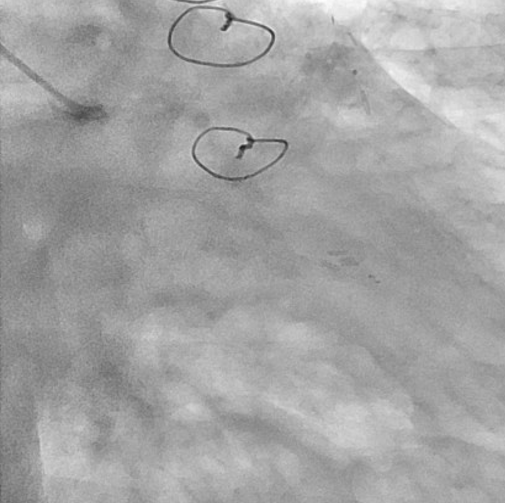
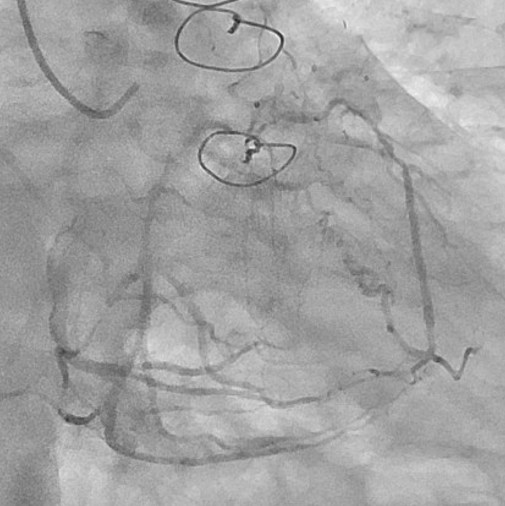
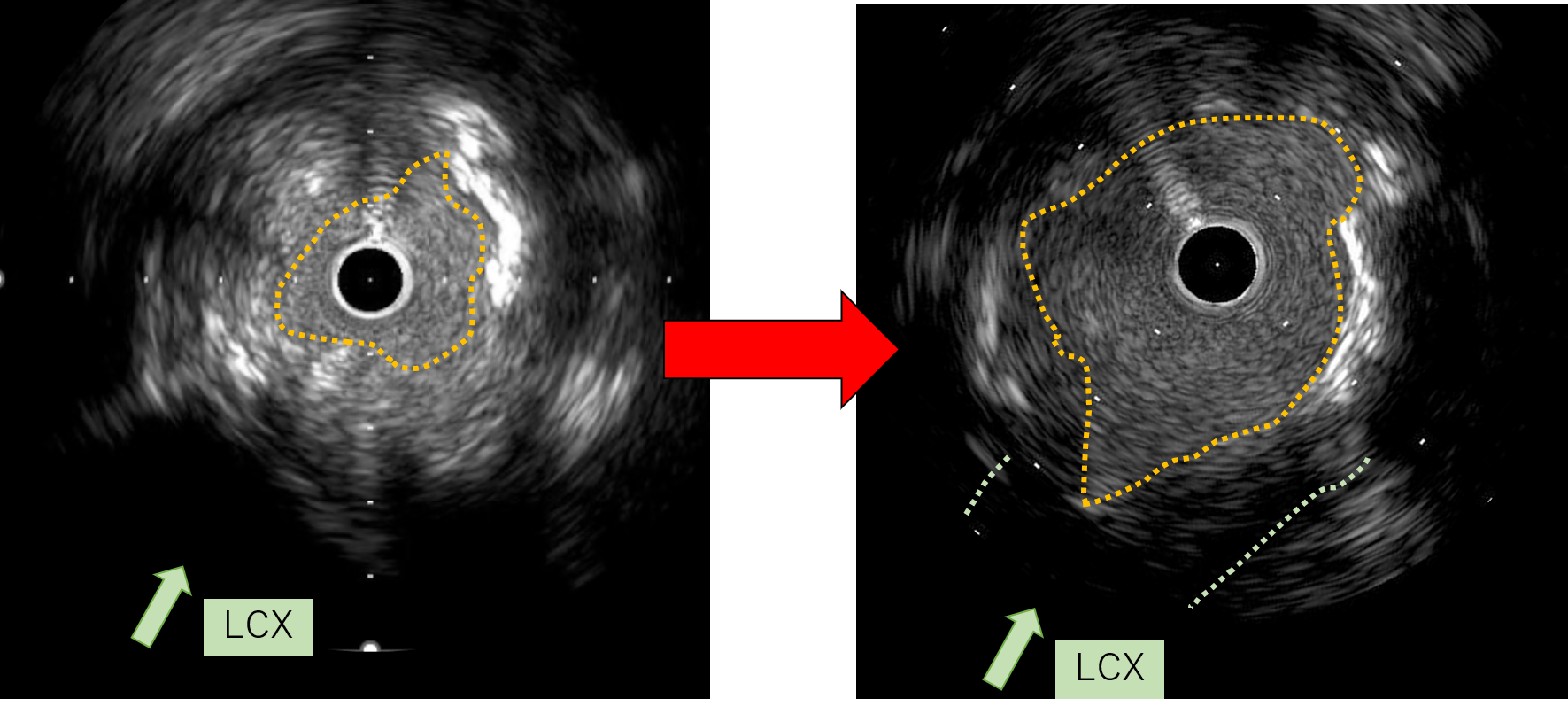
First, percutaneous coronary intervention (PCI) was performed toward the left anterior descending artery (LAD). The initial antegrade wire deviated from the true lumen; therefore, parallel wire technique was employed to achieve successful crossing. To avoid jailing the left circumflex artery (LCX) ostium, the stent was deployed precisely at the LAD ostium, and the left main trunk (LMT) was dilated using a 4.0-mm cutting balloon.

 Video3 (image 6-1).mp4
Video3 (image 6-1).mp4
Video4 (image 6-2).mp4
Video7 (image 7).mp4
Case Summary
Aorto-ostial CTO of the LMT is extremely rare, accounting for approximately 0.1% of all CTOs. In this case, the lesion was particularly unique due to its unprotected LMT, absence of retrogradeoption, and completely separated distal bifurcation. In a bifurcation with separated branches, successful wire passage into one branch inevitably resultsin “short-cut” the entry of the other branch. In this case, cutting angioplasty could not modify the cap; therefore, directional coronary atherectomy (DCA) was employed. Although DCA is currently approved only in Japan, the essential concept is targeted plaque modification at the entry, which may also be achieved with other atherectomy modalities.