Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251101_004
Successful Retrieval of a Fractured Guide Extension Catheter Entrapped in the Left Coronary Artery: A Rare Case Report
By Kuo-Ming Yang
Presenter
Kuo-Ming Yang
Authors
Kuo-Ming Yang1
Affiliation
Department of Cardiology, Kaohsiung Veteran General Hospital , Taiwan1
View Study Report
CASE20251101_004
Coronary - Complication Management
Successful Retrieval of a Fractured Guide Extension Catheter Entrapped in the Left Coronary Artery: A Rare Case Report
Kuo-Ming Yang1
Department of Cardiology, Kaohsiung Veteran General Hospital , Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
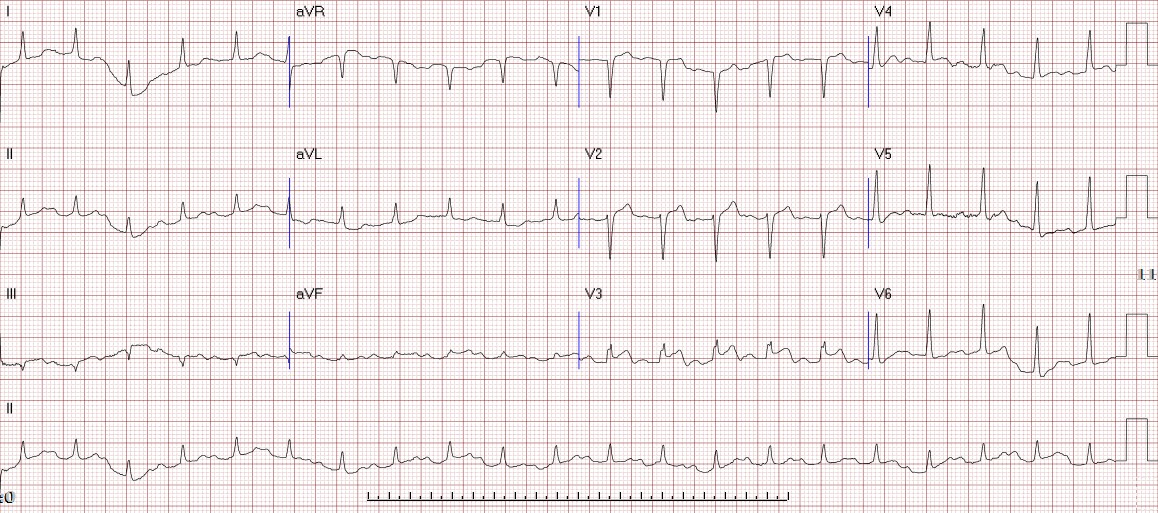
This 74-year-old male smoker with coronary artery disease presented with intermittent fever, abdominal pain and vomiting for a whole. Pulmonary infection related 2nd myocardial infarction was considered as first impression due to pulmonary edema related respiratory failure by CXR and ST elevation atlead V2-3 on ECG. However, ischemic heart disease could not be exculded due to reduced left ventricular ejectional fraction detected. No specific findings were noted on physical examination.

Relevant Test Results Prior to Catheterization
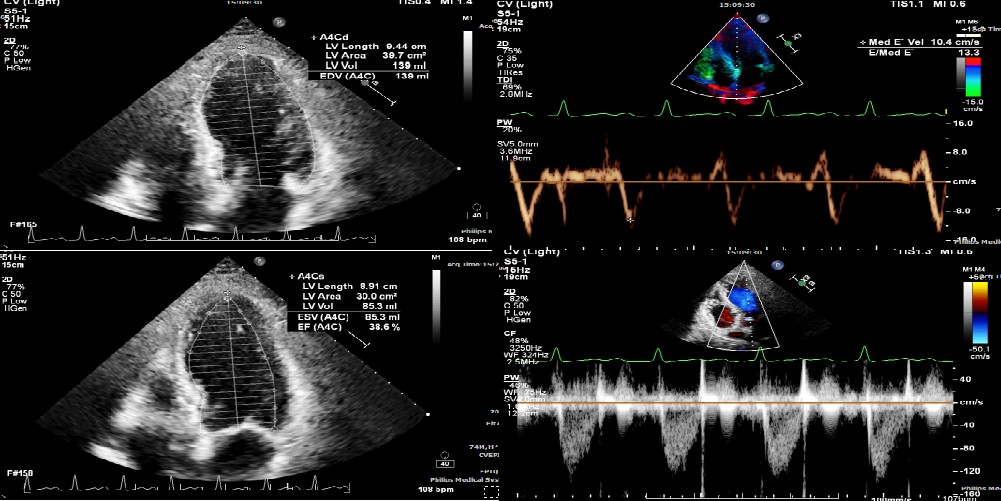
Theseries tests were provided on him prior to catheterization including laboratorytest, chest X-ray, and echocardiography. Mild elevation of cardiac enzymes andmild pulmonary edema were presented. The echocardiography showed 35% of leftventricular ejection fraction with hypokinesia of left ventricular basalinferior wall, apex, and mid-to-apical anterior wall. The rest of tests were unremarkable.
Relevant Catheterization Findings
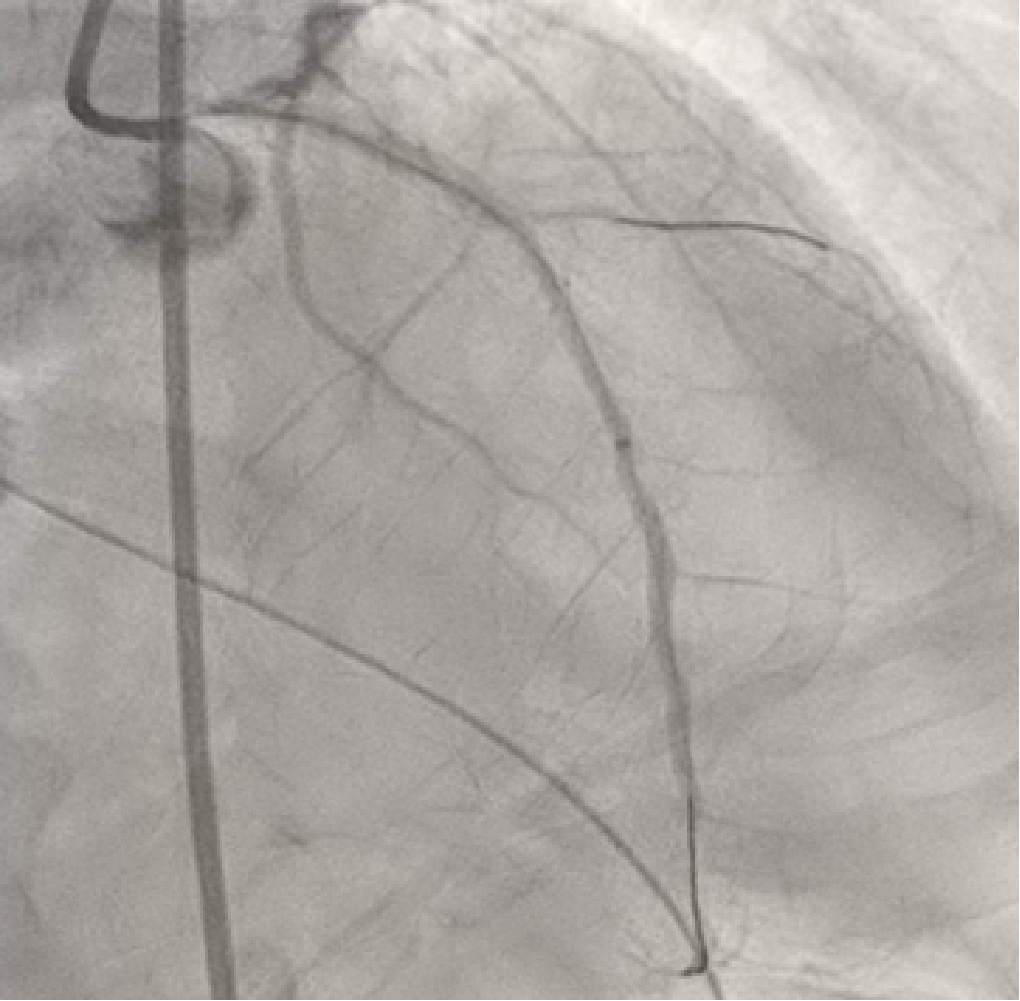
During the PCI, severe diffused lesion with maximum 95% stenosis around proximal part to distal part of LAD and 60% stenosis in the middle part of RCA were diagnosed.
Interventional Management
Procedural Step
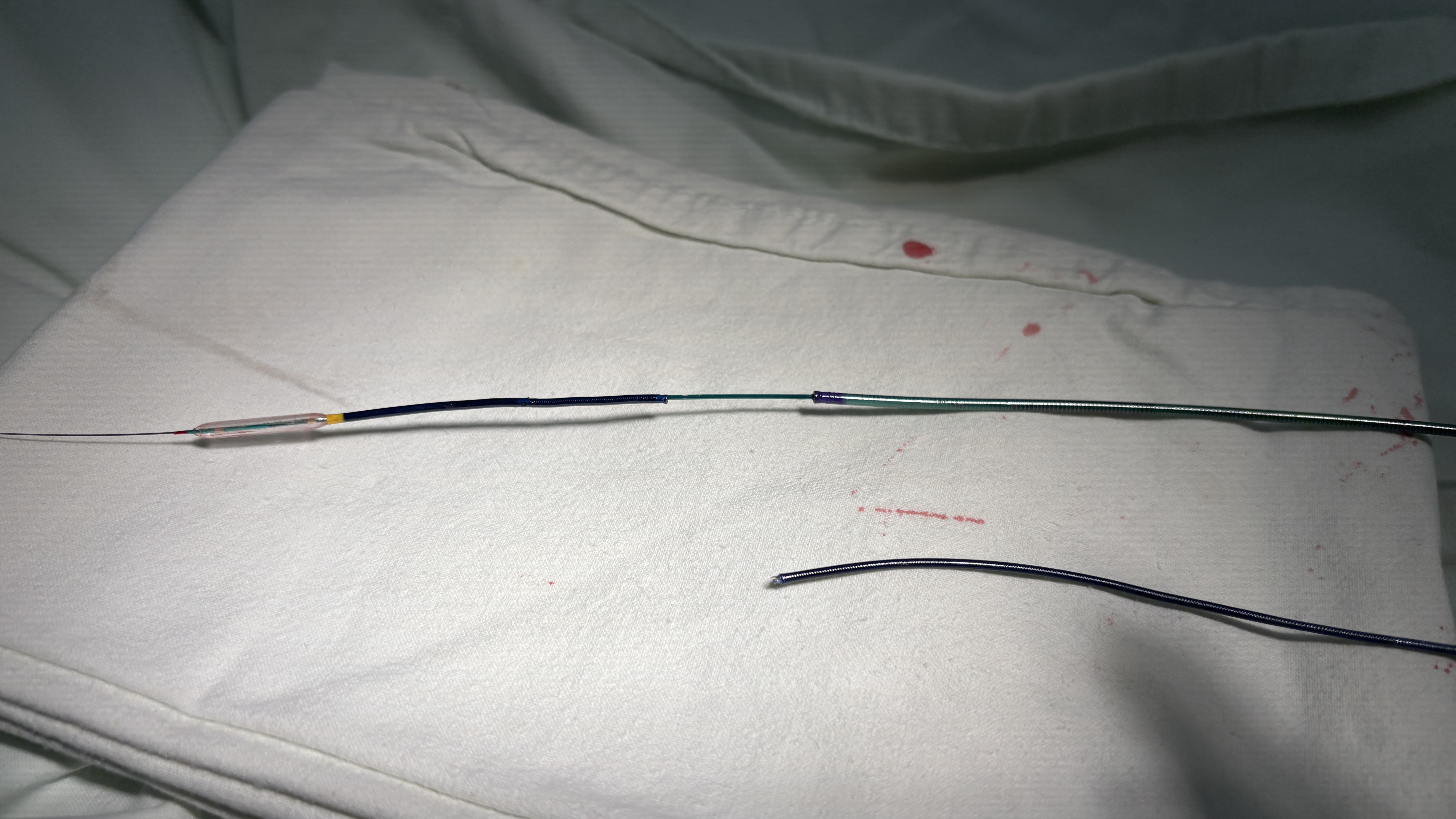
A 3.5x7F ASAHI PB Guide catheter with Sion guidewire was provided for LAD revisualization.After placing the guidewire in LAD, series balloon were provided todilate the stenotic lesions as Figure 1 showed. A 2.5x38 mm stentwas applied to place the distal part lesion of LAD. However, the difficulty to movethe stent to the correct place due to length of the stent and the irregularlumen of proximal part of LAD. 6.0F extension microcatheter was used to assistthe stent moving and implanting. After stenting, the extension microcatheterwas entrapped around middle part of LAD as Figure 2 showed. After pullingbackwards forcedly, the fracture of proximal part of the microcatheter was detectedand previous guidewire was pull out from coronary artery. After rewiring into the distalpart of LAD via the lumen of the fractured microcatheter, 7.0F telescopemicrocatheter with a 2.5x15 mm balloon was applied. The balloon wasmoved in the position 2-3 mm inferior to the fractured microcatheter and proximalpart of telescopemicrocatheter was placed in the ostium of left main coronary artery. After theballoon inflated, the whole sets including the body of the balloon and thetelescope microcatheter were pull backwards. The fractured catheter was movedbackwards with the inflated balloon to enter the telescope microcatheter. Thewhole sets with the fractured catheter were retried from the patientsuccessfully. The retried balloon and fractured catheter were illustrated inFigure 3.

Case Summary
Guideextension catheters were frequently applied in PCI to help the devicedeliverability. However, there were some complications of extension cathetersreported including entrapment of a guide extension catheter. The reportsregarding fractured extension catheter entrapped in coronary artery arelimited. In terms of the issue, successful retrieval of a fractured guide extension catheter entrappedin the left coronary artery was report. There were no significant complicationsoccurring after removing the catheter.