Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251101_003
Retrieval of Thrombosed Inferior Vena Cava Filter and Mechanical Thrombectomy of Associated Caval Thrombosis Using Flowtriever and Clottriever Systems With the Clottriever as Embolic Protection
By Dexter Yak Seng Chan
Presenter
Dexter Yak Seng Chan
Authors
Dexter Yak Seng Chan1
Affiliation
Queen Mary Hospital, Hong Kong, China1
View Study Report
CASE20251101_003
Endovascular - Venous Disease Intervention
Retrieval of Thrombosed Inferior Vena Cava Filter and Mechanical Thrombectomy of Associated Caval Thrombosis Using Flowtriever and Clottriever Systems With the Clottriever as Embolic Protection
Dexter Yak Seng Chan1
Queen Mary Hospital, Hong Kong, China1
Clinical Information
Relevant Clinical History and Physical Exam
A 55-year-old Chinese male with an underlying anti-phospholipid syndrome and prior left leg DVT on warfarin had an IVC filter implanted prior to a radical resection of the perineal sarcoma. Two weeks after the surgery, an IVC filter removal was attempted but thrombus was found at the filter. It was decided to leave the filter and continue with anticoagulation. However, 2 weeks further on, he presented with a progressive right lower limb swelling, erythema and pain which worsened despite warfarin


Relevant Test Results Prior to Catheterization
Ultrasoundand a CT venogram showed an extensive thrombosis from the IVC filter to belowknee veins. He had an INR of 2.2. CT pulmonary angiogram showed no pulmonary embolism
 CT Venogram for case.mp4
CT Venogram for case.mp4
Relevant Catheterization Findings
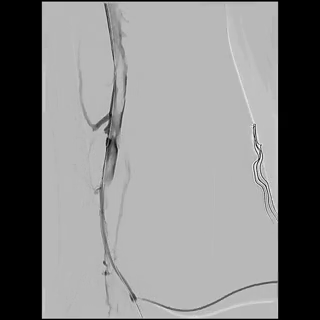
Right internal jugular vein (IJV) and popliteal vein large bore access was obtained with a 14Fr sheath and a 16Fr ClotTriever sheath respectively. Initial venogram showed extensive thrombosis from the below knee popliteal vein to the IVC filter with flow stasis of the intravenous contrast.


aat3xu.mp4
aat45d.mp4
aat3zn.mp4
Interventional Management
Procedural Step
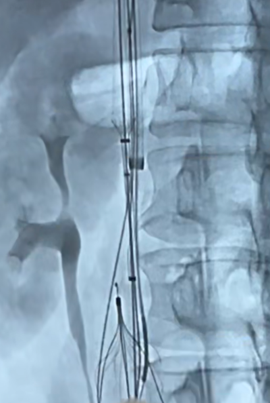
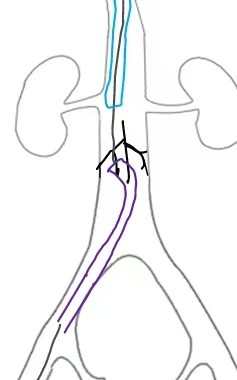
Through and through wire was achieved from popliteal to IJV and the 14fr IJV sheath was advanced past the IVCF struts to act as a protection for the basket and coring element of the ClotTriever for thrombectomy of the IVC and iliofemoral veins as several passes were made. There was satisfactory clearance of clots from the left iliofemoral veins. Aspiration of the IVCF was then performed with a FlowTriever 16 catheter but there was incomplete thrombectomy with some of the remnant clots being pushed above the IVC filter. The IJV sheath was upsized to 16F over and the sheath was used to protect the ClotTriever as it passed though the filter. The through and through Rosen wire (Cook Medical, Bloomington, Indiana) was subsequently pulled back from the IJV and cannulated into the right subclavian vein. The ClotTriever was then deployed next to the 16Fr sheath above the filter as an embolic protection device. The thrombosed IVC filter was then retrieved with a Clover snare (Cook Medical, Bloomington, Indiana). From the IJV sheath, FlowTriever disks were deployed and further thrombectomy of the remnant IVC thrombus was performed which yielded even more thrombus.

use of Flowtriever to aspirate clots from IVC fitler and showing clot above filter.mp4
Flowtriever disk deployment.mp4
post initial thrombectomy showing sheath from IJV past IVC filter as protection for ClotTriever.mp4
Case Summary
Completion venogram showed brisk return of flow and patency.
The patient had a resolution of swelling and pain by the next day and was subsequently discharged on warfarin once he achieved an increased therapeutic target. Post procedural day 1 DVT scans showed patent iliofemoral veins and IVC. 2 months post procedure ultrasound showed continued patency of the iliofemoral veins and IVC and he remained asymptomatic.