Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251101_002
The DK-Crush Antegrade Approach With Angulated Microcatheter for Complex Bifurcation Lesions: Subocclusive Left Main Stenosis and Ostial Circumflex Occlusion
By Farhat Fouladvand
Presenter
Farhat Fouladvand
Authors
Farhat Fouladvand1
Affiliation
Clinica San Carlo, Italy1
View Study Report
CASE20251101_002
Coronary - Complex PCI - CTO
The DK-Crush Antegrade Approach With Angulated Microcatheter for Complex Bifurcation Lesions: Subocclusive Left Main Stenosis and Ostial Circumflex Occlusion
Farhat Fouladvand1
Clinica San Carlo, Italy1
Clinical Information
Relevant Clinical History and Physical Exam
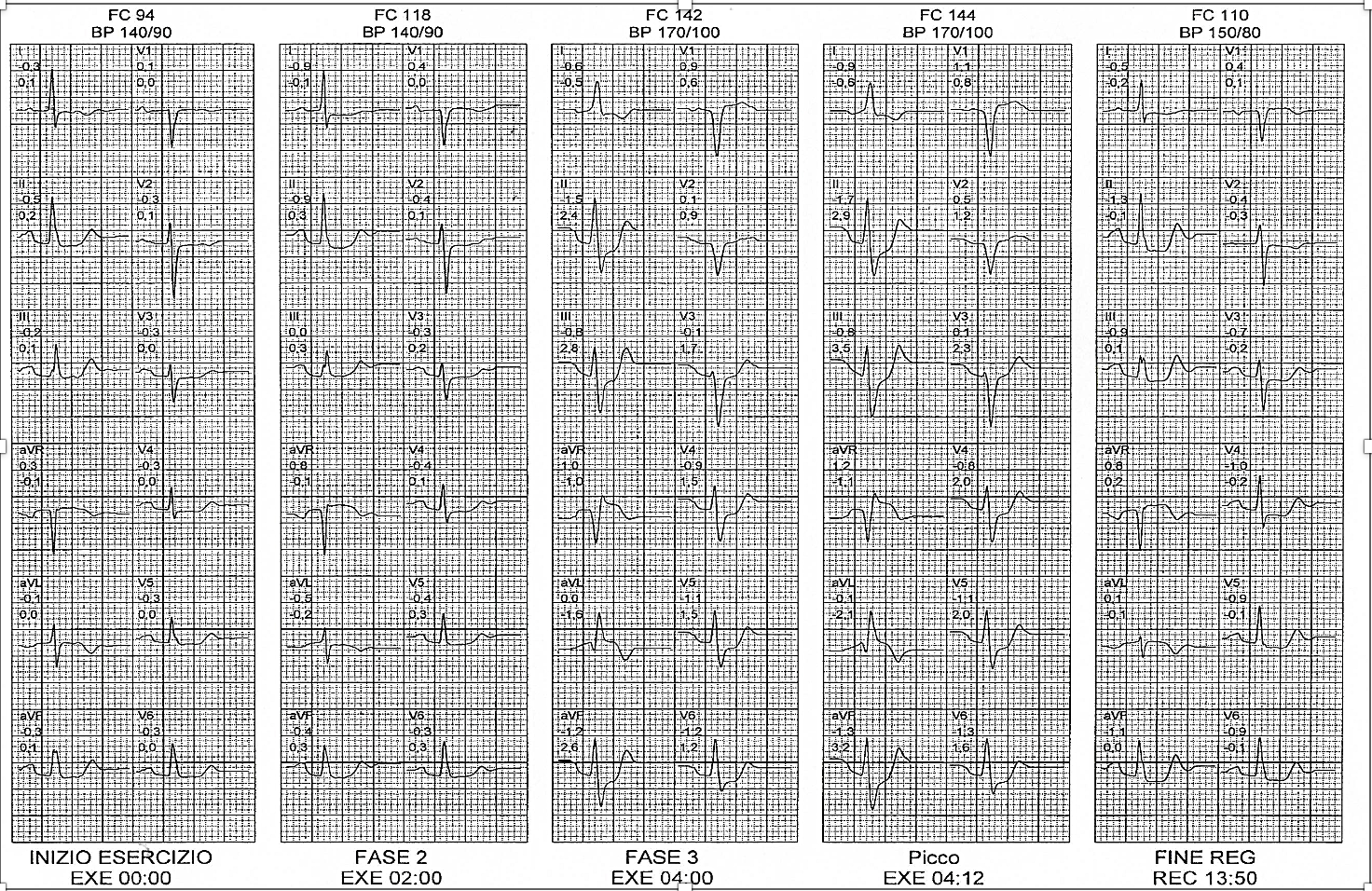
A 65-year-old woman with diabetes, hypertension, and dyslipidemia presented with effort angina. A treadmill test was positive for ischemia, showing significant ST depression and aVR elevation. She experienced chest pain that subsided during recovery, prompting same-day admission and coronary angiography.
Relevant Test Results Prior to Catheterization
The echocardiogram was normal. Laboratory results prior to catheterization showed elevated blood glucose (180 mg/dL), glycated hemoglobin (8.3%), and a poor lipid profile (LDL 175 mg/dL). Her renal function was severely impaired, with a creatinine of 2.5 mg/dL and an eGFR of 19.5 ml/min/1.73m².
Relevant Catheterization Findings
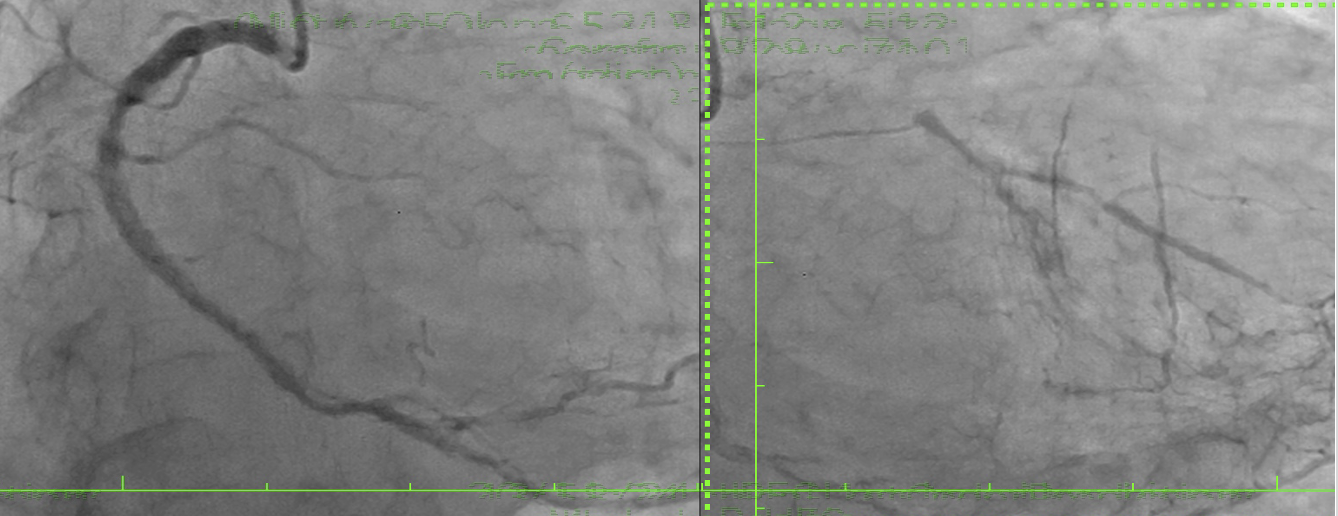
Same-day coronary angiography revealed diffuse disease in the right coronary artery providing collaterals to the LCx and LAD. A subocclusive distal left main stenosis extended into the LAD. Despite a high Syntax score (33) favoring bypass, the patient opted for percutaneous treatment. A key challenge was locating the LCx ostium, which was angiographically silent, with only a thin channel guiding the wire toward the LAD, complicating LCx access.
Interventional Management
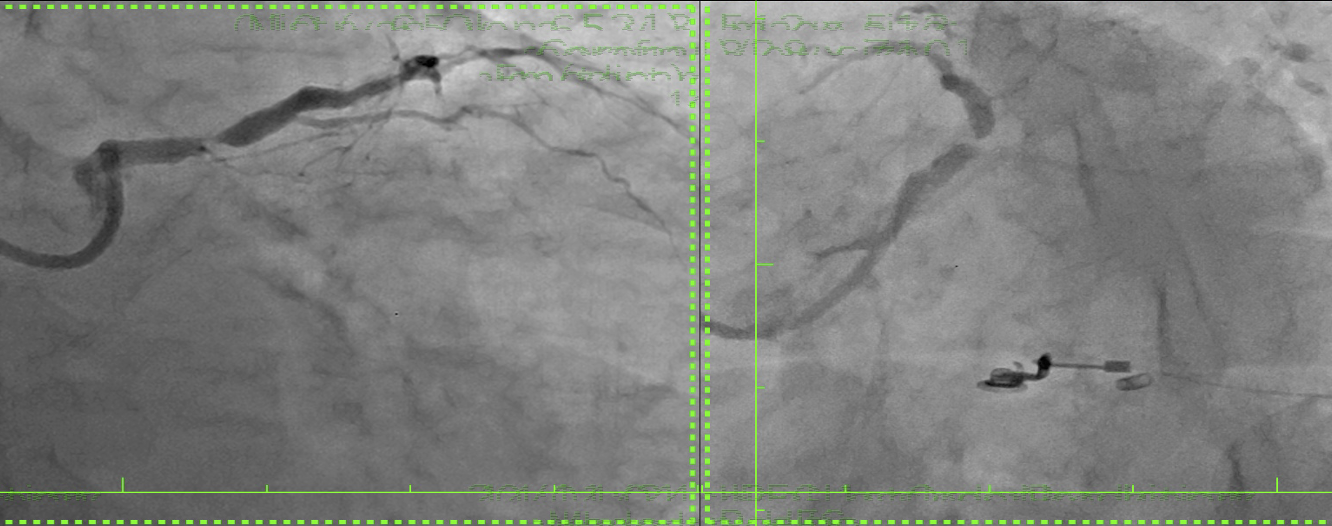
Procedural Step
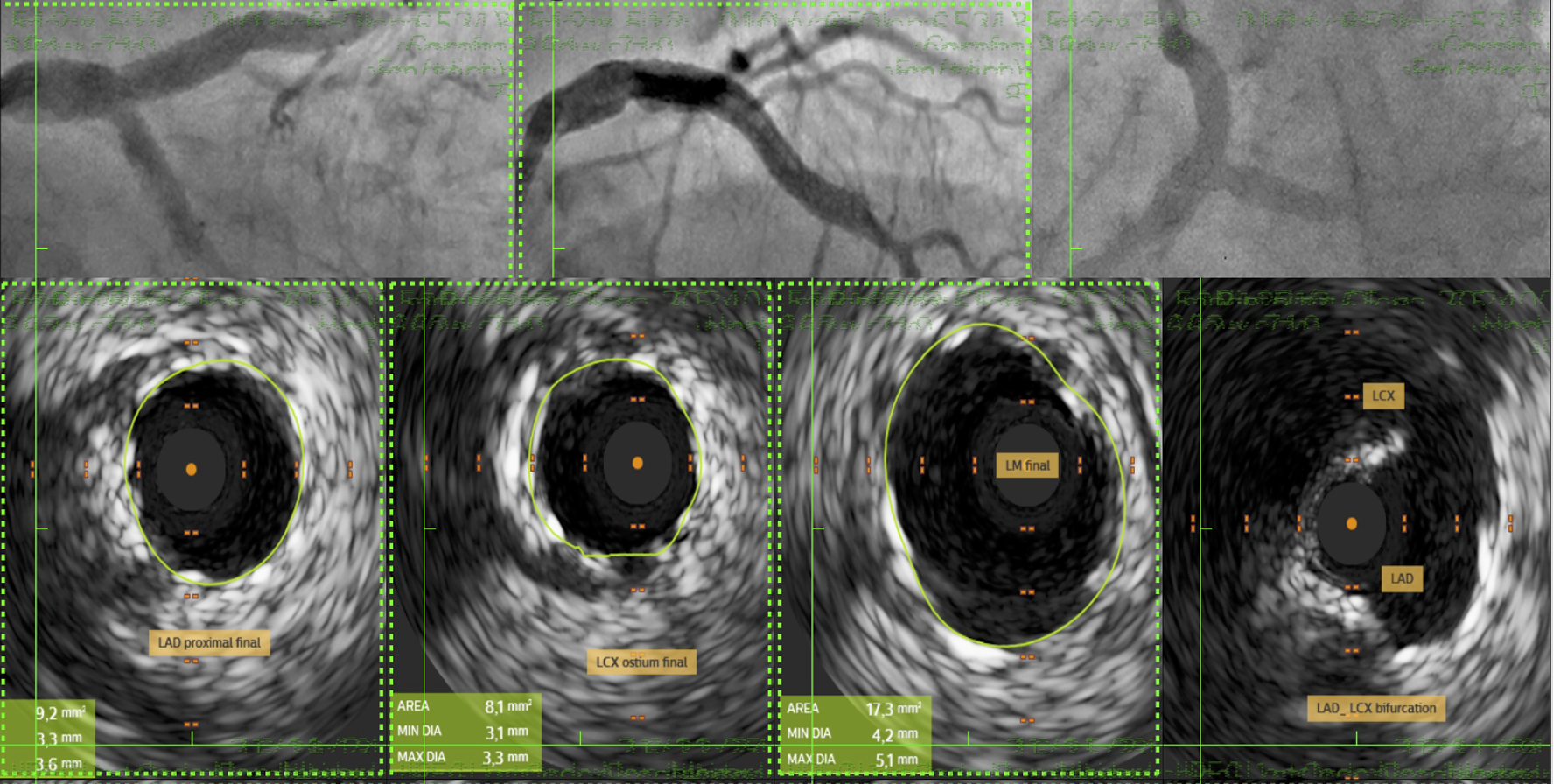
The procedure commenced with IABP insertion and the use of a 7F XB guiding catheter for an antegrade approach. A wire was advanced across the LM-LAD stenosis, and predilatation with a 2.5 mm semicompliant (SC) balloon revealed the faint ostium of the occluded LCx. A 45° angulated microcatheter facilitated the crossing of the LCx occlusion with a stiff wire, which was then exchanged for a standard workhorse wire.Following LCx predilatation, kissing balloon pre-dilation of the LM-LAD-LCx bifurcation was performed. A 3.0x18 mm Sirolimus stent was deployed in the proximal LAD. Subsequently, a 2.75x18 mm Sirolimus stent was placed in the LCx with minimal protrusion into the LM and crushed with a 3.5 mm non-compliant (NC) balloon. The crushed stent struts were recrossed, predilated with sequential SC balloons, and a distal optimization (DOT) was performed. A second kissing balloon inflation followed.A third Sirolimus stent (4.0x25 mm) was then overlapped with the previous stent in the LAD-LM segment. After a proximal optimization technique (POT) in the LM, the LCx was rewired. Final optimization included further DOT in both the LAD and LCx, a final triple kissing balloon inflation, and a concluding POT. An excellent final result was confirmed by IVUS (LAD area 9.2 mm²; LCx area 8.1 mm²; minimal lumen area 16 mm²) and angiography, after which the IABP was removed.
Case Summary
A 65-year-old woman with complex coronary disease, including distal left main stenosis and a chronic occluded LCx ostium, successfully underwent percutaneous intervention using a DK-crush stenting technique after refusing surgery. The challenging LCx origin, identified after LM-LAD predilatation, was crossed using a 45° angulated microcatheter. The patient remained asymptomatic with excellent therapy compliance at follow-up. The procedure's success was confirmed by IVUS, demonstrating the efficacy of tailored percutaneous approaches for complex lesions.