Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251031_001
A Challenging Case of RCA Ostial CTO With Severe Calcification
By Taito Nagai
Presenter
Taito Nagai
Authors
Taito Nagai1
Affiliation
Misato Central General Hospital, Japan1
View Study Report
CASE20251031_001
Coronary - Complex PCI - CTO
A Challenging Case of RCA Ostial CTO With Severe Calcification
Taito Nagai1
Misato Central General Hospital, Japan1
Clinical Information
Relevant Clinical History and Physical Exam
Case is 80s female who had medical history of hypertention and dyslipidemia. The patient veisited our hosipital with the chief complaint of worsening exertional chest pain, and was diagnosed with effort angina pectoris. There were no obvious signs of heart failure such as lower limb edema, decreased oxygenation.
Relevant Test Results Prior to Catheterization
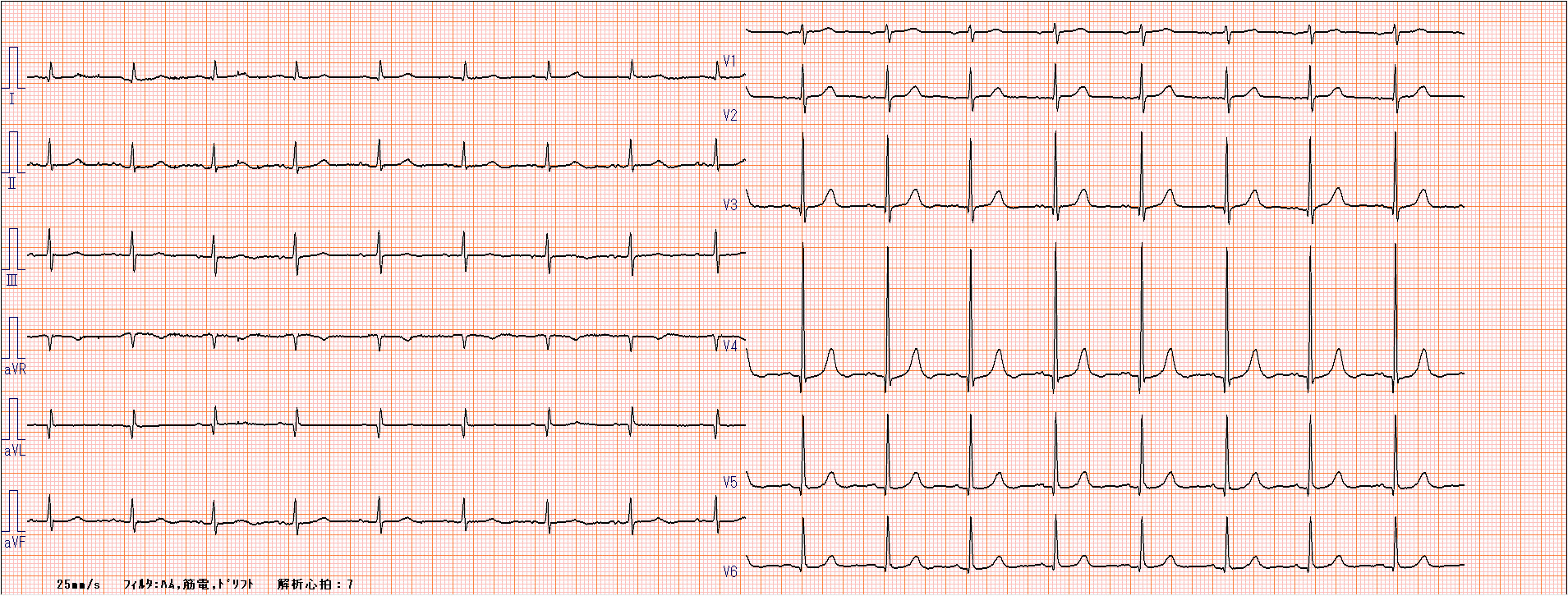
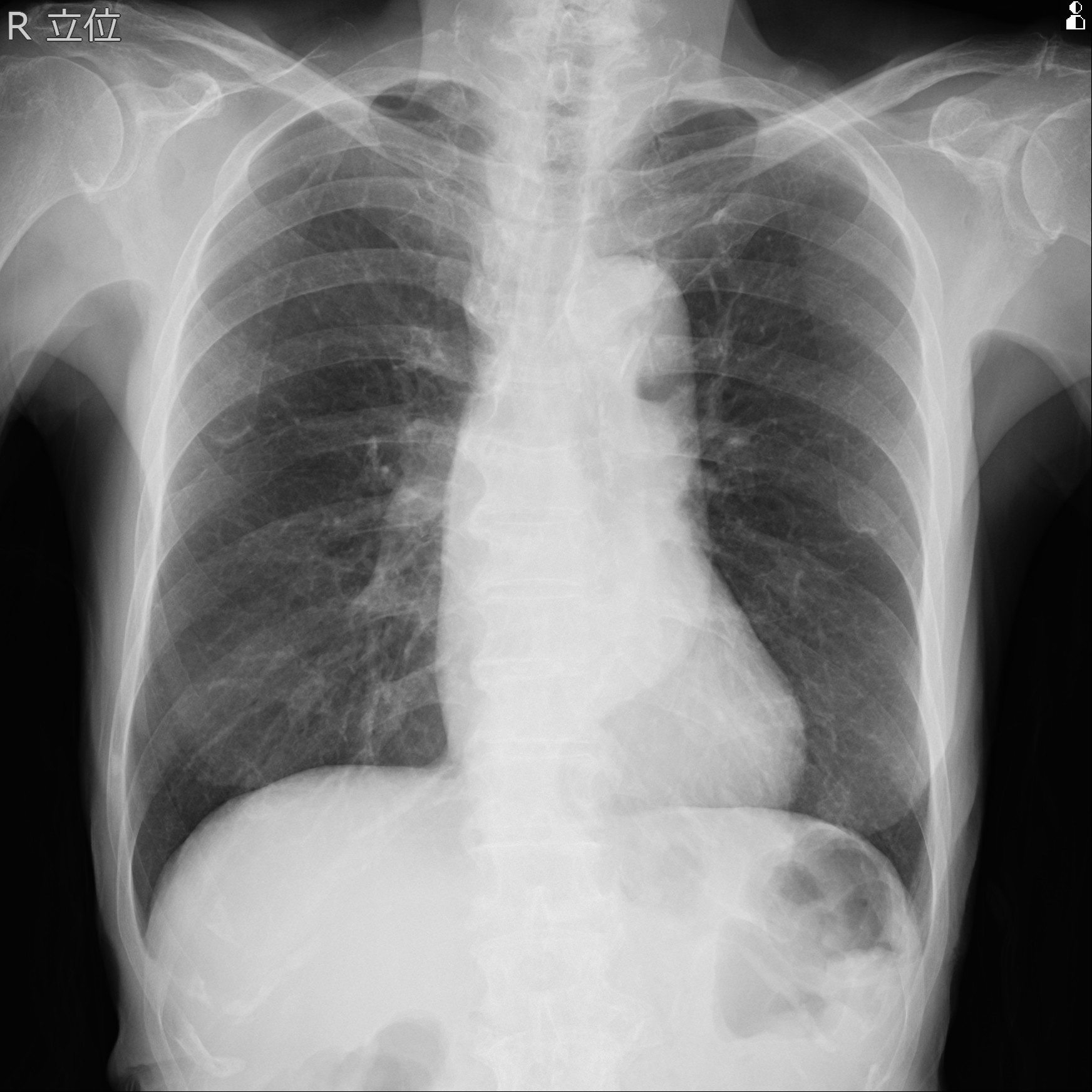
Blood test showed as follows. Renal function was normal (eGFR=63.7), LDL-C was 47mg/dl, HbA1c was 5.3%. ECG showed sinus rhythm and no ST-T change. Chest X-ray showed no pulmonary congestion, and CTR was 49%. Echocardiogram showed no asynergy and normal LV function (EF62%) with mild-moderte AR.
Relevant Catheterization Findings
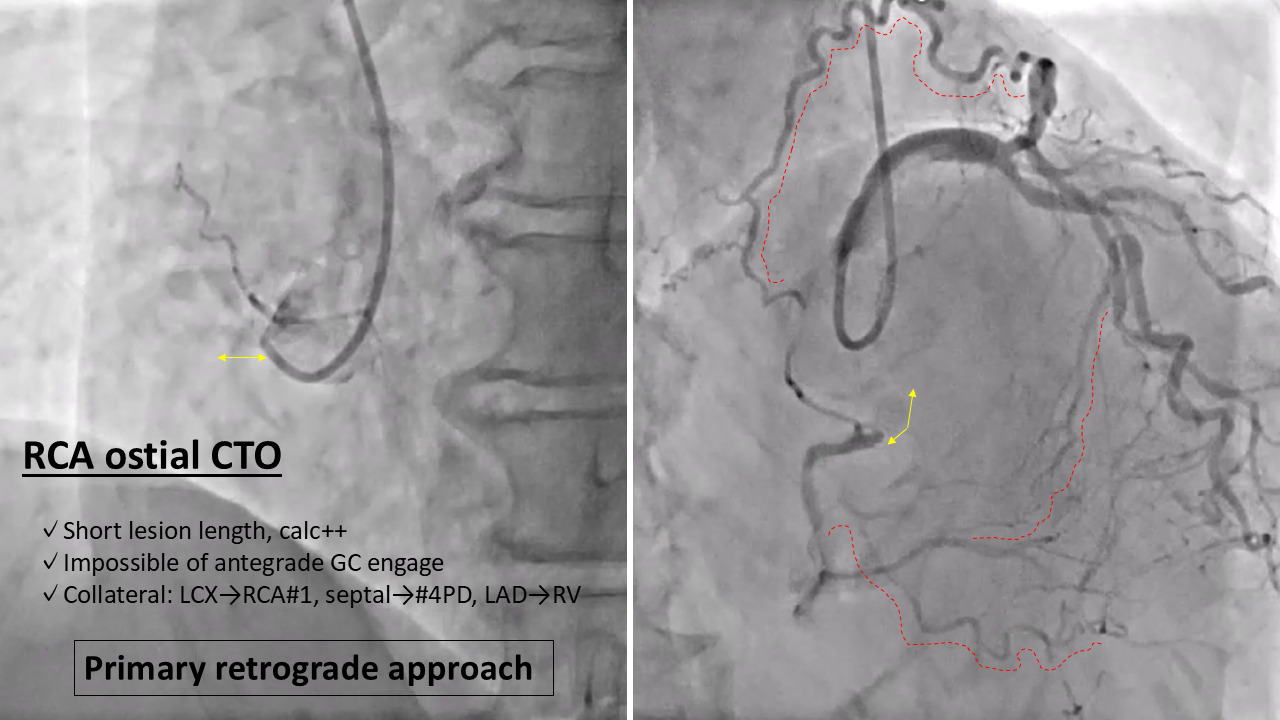
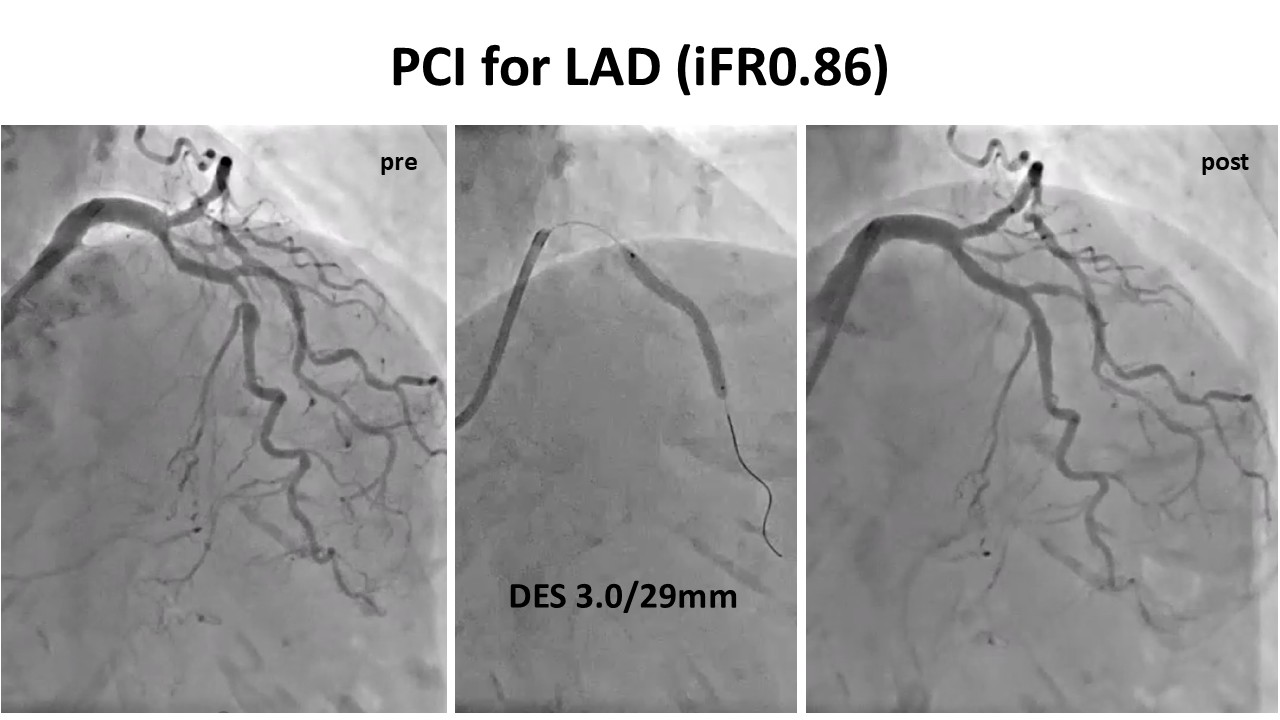
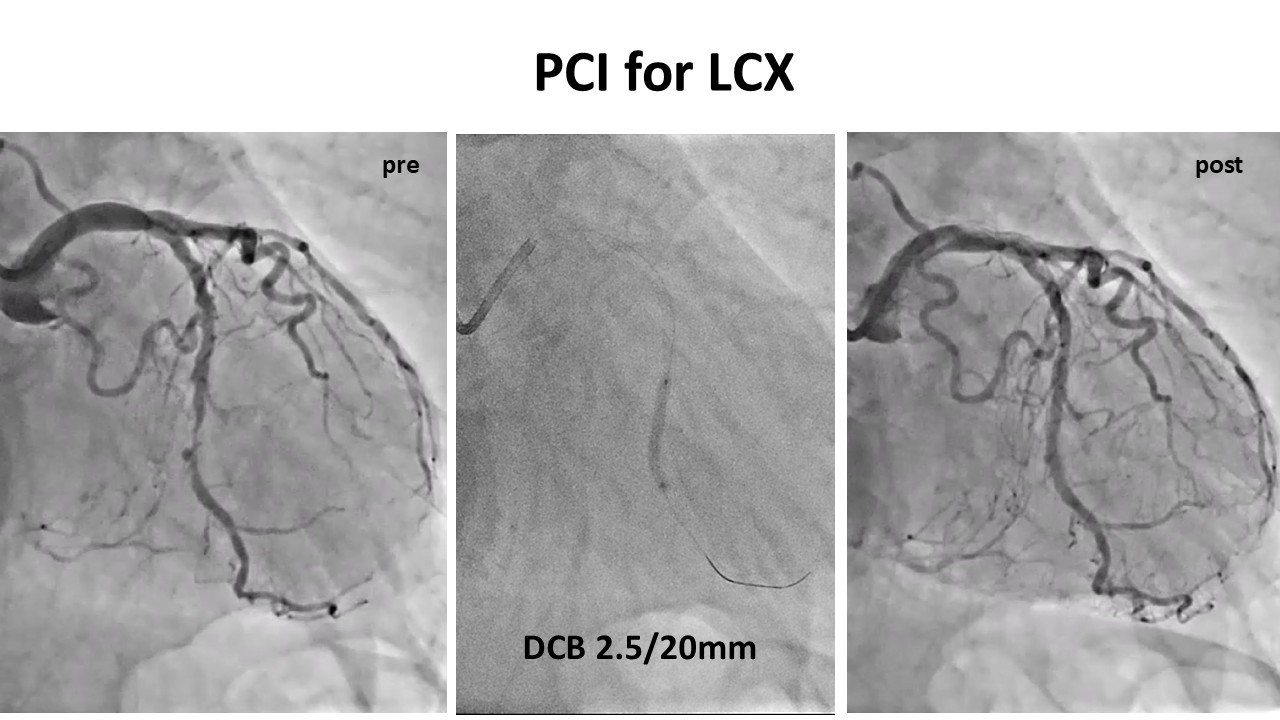
CAG showed three vessel disease. There were moderate-to severe stenosis at the mid of LAD and LCX and RCA#1 was occluded from ostial with severe calcification. Diagnostic catheter could not engage for RCA. After LAD and LCX lesion was treated, we planned to performe PCI for RCA CTO lesion.
Interventional Management
Procedural Step
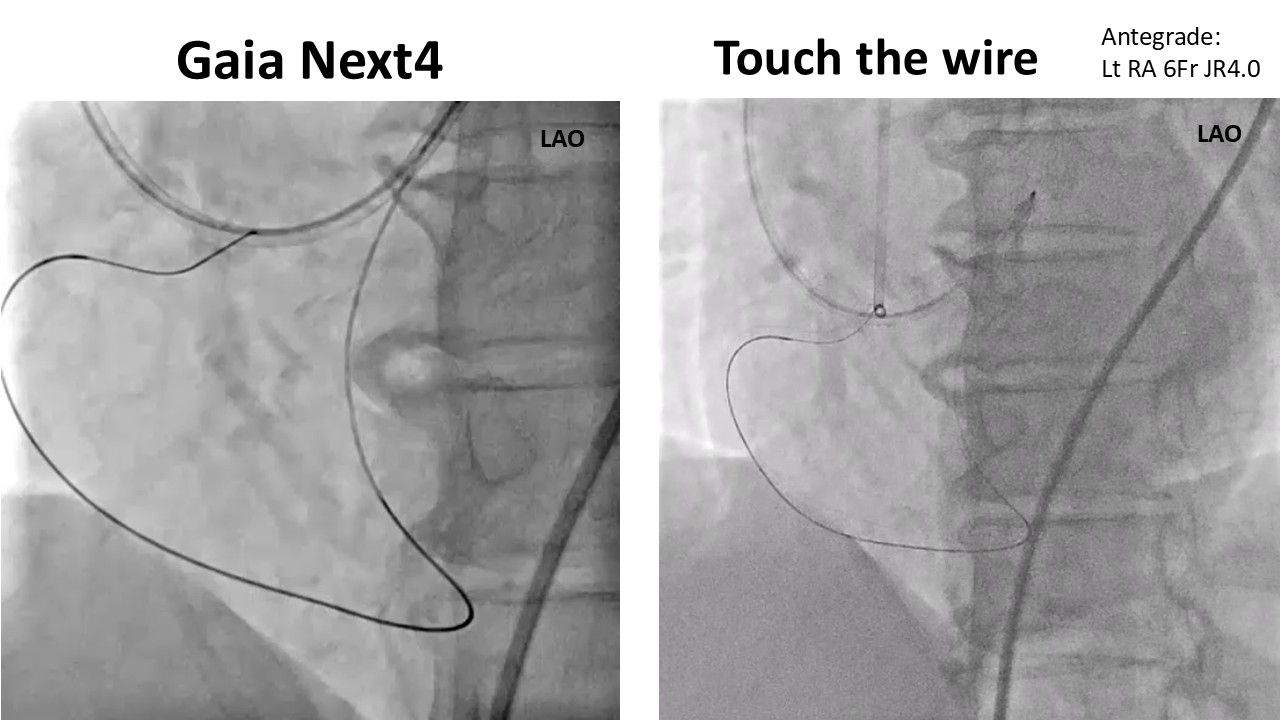
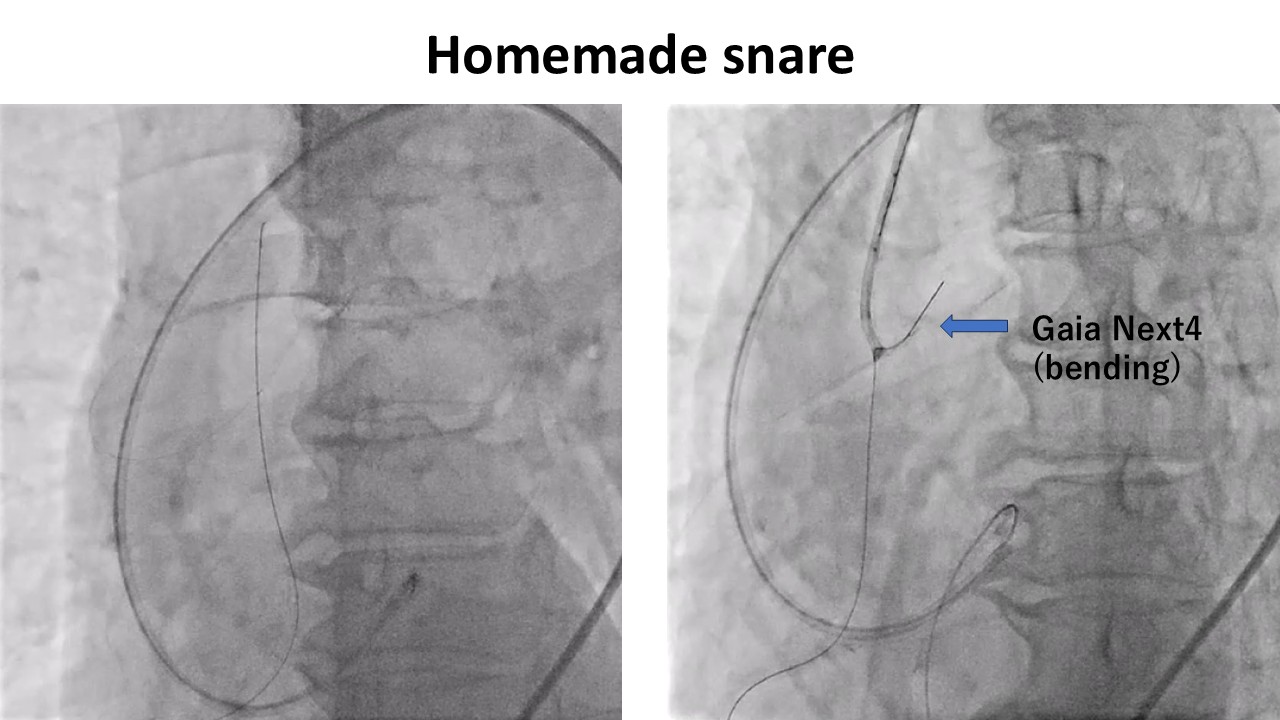
Primary retrograde approach was performed through the septal branch, and SUOH03 wire and Corsair XS reach the near position of CTO exit. Gaia Next4 succeeded to pass through the CTO lesion by retrogradely and we confirmed the wire passage by touching with antegradeguiding catheter, but Corsair XS could not pass the CTO lesion due to severe calcification. We made homemade snare with guide-extension catheter, small diameter balloon, conventional wire, and catch the Gaia Next4 within aorta. After that, MC:Zizai could pass the CTO lesion by retrogradely. But we could not change the wire within antegrade guiding catheter because the Gaia Next 4 was bended made by cathching with homemade snare, then externalization could not be established. After releasing the Gaia Next4 once out of antegrade guiding catheter, we suceeded to pull out the bended Gaia Next4 and change to RG3. After pull through system was established by re-catch the wire with homemade snare, small diameter balloon crossed the lesion and dilated. Because IVUS imaging showed severe calcified plaque, Intracoronary lithotripsy was used for modificaton. We put the drug-eluting stent for the CTO lesion, and finished the procedure. Final angiography showed no flow limitation and acceptable stent expansion.
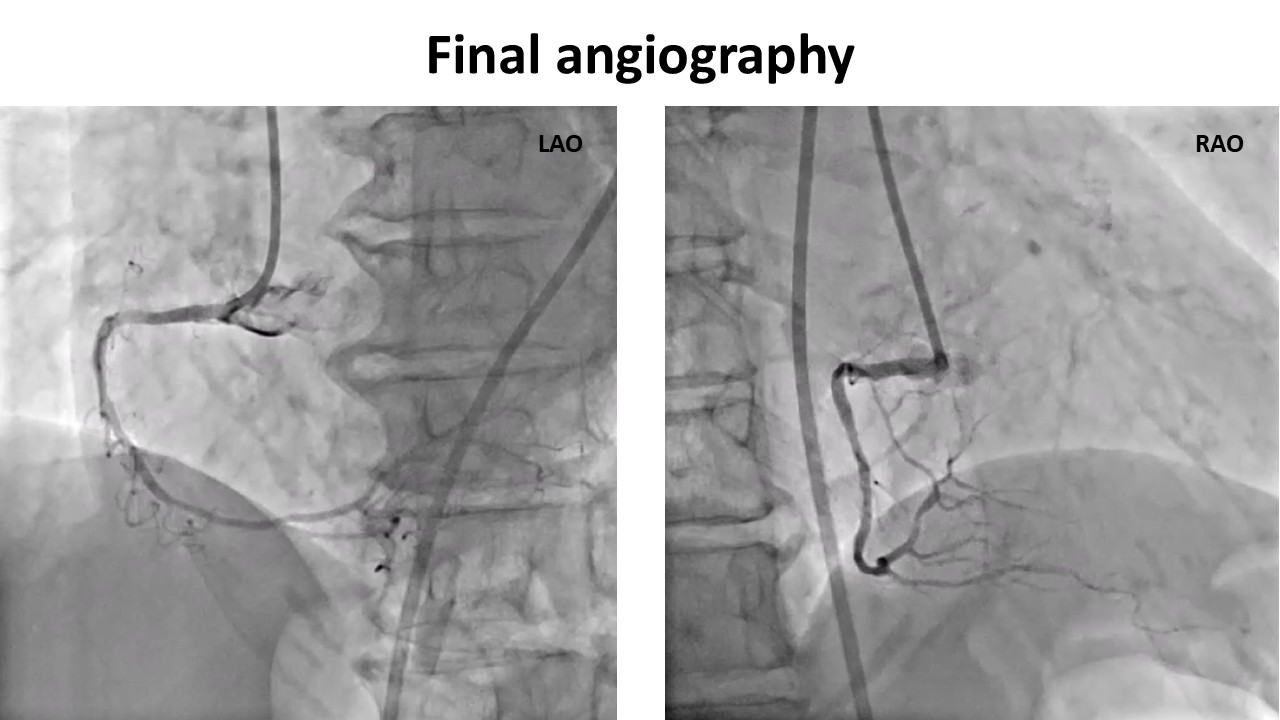
Case Summary
Because retrograde approach was only choice of the strategy for this case, there were some limitations and tips of the procedure. Although we succeeded direct wire crossing by retrogradely, microcatheter could not pass the CTO lesion due to severe calcification. At the situation, homemade snare is good option for establishing pull through system. If the wire position by catching with homemade snare is too proximal site, there is some risk of bending of wire. In this case, we fortunately succeeded to release and change the wire to RG3, and establish the pull through system. We experienced RCA ostial CTO with severe calcification and succeeded to treat by using several techniques.