Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251030_007
Catastrophic Nightmare in Acute Inferior Wall STEMI
By Wongwaris Aphijirawat
Presenter
Wongwaris Aphijirawat
Authors
Wongwaris Aphijirawat1
Affiliation
Queen Sirikit Naval Hospital, Thailand1
View Study Report
CASE20251030_007
Coronary - Complication Management
Catastrophic Nightmare in Acute Inferior Wall STEMI
Wongwaris Aphijirawat1
Queen Sirikit Naval Hospital, Thailand1
Clinical Information
Relevant Clinical History and Physical Exam
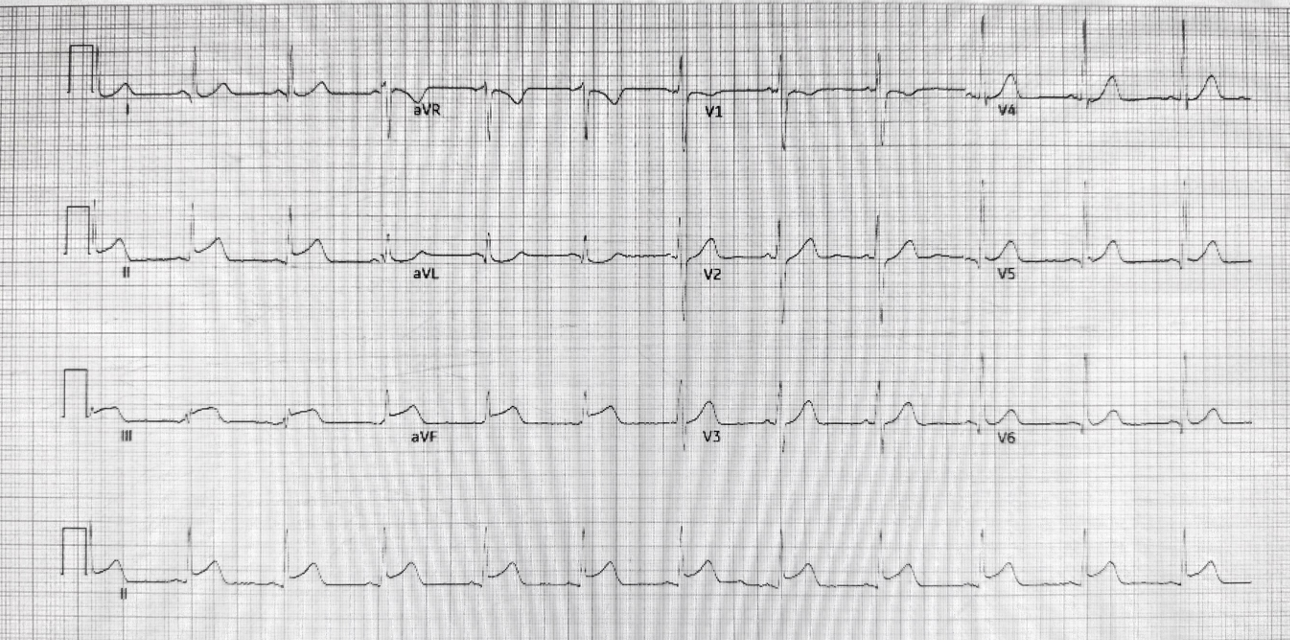
A 33 year old man , non smoker,with a history of of spinal surgery presented with sudden chest pain at rest with diaphoresis for 1 hour PTA. He went to emergency department. ECG Showed sinus rhythm with ST elevation in II, III, avF. Acute inferior wall STEMI was diagnosed, and he was emergency brought into cath lab.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
Left main : No significant stenosisLAD : total occlusion at distal segmentLcx : total occlusion at distal OM branchRCA : No significant stenosis
 Baseline angiogram RAO caudal.mpg
Baseline angiogram RAO caudal.mpg
Baseline angiogram RAO cranial.mpg
Baseline angiogram RCA1.mpg
Interventional Management
Procedural Step
We access right radial artery using 5/6 F sheath, IL 3.5 catheter.Angiogram showed total occlusion at distal segment of OM1 branch and distal LAD. Then we injected RCA which no significant stenosis. We thought the culprit lesion was distal OM branch then we planned to engage Left coronary again. Just a seconds after we prepared to engaged left system again, patient suddenly developed hypotension and then cardiac arrest. Simultaneous CPR and left coronary system injection were performed. At this time, the left system showed the total occlusion of left main coronary artery!! With TIMI 0 flow.

angiogram1.mov
procedure2.mov
final angiogram.mov
Case Summary
We also search for the etiology of MI the young patient with non-smoking. All hypercoagulable state were negative. Echocardiogram showed good LVEF but the agitated saline bubble test was positive with > 30 microbubbles during Valsalva’s maneuver. High risk PFO was diagnosed. An 25/18 mm PFO device closure was done. So, the final diagnosis is coronary emboli causing acute inferior wall STEMI with the guiding-induced left main dissection during coronary angiogram.