Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251029_005
A Case of ECMO-Assisted Rotational Atherectomy for Multi-Vessel Coronary Artery Stenosis With Calcification
By Haoyu Wu
Presenter
Haoyu Wu
Authors
Haoyu Wu1
Affiliation
Shaanxi Provincial People’s Hospital, China1
View Study Report
CASE20251029_005
Coronary - Complex PCI - Calcified Lesion
A Case of ECMO-Assisted Rotational Atherectomy for Multi-Vessel Coronary Artery Stenosis With Calcification
Haoyu Wu1
Shaanxi Provincial People’s Hospital, China1
Clinical Information
Relevant Clinical History and Physical Exam
Sex & Age: Female, 67 years old.Height & Weight: 160 cm, 61 kg.BMI: 23.8 kg/m².Chief Complaint: Recurrent episodes of chest tightness for 4 years.Risk factors: No history of smoking, hypertension, or diabetes.
Relevant Test Results Prior to Catheterization
NT-proBNP: 9119 pg/mL.Myocardial Injury Markers: Within normal range.
Blood Lipids: Triglycerides (TG): 1.07 mmol/L; LDL-C: 2.6 mmol/L.
Serum Creatinine: 59.77 μmol/L.
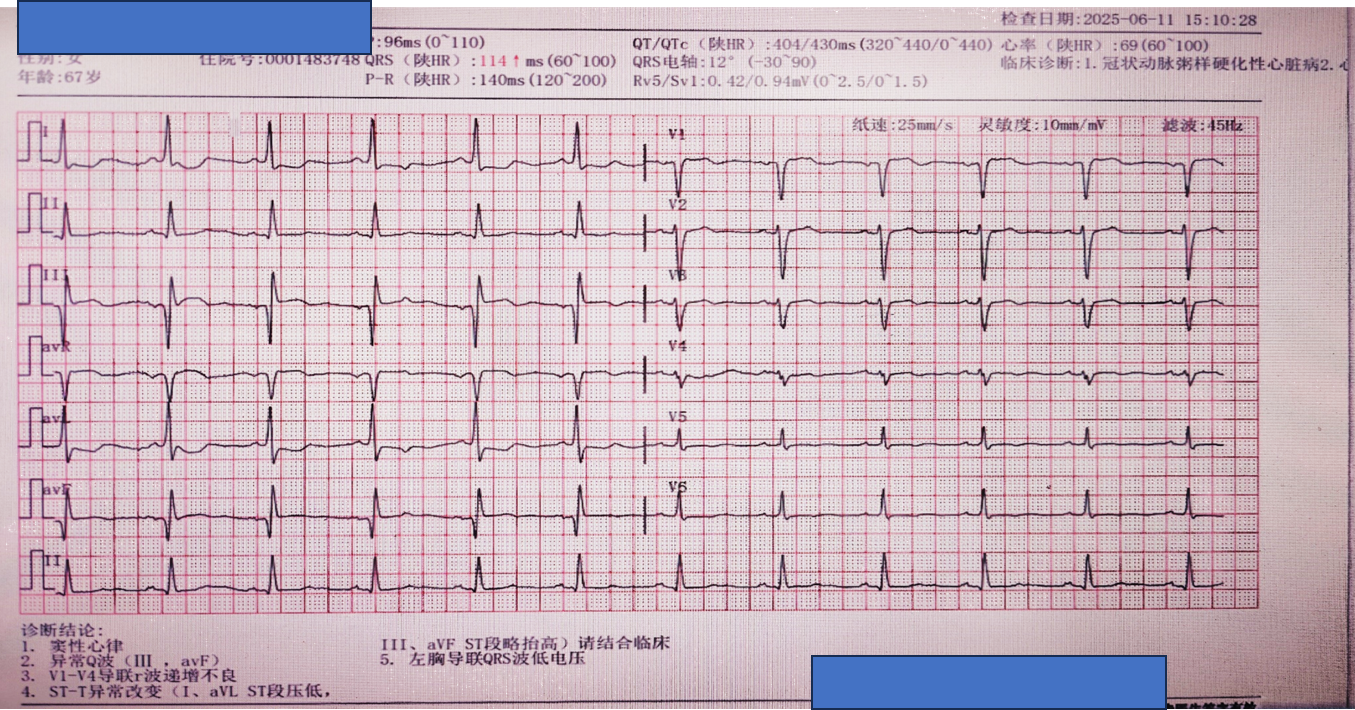
Echocardiography Results: Left Ventricular Ejection Fraction (LVEF): 37%; Regional Wall Motion Abnormalities: Reduced contraction observed in the apical segment of the left ventricular anterior wall, cardiac apex, and basal segment of the inferior wall.
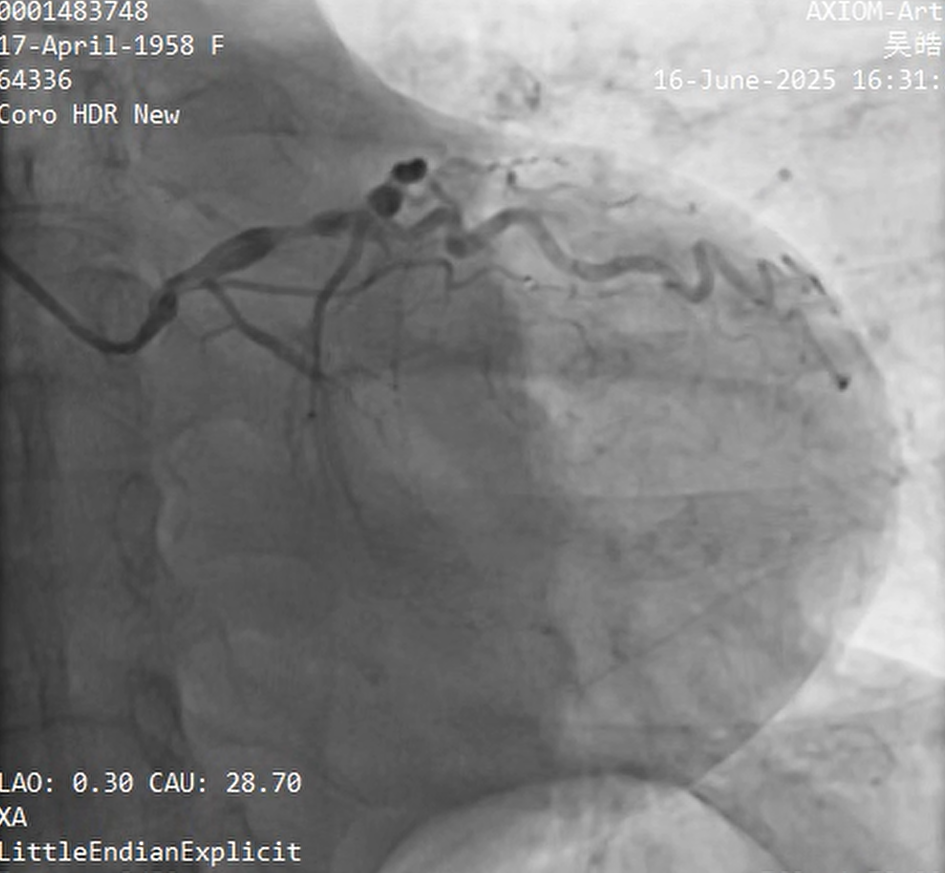
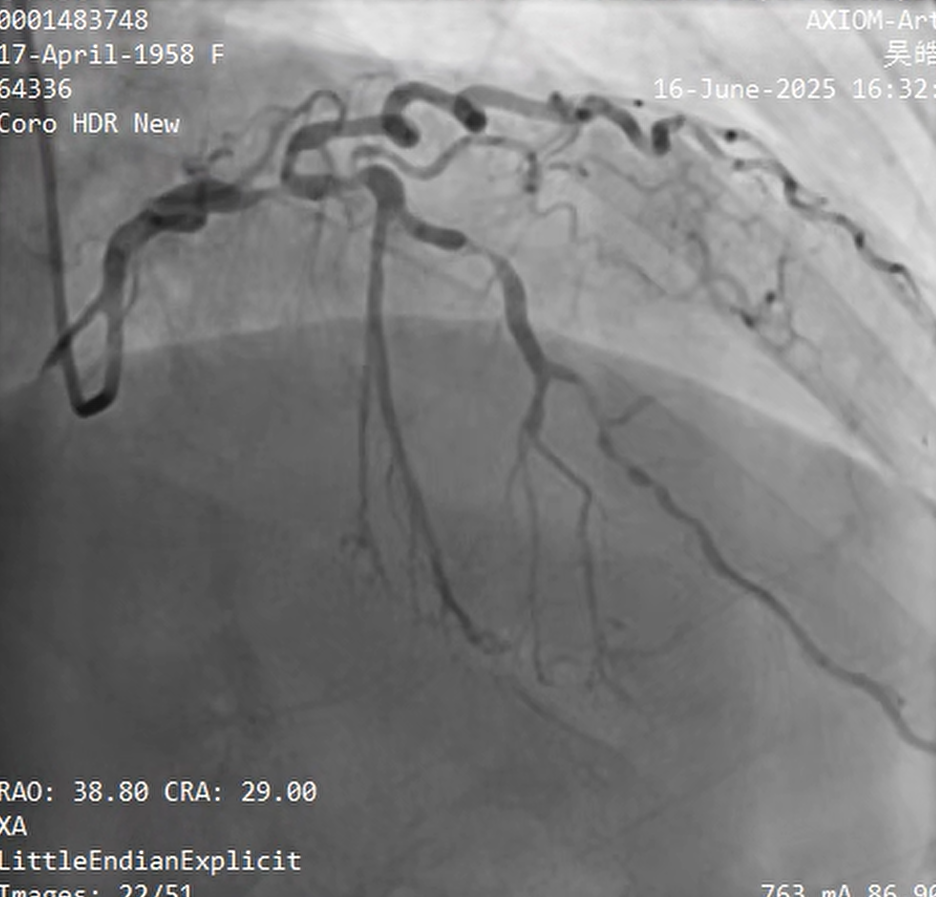
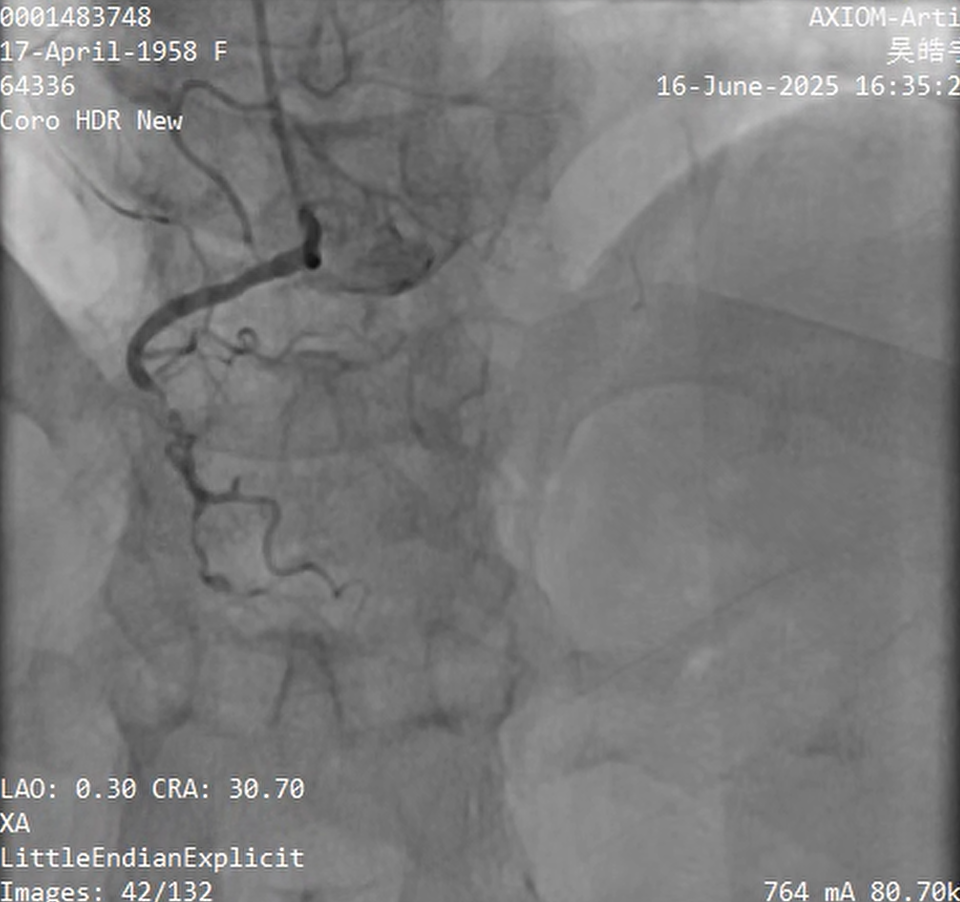
Relevant Catheterization Findings
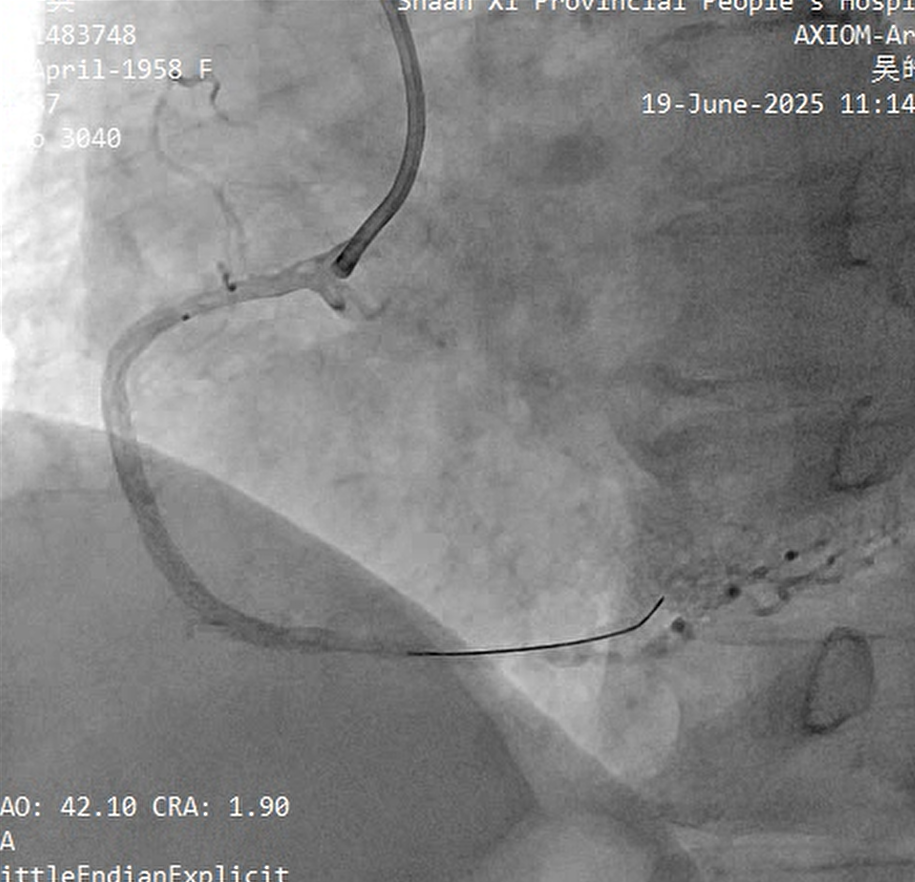
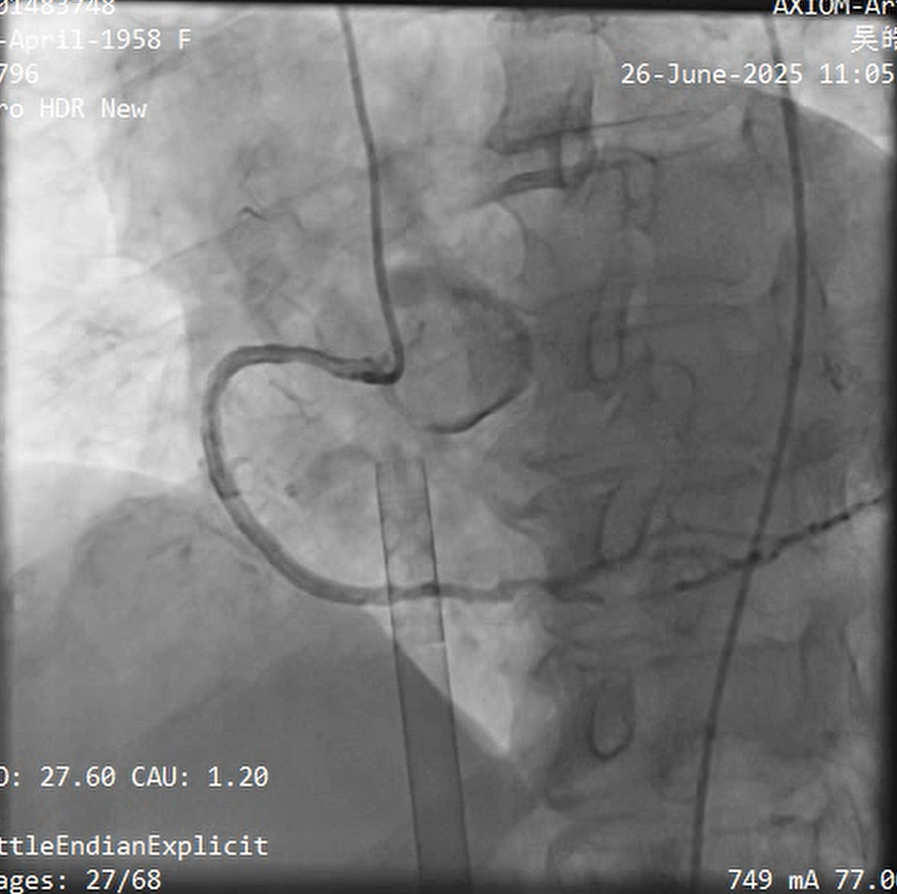
30% stenosis in LMT; 100% stenosis in LCX;99% stenosis with calcification in the LAD;99% stenosis in the RCA。
 CAG1.mp4
CAG1.mp4
CAG2.mp4
CAG3.mp4
Interventional Management
Procedural Step
Strategy:CABG Refused ;RCA to Be Addressed First;Left Coronary Lesions to Be Treated Under ECMO Support.
Balloon failure to cross the LAD.mp4
Rotational atherectomy for LAD.mp4
Final angiogram for LAD.mp4
RCA:
XT-A wire was successfully redirected into the distal true lumen after multiple manipulations;
Advancement of the microcatheter was obstructed by a lesion in the mid RCA;
The microcatheter was withdrawn, and angiography confirmed that the guidewire was in the true lumen;
0.8 × 10 mm balloon failed to cross the proximal lesion in the RCA2;
With the support of a Guidezilla catheter, the 0.8 × 10 mm balloon successfully crossed the lesion;
Under IVUS guidance, a 2.0 × 38 mm DCB was implanted in RCA2-3, 3.0 × 32 mm and 3.0 × 19 mm DES were implanted in RCA1-2;
The left coronary lesion was addressed in 7 days, with ECMO support.
LAD:
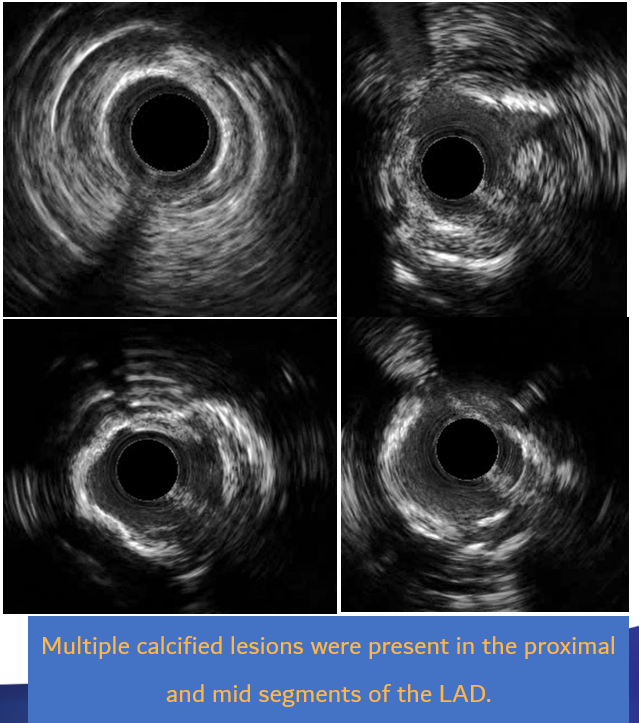
Neither 0.8 × 10 mm nor 1.25 × 15 mm balloon could cross the mid LAD lesion; tactile feedback confirmed calcification;
Rotational atherectomy was initiated. However, the microcatheter could only be advanced to the mid segment of the LAD. The rotawire was then exchanged through the microcatheter;
1.25mm Bur,a distinct "breakthrough" sensation was felt as the rotablation burr crossed the mid LAD lesion;
During rotational atherectomy, transient coronary no-reflow occurred, accompanied by hypotension and bradycardia.;
The 2.0 × 15 mm balloon successfully and smoothly crossed;
LAD 6-8, a 2.0 × 24 mm DCB was deployed, followed by the implantation of a 2.75 × 20 mm stent and a 3.5 × 16 mm stent;
The treatment for the LCX was scheduled for a later stage.
Case Summary
The patient's baseline cardiac function was severely compromised, which significantly increased the procedural complexity and risk from the outset.Initial difficulties were encountered during the right coronary artery intervention, including failure to advance microcatheters and balloons. However, the complexity peaked during the left coronary intervention, where severe calcification necessitated rotational atherectomy as the viable strategy to modify the plaque.During the atherectomy, the patient developed hemodynamic instability. ECMO provided essential hemodynamic support, enabling this high-risk PCI and atherectomy to be completed safely.