Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251029_004
Fight or Flight? - An Undeflated Stent Balloon Snap and Stuck at the Left Main Coronary Artery
By Che Yan Liu, Chun Yuan Chu
Presenter
Che Yan Liu
Authors
Che Yan Liu1, Chun Yuan Chu1
Affiliation
Kaohsiung Medical University, Taiwan1
View Study Report
CASE20251029_004
Coronary - Complication Management
Fight or Flight? - An Undeflated Stent Balloon Snap and Stuck at the Left Main Coronary Artery
Che Yan Liu1, Chun Yuan Chu1
Kaohsiung Medical University, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
A 72-year-old man with a history of type 2 diabetes, hypertension, and End-stage renal disease. He was approached to our emergency department due to chest tightness associated with dyspnea during a session of hemodialysis. He denied fever, chills, vomiting, abdominal pain, tarry or bloody stool. Unfortunately, respiratory failure was developed after admission, he was intubated.

Relevant Test Results Prior to Catheterization
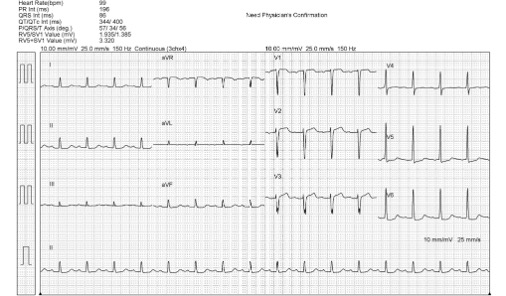
The Laboratory data revealed elevated NTproBNP(>70000 pg/ml) and Troponin-I level (32 ng/ml). Pulmonary edema was noted on Chest X-ray (picture as above). The electrocardiogram (ECG) which showed normal sinus rhythm without obvious ST segment elevation. Non-ST-Elevation Myocardial Infarction was diagnosed.
Relevant Catheterization Findings
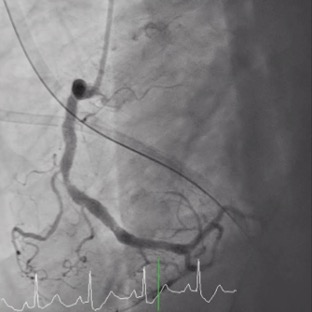
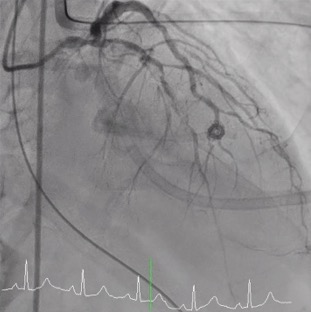
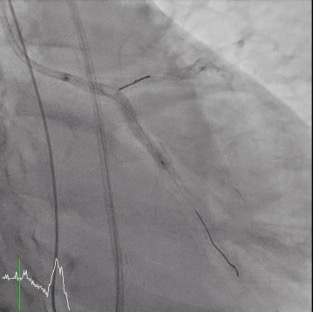
Coronary angiography(CAG) was done and showed Right Coronary artery(RCA) segment 2 70% stenosis, 75% stenosis at distal Left Main coronary artery(LM) and 90% stenosis at middle Left Anterior Descending artery (LAD), along with a 90% stenosis at the Left Circumflex artery (LCX) orifice. Due to the patient could only afford one Drug-Eluting Stent(DES), so our initial strategy: a Bare-Metal Stent(BMS) at the middle part of LAD and one DES stent crossing over LM-LAD with final kissing.
Interventional Management
Procedural Step
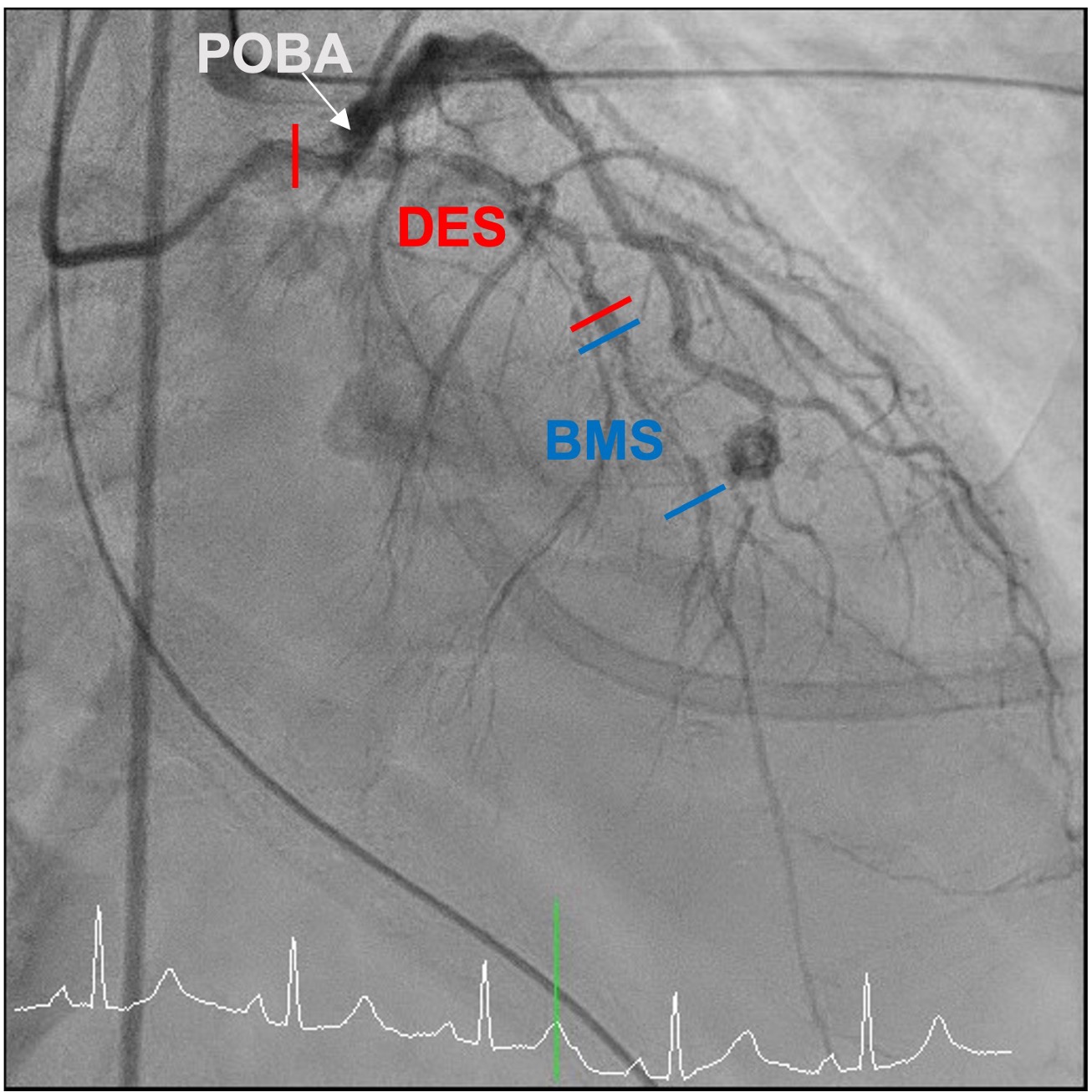
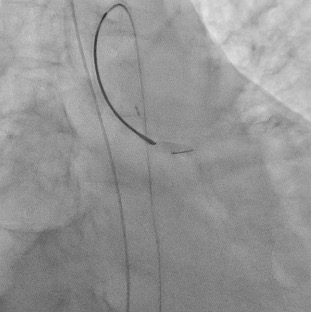
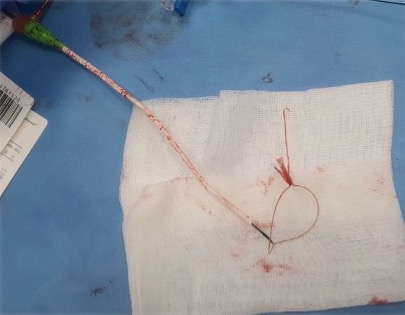
Percutaneous coronary intervention (PCI) was initiated by a right femoral approach using a 7 Fr EBU 3.5 guide catheter. We started from NC balloon and cutting balloon for lesion preparation, then first BMS was deployed successfully but the 3.5 X 48mm DES was hard to push even by side branch and distal anchor technique. We changed our strategy from 1 long stent to 2 shorter stent with a shorter DES and it work. But, due to the jailed LCX orifice, the reversed culotte technique was used with the opened 48mm DES at the beginning as bail out 2 stent strategy. We were able to deployed the opened 48mm DES at the LM-LCX successfully, however, the balloon could not be deflated and was stuck! We hurriedly tried the opened cutting balloon and back-and-forth traction but failed. Even worse, the balloon shaft snapped! We tried to engage the guiding to catch the balloon but failed again. Overall, this was a catastrophe with an un-deflated fractured balloon trapped and stuck at the left main coronary artery.The patient complained of severe chest pain accompanied by a dropping blood pressure. We administered Bosmin with Levophed pump for the shock status and contacted the Cardiovascular surgeon and ECMO team immediately. For our last resort, we tried the Snare to catch the proximal tip of the undeflated fractured balloon and finally we succeeded. We were able to capture the balloon and retrieve it, with the angiography resulted expanded stent with normal coronary flow.
 Snare retrive undefalted stent ballon .mp4
Snare retrive undefalted stent ballon .mp4
Case Summary
Balloon entrapment is an uncommon complication during PCI. We can try gentle traction if deflation is possible, and advance another guide extensor for retrieval. But if the balloon fails to deflate, with balloon shaft fracture. This is even rare and one of the most dreaded complications, especially at the left main, which can occlude coronary flow, causing myocardial infraction, shock, and even death. If such an unfortunate event occur, stay calm then stabilize the hemodynamics (including vasopressor, IABP, ECMO). Several percutaneous maneuvers (ex. Snare) can be tried, and do not hesitate to contact the surgeons for emergent operation if the efforts fail.