Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251029_001
Bridging an Aneurysmal Coronary Segment With Drug-Eluting Stents: A Pragmatic Percutaneous Coronary Intervention Strategy for Non-ST-Elevation Myocardial Infarction in a Resource-Limited Setting
By Muhammad Husen Latief
Presenter
Muhammad Husen Latief
Authors
Muhammad Husen Latief1
Affiliation
Siloam Hospital Makassar , Indonesia1
View Study Report
CASE20251029_001
Coronary - ACS/AMI
Bridging an Aneurysmal Coronary Segment With Drug-Eluting Stents: A Pragmatic Percutaneous Coronary Intervention Strategy for Non-ST-Elevation Myocardial Infarction in a Resource-Limited Setting
Muhammad Husen Latief1
Siloam Hospital Makassar , Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
A 52-year-old man presented with 4-hour retrosternal chest pain radiating to the left arm, pressure-like and persistent, associated with mild diaphoresis. He had hypertension and dyslipidemia with poor medication adherence, no diabetes, smoking, or prior coronary disease. On examination, he was stable but tachycardic (BP 132/84 mmHg, HR 120 bpm), afebrile, with normal heart sounds, clear lungs, no edema, and no signs of heart failure.
Relevant Test Results Prior to Catheterization
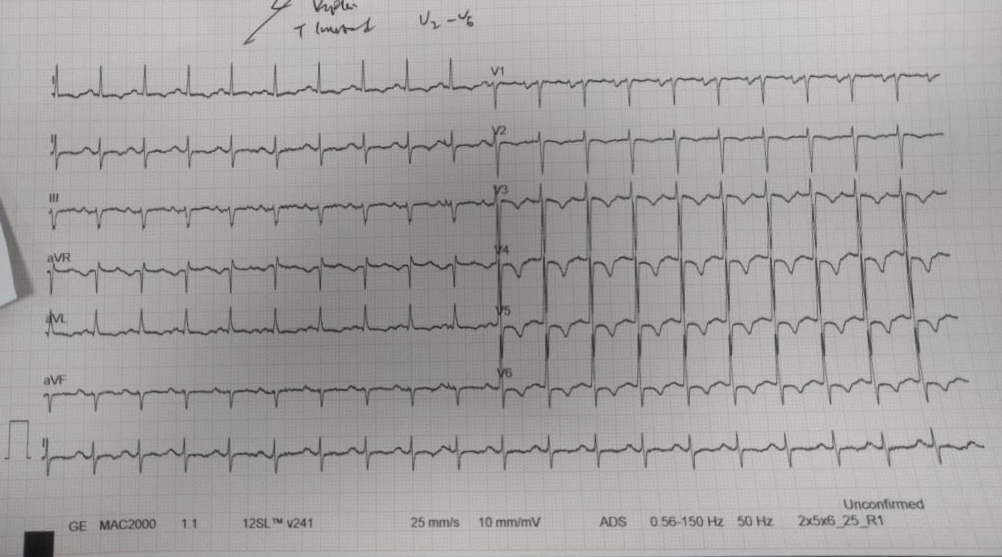
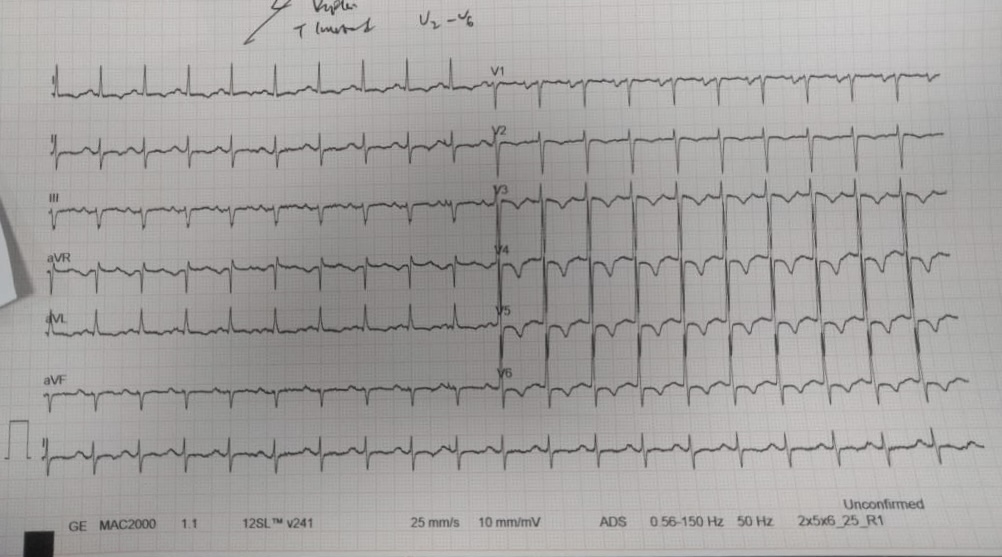
ECG showed 1–2 mm ST depression with T-wave inversion in leads V3–V6, consistent with anterior ischemia. High-sensitivity troponin I was elevated at 1.2 ng/mL and rising. Chest X-ray was normal. Echocardiography showed mild LV systolic dysfunction (EF 50%) with anterior hypokinesia. Renal function and electrolytes were within normal limits.
Relevant Catheterization Findings
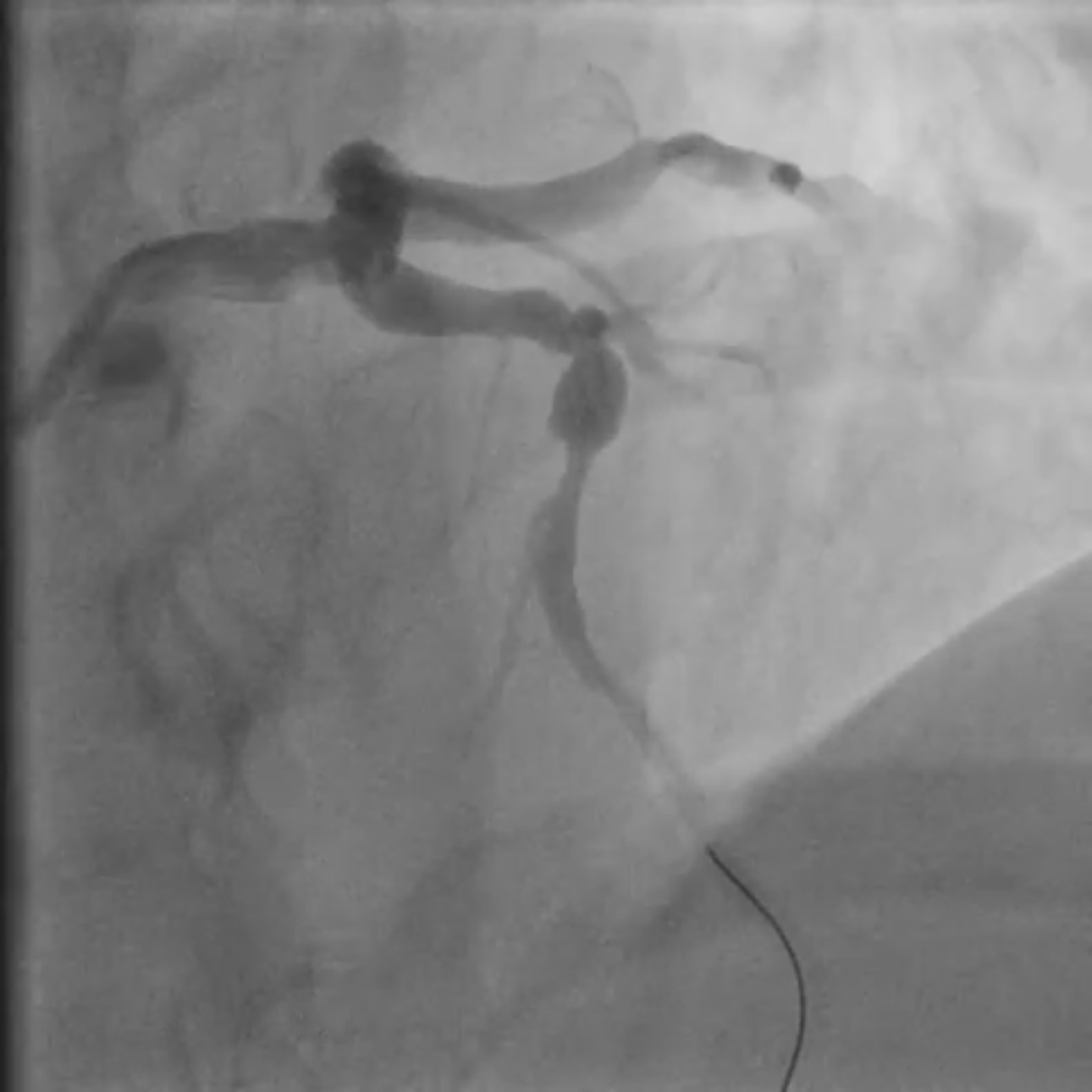
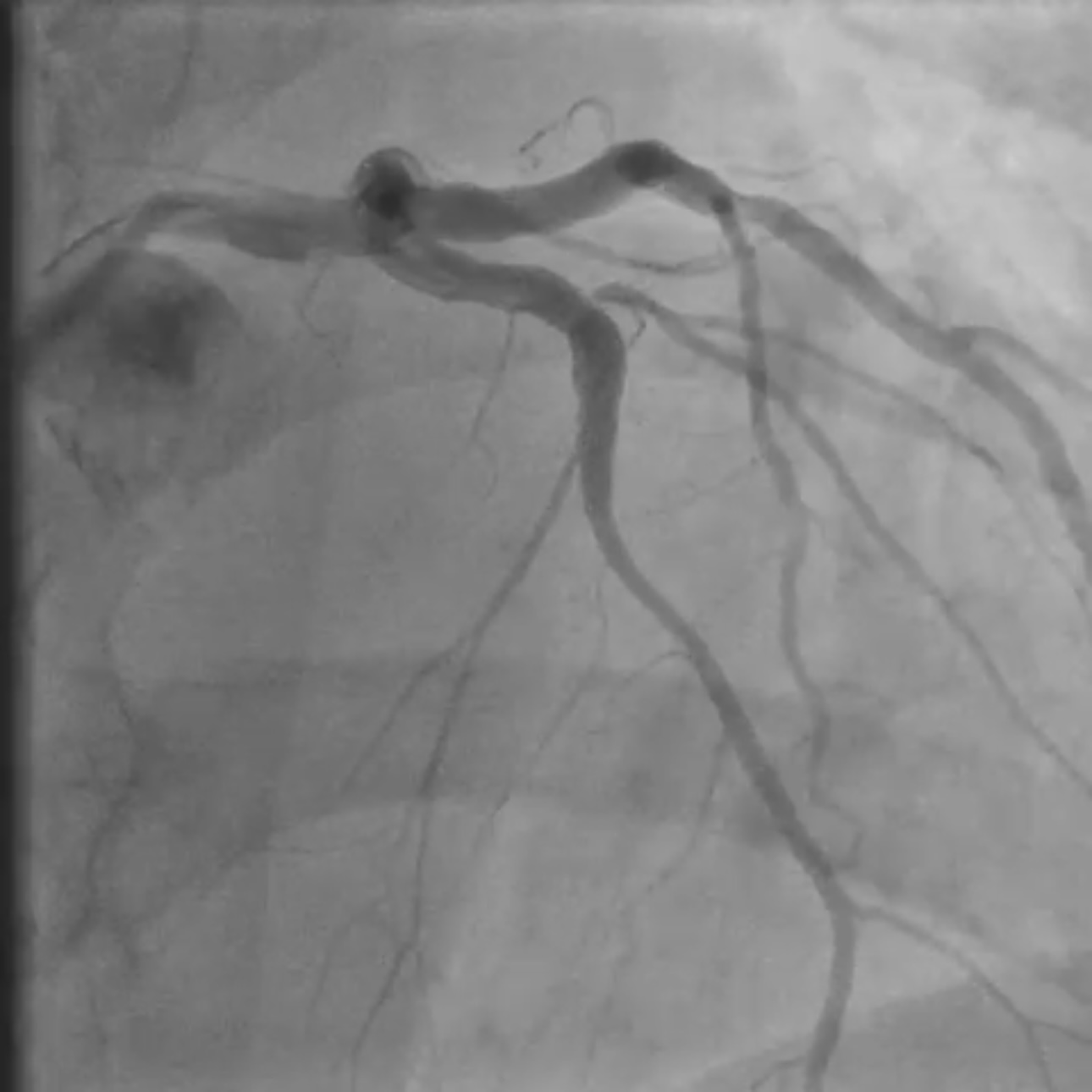
Coronary angiography revealed two severe stenoses in the mid left anterior descending (LAD) artery, separated by a short fusiform aneurysmal segment. The aneurysm was located between diseased segments and measured approximately 6 mm in diameter. A diagonal branch originated close to the proximal edge of the aneurysm. No thrombus or flow limitation was seen, and TIMI 3 flow was maintained pre-intervention.
 95633e10-0452-4706-b391-261f2bea569e.mov
95633e10-0452-4706-b391-261f2bea569e.mov
95633e10-0452-4706-b391-261f2bea569e.mov
95633e10-0452-4706-b391-261f2bea569e.mov
Interventional Management
Procedural Step
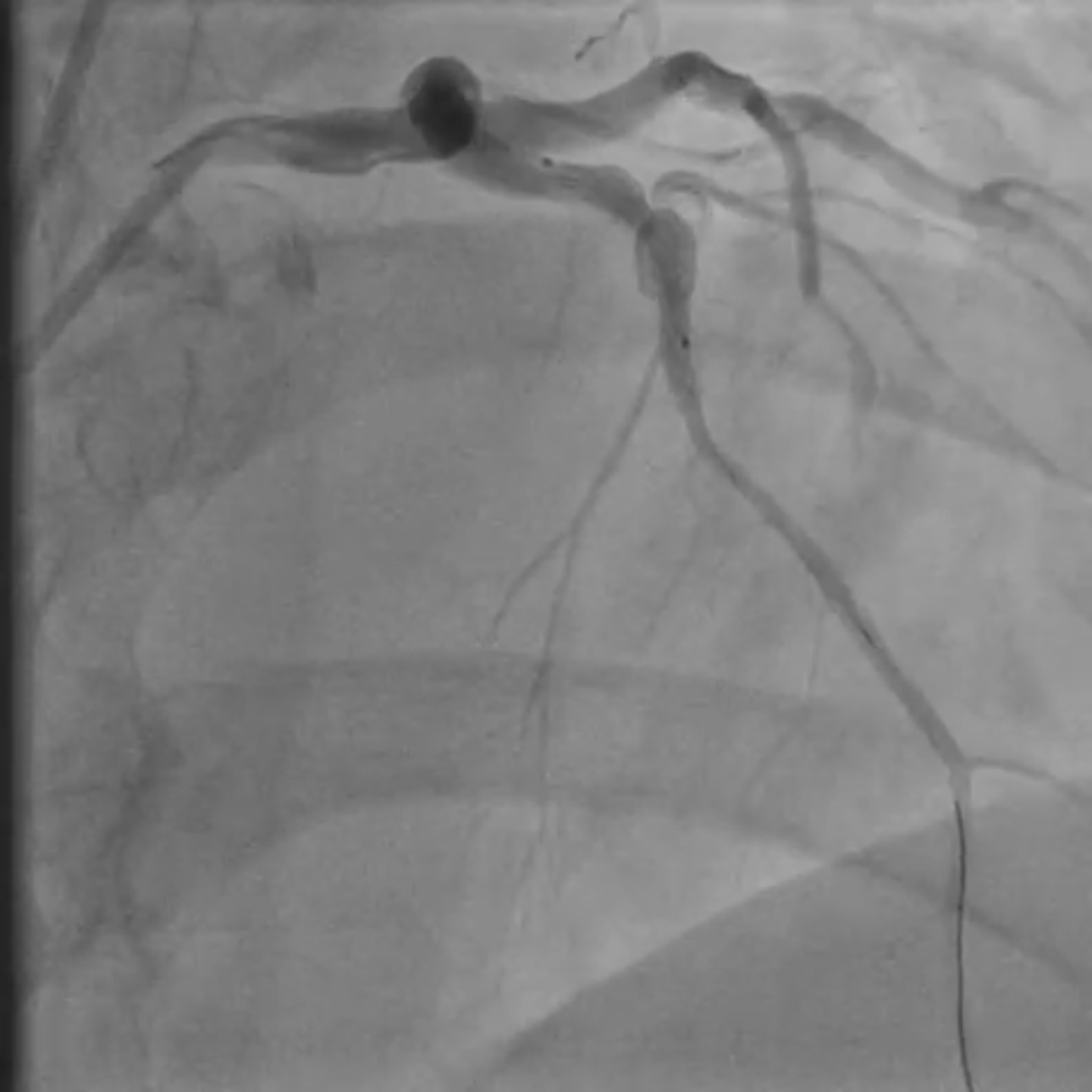
Coronary angiography revealed two critical stenoses in the mid–left anterior descending (LAD) artery separated by a short fusiform aneurysmal segment. A diagonal branch originated near the proximal aneurysm margin. Implanting a covered stent was avoided due to the high risk of diagonal branch occlusion, and a drug-eluting balloon (DEB) strategy was rejected because it offered no vessel scaffolding and could destabilize the aneurysmal wall. A dual drug-eluting stent (DES) bridging technique was selected to stabilize the aneurysmal segment while maintaining branch perfusion. The procedure was performed via right radial access using a 6F XB guide catheter for enhanced support. A floppy guidewire was advanced into the distal LAD. Lesion preparation was performed with a 2.5 mm semi-compliant balloon. A 3.0 × 15 mm DES was first deployed distally to treat the distal stenosis and establish a stable anchoring platform on healthy vessel. A second DES (3.5 × 22 mm) was then implanted across the aneurysmal segment, with distal overlap onto the first stent to secure the construct outside the aneurysm. The proximal landing zone was carefully positioned in healthy vessel proximal to the aneurysm. Post-dilatation was deliberately limited to the landing zones with a non-compliant balloon to minimize mechanical stress on the aneurysmal wall. Final angiography showed optimal stent expansion, preserved flow to the diagonal branch, no dissection or perforation, and TIMI 3 flow. The patient received unfractionated heparin during PCI and dual antiplatelet therapy (aspirin + ticagrelor) per ACS guidelines.

95633e10-0452-4706-b391-261f2bea569e.mov
95633e10-0452-4706-b391-261f2bea569e.mov
95633e10-0452-4706-b391-261f2bea569e.mov
Case Summary
This case demonstrates that percutaneous treatment of a stenotic segment with an intervening coronary aneurysm can be performed safely with a sequential DES-bridging strategy when covered stents are not feasible due to side-branch involvement. Drug-eluting balloon therapy alone was inadequate as it offered no structural support. Anchoring both stents on healthy vessel segments and avoiding aggressive dilation within the aneurysm provided vessel stability, preserved diagonal branch flow, and achieved excellent procedural success in a resource-limited setting.