Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251028_004
From Stonewall to Stent: ELCA as a Bailout Strategy for Rota-Burr Uncrossable Lesion
By Alvin Brilian Budiono, Wei Wang
Presenter
Alvin Brilian Budiono
Authors
Alvin Brilian Budiono1, Wei Wang2
Affiliation
Primaya Hospital Makassar, Indonesia1, Wuhan Asia Heart Hospital, China2
View Study Report
CASE20251028_004
Coronary - Complex PCI - Calcified Lesion
From Stonewall to Stent: ELCA as a Bailout Strategy for Rota-Burr Uncrossable Lesion
Alvin Brilian Budiono1, Wei Wang2
Primaya Hospital Makassar, Indonesia1, Wuhan Asia Heart Hospital, China2
Clinical Information
Relevant Clinical History and Physical Exam
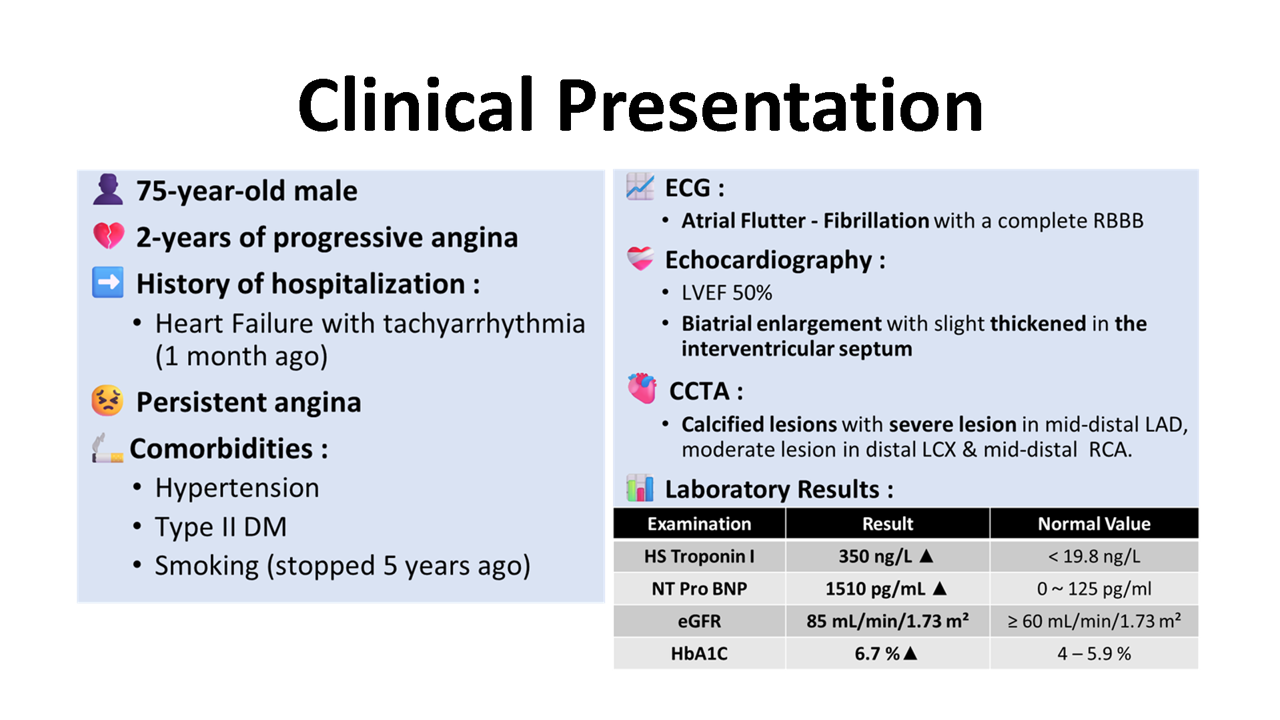
A 75-year-old male presented with persistent angina since 2-years. He had comordibities of hypertension, type 2 diabetes, and a smoking history. He was recently hospitalized for heart failure with tachyarrhythmia. Medications were fosinopril, furosemide, spironolactone, andrivaroxaban.
Relevant Test Results Prior to Catheterization
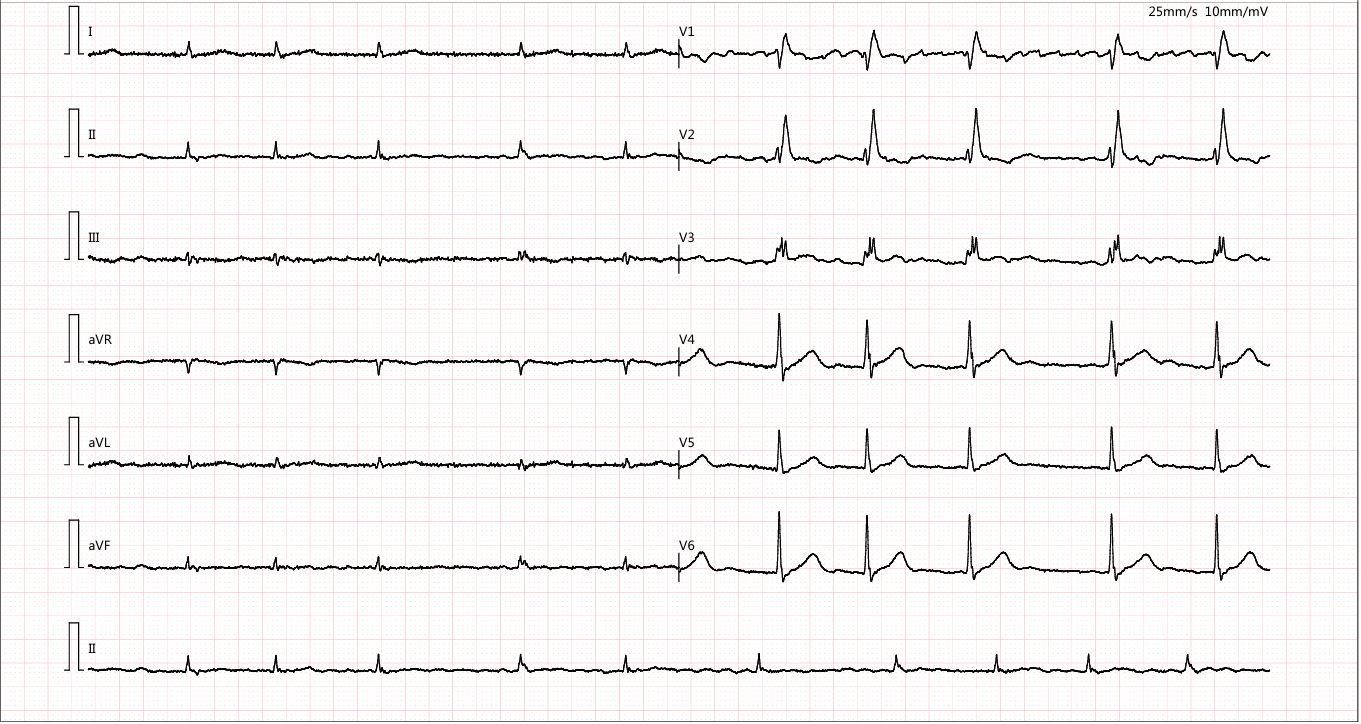
ECG showed Atrial Flutter-Fibrillationwith a complete RBBB. Echocardiography revealed LVEF 50%, biatrial enlargementwith slight thickened in the interventricular septum, mild mitralregurgitation, and severe tricuspid regurgitation. CCTA identified heavilycalcified plaques in LAD, LCX, and RCA.
Relevant Catheterization Findings
Diagnostic angiography revealed 95%stenosis in mid & distal LAD, 80% stenosis in proximal OM4, and 60%stenosis in distal RCA with calcification.
 CAG1.mp4
CAG1.mp4
CAG2.mp4
CAG3.mp4
Interventional Management
Procedural Step
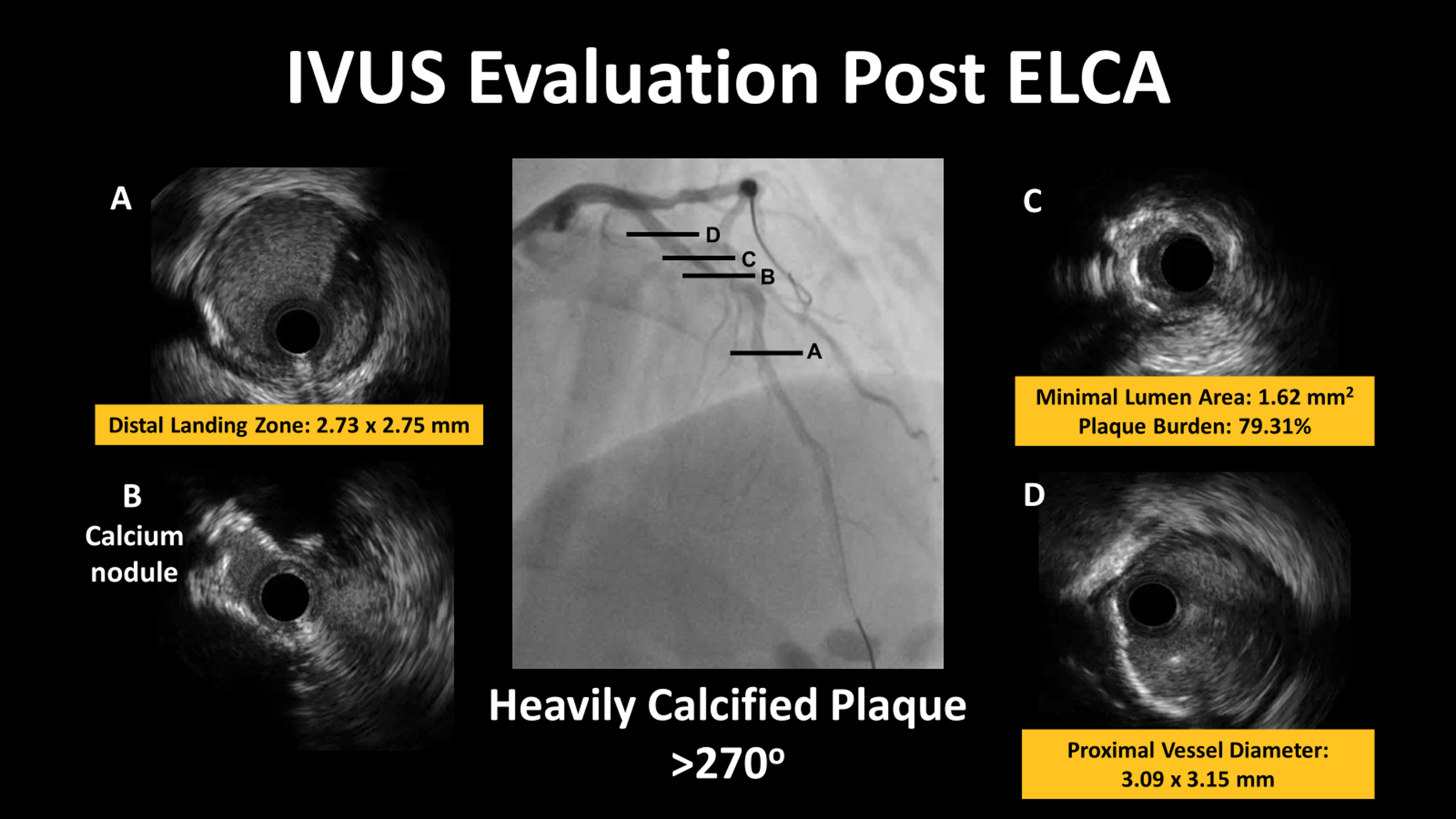
PCI was initiated with prophylactic IABP via a 7Fr EBU 3.5 guide. A guidewire crossed the lesion, but a 2.0/20mm balloon failed. A 1.5/15mm balloon predilated at 16 atm, yet larger balloons remained uncrossable and angiography showed no improvement. The procedure was complicated by chest pain, hypotension, and ST-segment elevation, prompting urgent IABP initiation.
PRE PCI.mp4
ROTA FAILED.mp4
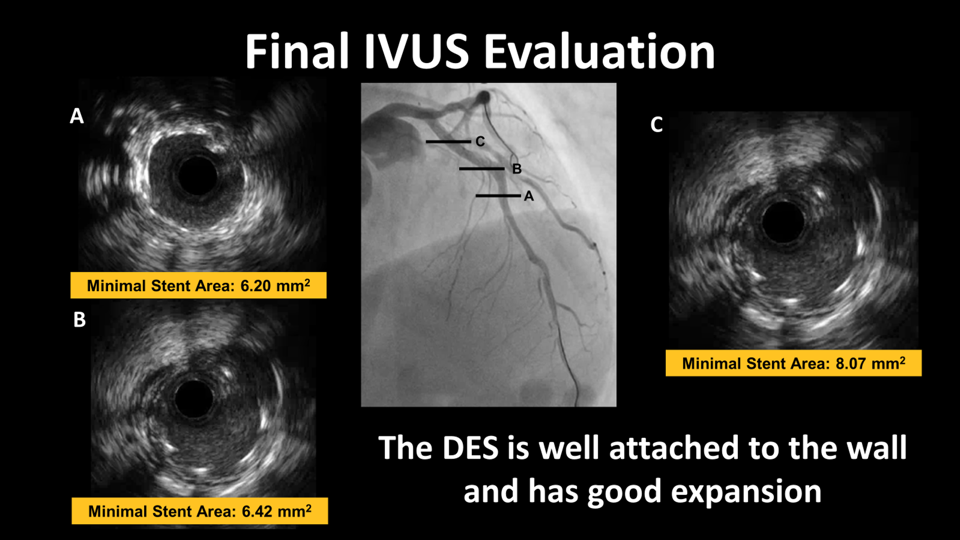
FINAL VIDEO.mp4