Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251028_001
Step-Down Rota Burr Strategy in Calcific Lesion
By Sourabh Agstam, Sandeep Seth
Presenter
Sourabh Agstam
Authors
Sourabh Agstam1, Sandeep Seth1
Affiliation
AIIMS, New Delhi, India1
View Study Report
CASE20251028_001
Coronary - Complex PCI - Calcified Lesion
Step-Down Rota Burr Strategy in Calcific Lesion
Sourabh Agstam1, Sandeep Seth1
AIIMS, New Delhi, India1
Clinical Information
Relevant Clinical History and Physical Exam
• A 64-year-old gentleman, a known case of diabetes, hypertension, had IWMI (2009) followed by
O
Relevant Test Results Prior to Catheterization
Two-dimensional echocardiography showed Normal left ventricle systolic function. Laboratory parameters were in normal range.
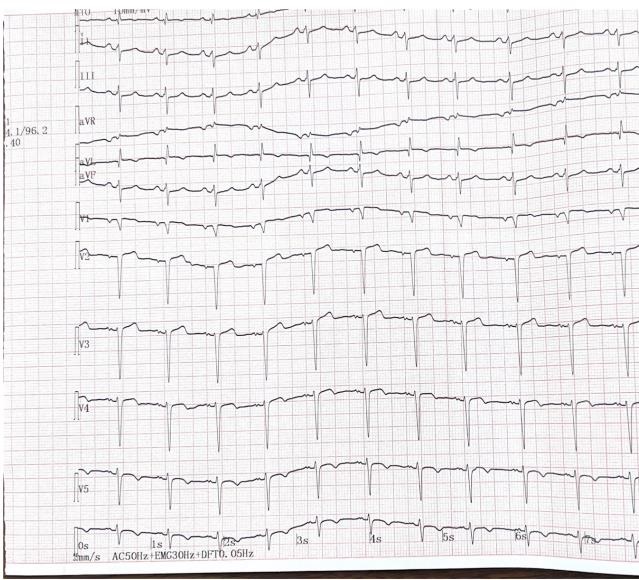
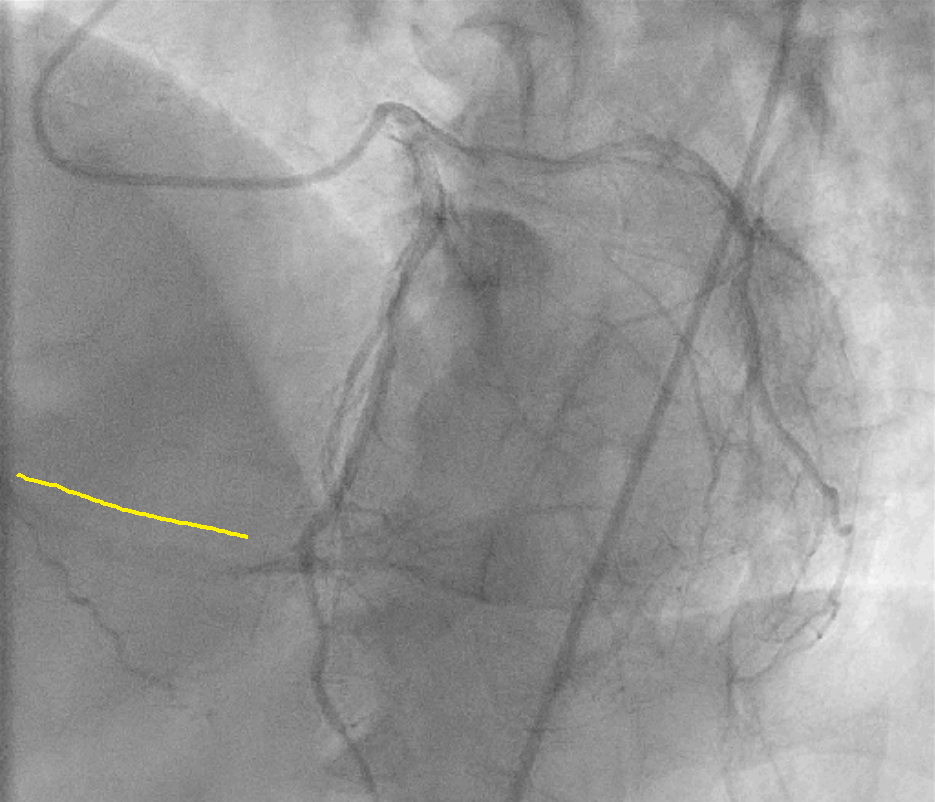
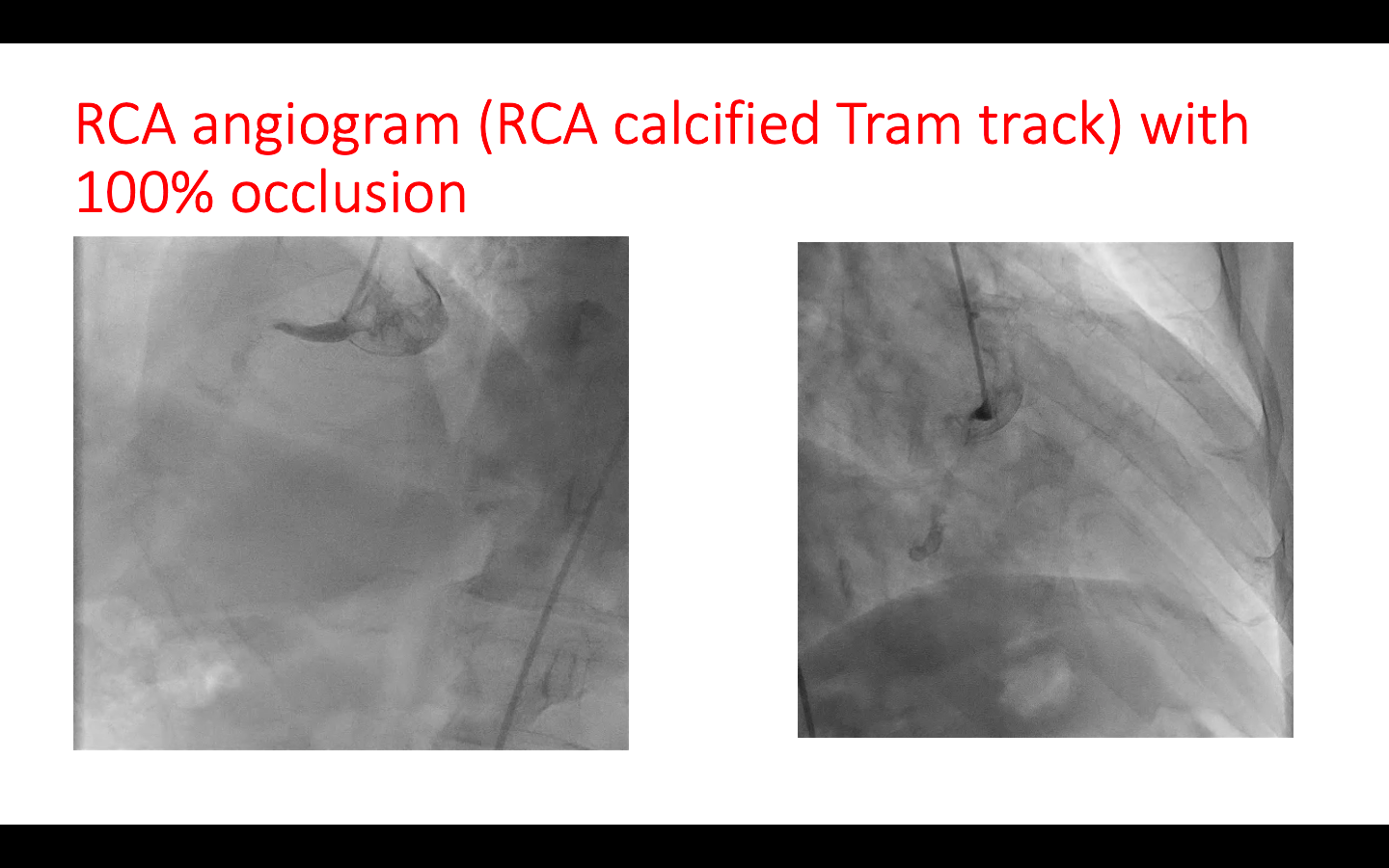
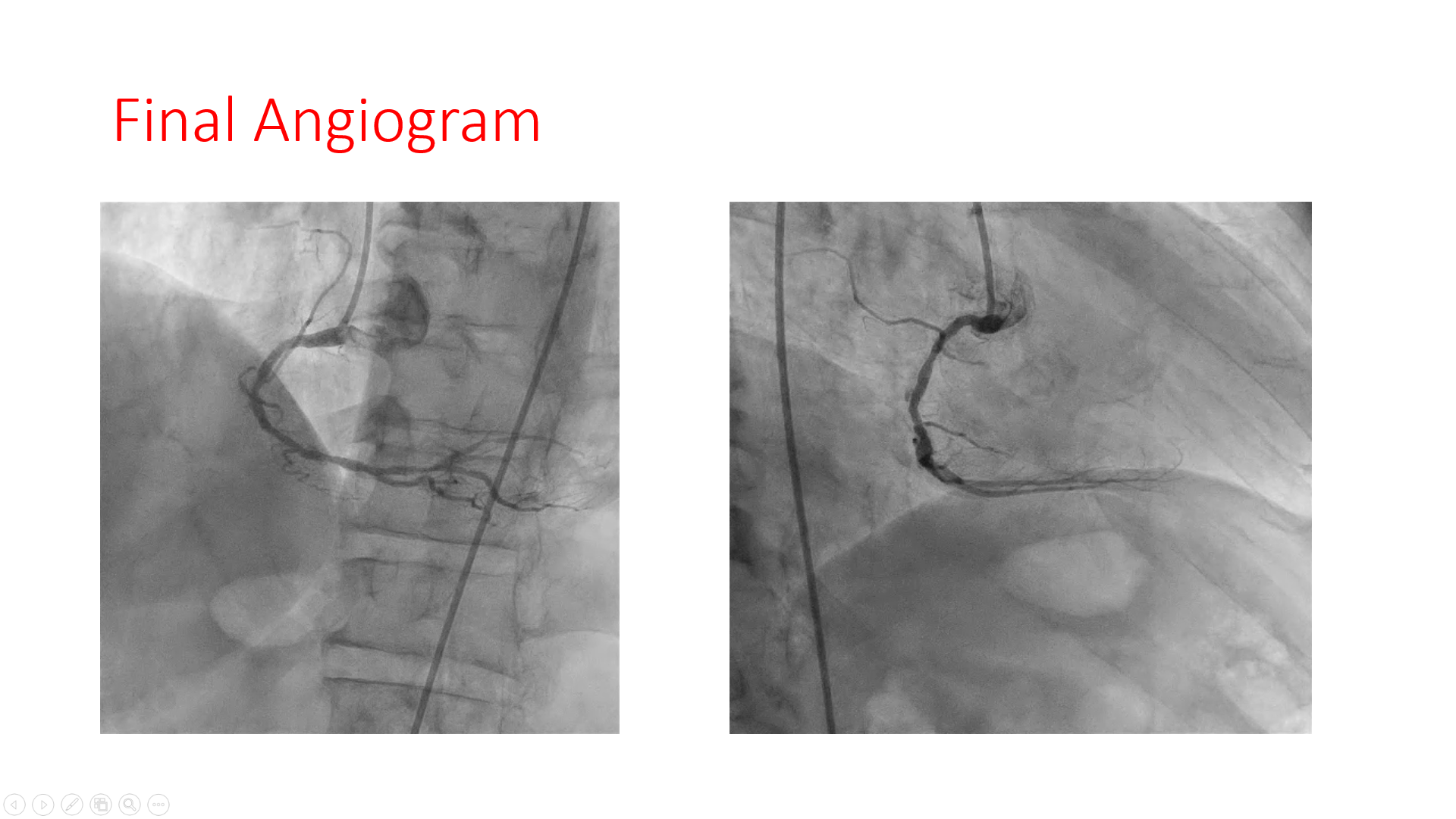
Relevant Catheterization Findings
Angiogram suggestive of patent stents in LAD and LCX; and dominant right coronary artery with proximal cut off along with tram track calcification. The RCA is filling distally by retrograde collaterals Rentrop III.
 mov-00001.avi
mov-00001.avi
mov-00005.avi
Video 1.mp4
Interventional Management
Procedural Step
7F Femoralapproach and AL 0.75 was taken.
video 2.mp4
Video 3.mp4
mov-00024.avi
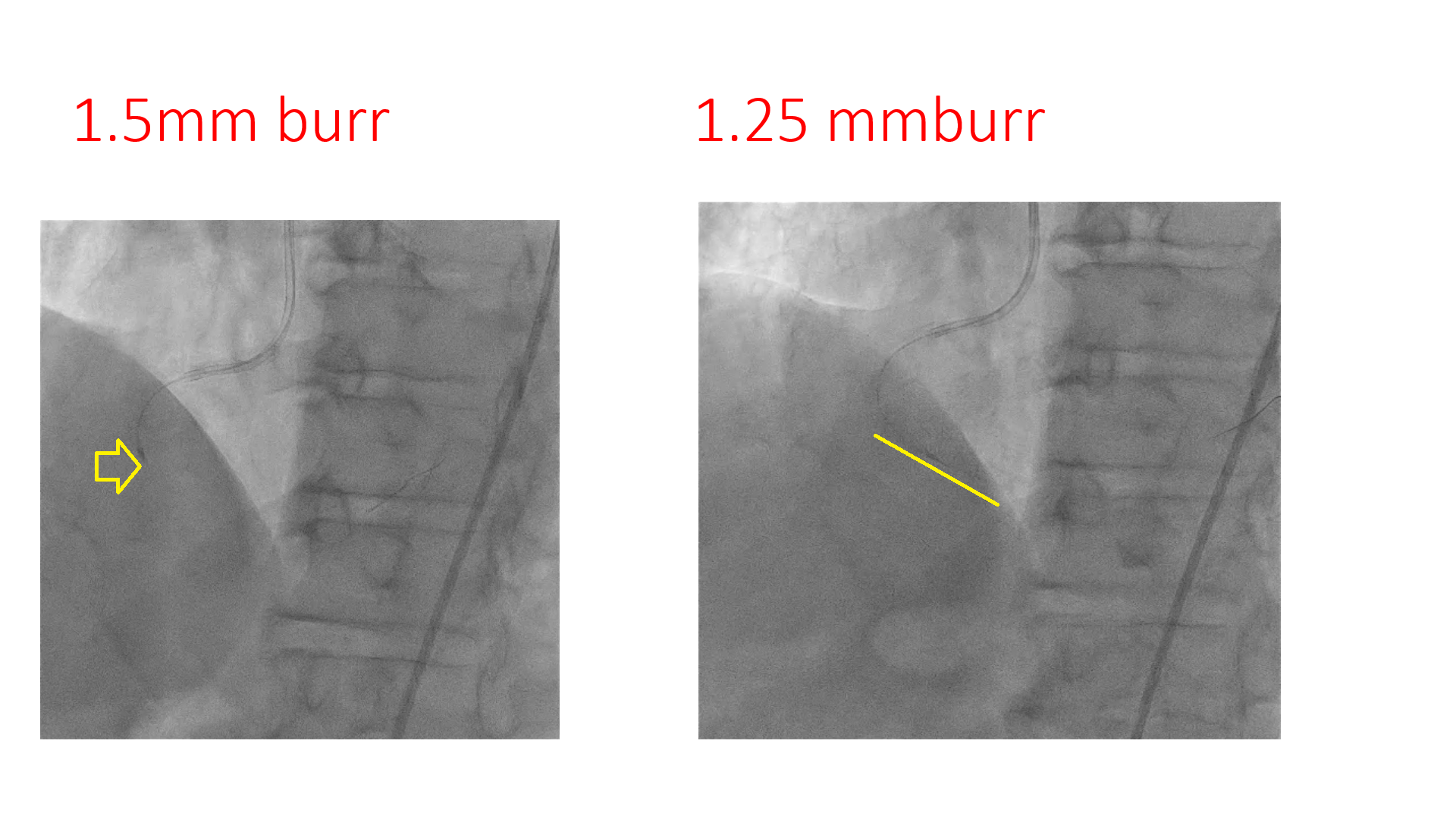
Case Summary
Step-down Rota burr strategy should be done early, in case of difficulty with regular burr. Tortuosity in vessel predisposes to wire bias in rotablation. Changing the wire to extra support or reducing the burr size: what should be done ideally and always matter of discussion.